
Abstract
Objective:
People with diabetic peripheral neuropathy (DPN) have impaired gait and balance performance. The aim of this study is to investigate therapeutic effectiveness of mechanical stimulation through a wearable foot compression device equipped in a shoe insole on vibration perception, balance control and gait performance in people with DPN.
Methods:
Using a single-arm 4-week intervention study design, we examined effectiveness of daily use of shoes equipped with the foot compression device (Footbeat™, AVEX, Grand Junction, CO, USA) on improving vibration perception threshold (VPTmax), skin perfusion pressure (SPP), ankle brachial index (ABI), lower extremities edema (circumferences in the calf and ankle), and motor performance (postural sway with eyes open and closed conditions, and gait performance during normal, dual-task and fast walking). Thirty people with type 2 diabetes and symptoms of PN completed the experimental protocol.
Results:
Improvements in VPTmax (before = 27.4 V, after = 23.3 V, P = .007, d = 0.33, where d denotes effect size), center-of-mass sway in the mediolateral direction with both eyes open and closed conditions (before = 0.94 cm, after = 0.76 cm, P = .020, d = 0.47; before = 1.10 cm, after = 0.83 cm, P = .033, d = 0.66, respectively), and stride velocity for normal walking, dual-task walking and fast walking tasks (before = 0.87 m/s, after = 0.96 m/s, P = .017, d = 0.41; before = 0.75 m/s, after = 0.91 m/s, P = .001, d = 0.77; before = 1.10 m/s, after = 1.20 m/s, P = .043, d = 0.33, respectively) were found post treatment. There was no significant improvement in SPP, ABI, and circumferences in the calf and ankle.
Conclusions:
Our findings suggest the wearable foot compression device may be effective for reducing neuropathic symptoms and enhancing motor performances in people with DPN.
In the United States, more than 30 million people suffer from diabetes, and every year 1.5 million people are newly diagnosed with diabetes. 1 Diabetic peripheral neuropathy (DPN), nerve damage, is a major diabetic complication, affecting between 30 and 50% of people with diabetes at all ages, 2 and a leading risk factor for foot ulcer, infection, and amputation. 3 One common problem in DPN is diminished sensation particularly in the lower extremity due to damaged nerve. 4 This results in lack of sensorimotor communication with the central nervous system during locomotor tasks such as gait and balance control during quiet standing. In fact, several studies have documented gait abnormalities and postural instability associated with DPN.5-10 For example, people with DPN have larger postural sway during quiet standing compared to people with diabetes and no neuropathy, and healthy people. 5 Also, people with DPN have slower gait speed compared to healthy people. 7 These impairments in locomotor tasks are likely to indicate increase in risk of injury during locomotion such as falling,11,12 and low quality of life and high morbidity and mortality in people with diabetes. 13 Therefore, it is important to treat DPN properly and prevent worsening of its symptoms.
It is well established that nonsurgical and nonpharmacological interventions may be an effective adjunct to pathophysiological and/or motor symptoms of DPN. It was reported that, in people with DPN, aerobic exercise intervention improves balance control and gait speed, 14 and exercise intervention specifically focusing on ankle movement (ie, balance training) improved balance control.15,16 In addition, previous studies demonstrated that use of ankle-foot orthoses or off-loading devices improves wound healing,17-19 balance control, 20 and gait stability. 21 Also, several studies investigated the effect of electrical stimulation as an adjunctive therapy,12,22,23 and reported improvement in wound healing, 22 plantar sensation in the foot and balance control,12,23 and gait speed 12 in people with DPN after receiving electrical stimulation. Although these studies reported positive results for the management of DPN, fundamental barriers such as reluctance to exercise, 24 discomfort in wearing an exoskeleton25,26 and electrical stimulation devices, 26 and the relatively high cost of electrical stimulation may limit the effectiveness of such treatments.
In addition to these interventions, a few studies have reported that mechanical stimulation applied to the bottom of the foot through vibrating insoles may be effective for enhancing plantar sensation in the foot27-29 and balance control for people with DPN.30,31 These studies only reported the effect of mechanical stimulation on plantar sensation or balance control. However, their findings together with its effectiveness on gait and balance in healthy older adults reported in another study 32 have predicted the possibility of potent effects of mechanical stimulation on sensation, gait and balance control in people with DPN. Furthermore, recent development in micro-mobile compression devices installed in shoe insoles has enabled mechanical stimulation on the plantar surface of the foot during day-to-day activities without additional discomfort. 33 However, its effectiveness on pathophysiology and motor symptoms in people with DPN has not yet been tested. Therefore, the aim of this study was to evaluate the effect of mechanical stimulation through micro-mobile foot compression devices installed in shoe insoles on vibration perception, balance control, and gait performance in people with diabetes. Based on prior findings, we hypothesized that daily use of the wearable foot compression device would improve vibration perception. In addition, it was hypothesized that the improvements in vibration perception would lead to improvements in balance outcomes and gait parameters.
Methods
Participants
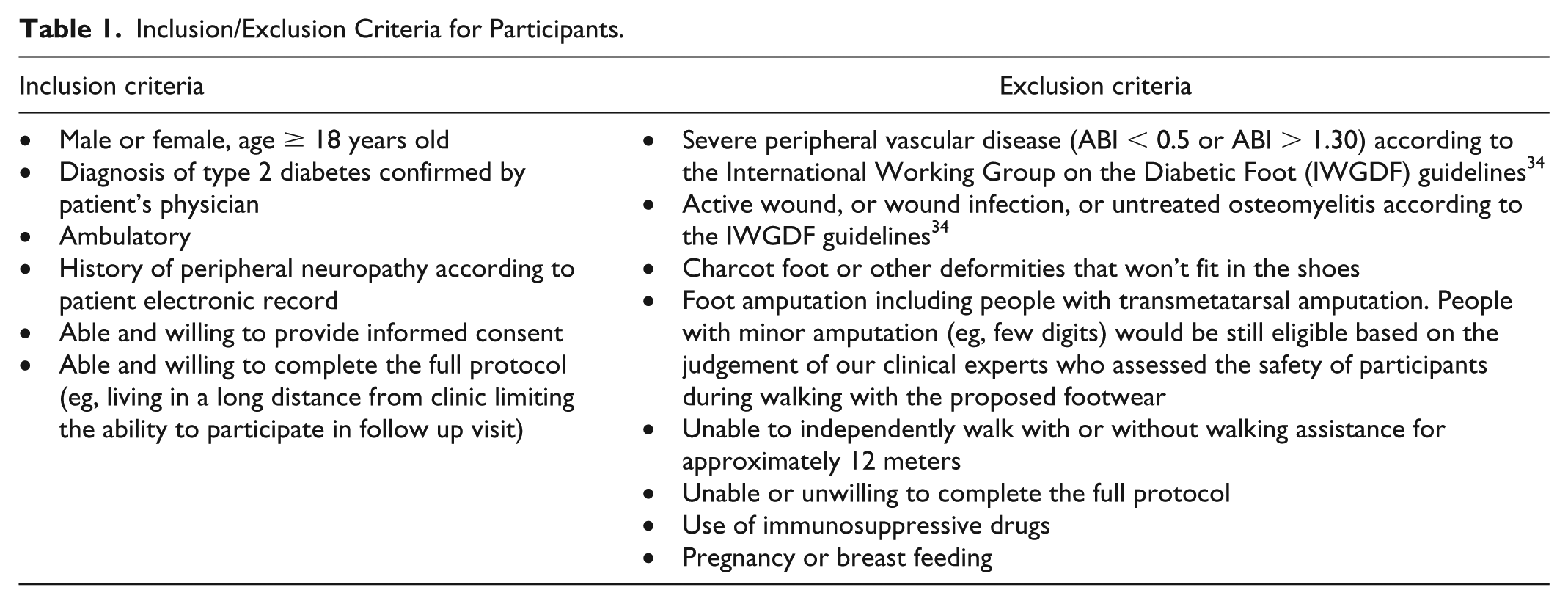
We recruited a convenience sample of 30 people with type 2 diabetes in this study. Potential participants were screened for eligibility based on the inclusion and exclusion criteria described in Table 1. 34 We recruited participants from the Baylor College of Medicine, outpatient clinics and senior centers in the greater Houston area via their physicians’ referrals or advertisements. All participants provided written informed consent approved by the Baylor College of Medicine Institutional Review Board prior to participating in the experimental protocol. This study was registered in ClinicalTrials.gov, identifier NCT03135535.
Inclusion/Exclusion Criteria for Participants.
Device
In this study, an FDA cleared micro-mobile foot compression device installed in shoe insoles (Footbeat, AVEX LLC, Grand Junction, CO, USA) was used (Figure 1). The foot compression device is composed of a rechargeable motorized thrusting arm and pressure pad (18.6 cm2). It was designed to push the arch of the plantar surface of the foot with a pressure of 3.76 N/cm2 every 35 seconds while participants were sitting or lying down, which empties the plantar venous plexus and accelerates blood flow in the lower extremity (Figure 1). 33 The foot compression device was automatically deactivated when it senses standing or walking (ie, when it senses more plantar pressure). We provided each participant with a pair of shoes (Dr. Comfort LLC, Mequon, WI, USA) equipped with the insoles with the micro-mobile foot compression device. The tightness of the shoes was adjusted using a reel clutch (BOA Technology Inc, Denver, CO, USA). 35 We asked participants to wear the shoes for at least four hours a day for a period of four weeks based on the minimum battery life of the foot compression device when the system was continuously activated. The average time of wearing the shoes and the average time of the compression device activation across participants were 5.4 ± 2.0 and 5.2 ± 2.0 hours, respectively.
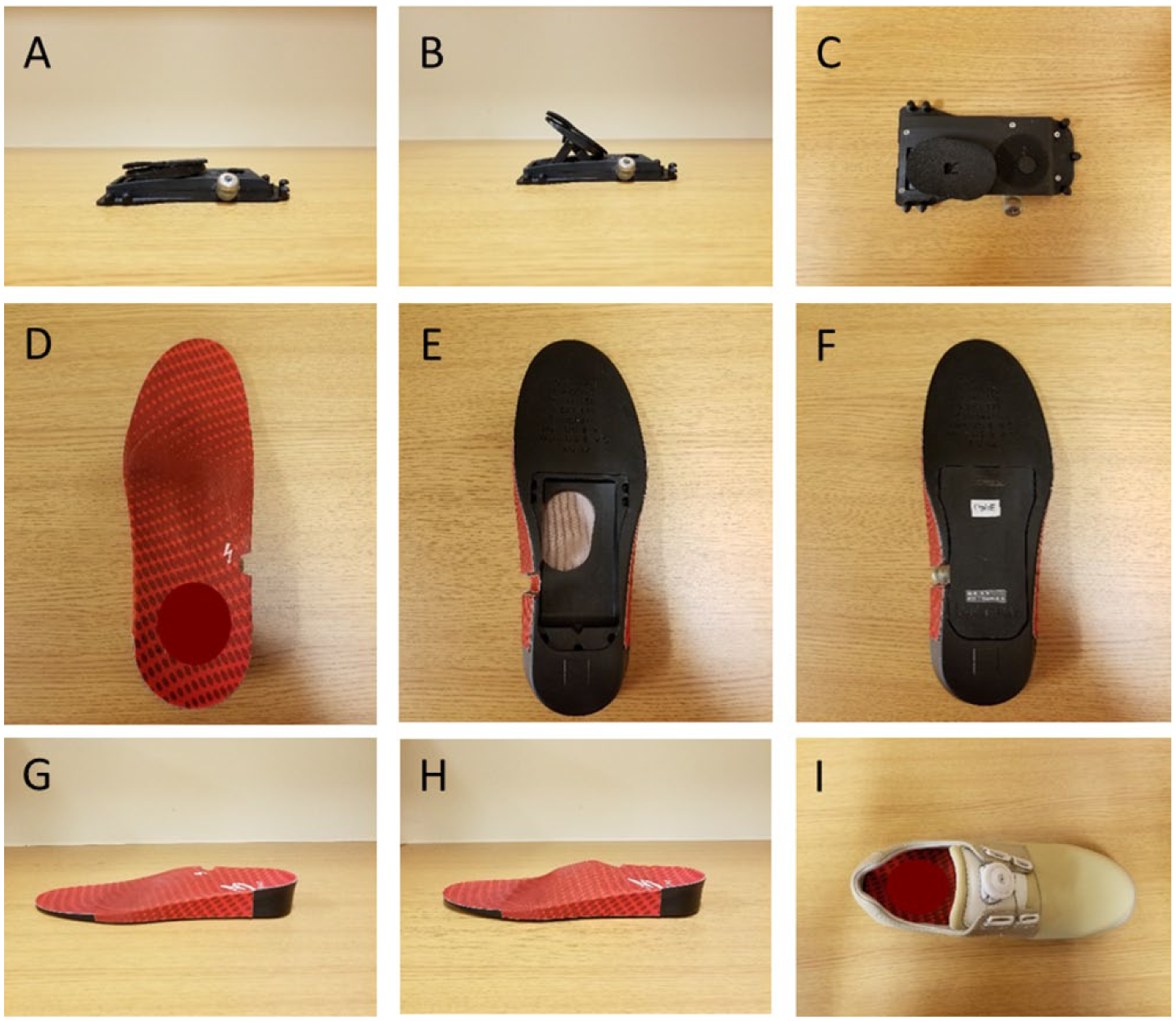
Illustrations of the foot compression device, insole and shoe that were used in this study: (A) side view of the foot compression device with the thrusting arm and pressure pad when resting,; (B) side view of the foot compression device with the thrusting arm and pressure pad when pushing; (C) top view of the foot compression device with the thrusting arm and pressure pad when pushing, (D) top view of the top side of the insole; (E) top view of the bottom side of the insole before installing the foot compression device; (F) top view of the bottom side of the insole after installing the foot compression device; (G) side view of the insole with the thrusting arm and pressure pad when resting; (H) side view of the insole with the thrusting arm and pressure pad when pushing; and (I) top view of the shoe equipped with the insole.
Experimental Protocol and Outcomes
We used a single-arm 4-week intervention study design of daily use of plantar mechanical stimulation. At baseline, we collected participant characteristics including age, body mass index (BMI), sex, the number of prescribed and over-the-counter medications, comorbidities, and deformities in the foot, skin (eg, flaky, calluses, warts) and nail (discolored, missing, dystrophic/fungal). 36 In addition, we assessed each participant’s depressive state using the Center for Epidemiological Studies Depression Scale (CES-D), 37 cognitive function using the Montreal Cognitive Assessment (MoCA) 38 and frailty status using the Fried Frailty Criteria. 39 Functional characteristics such as fall history, daily activities level and mobility-related fatigue were assessed using self-disclosure, the Barthel Index of Activities of Daily Living (ADL) 40 and the Mobility Tiredness Scale, respectively. Other functional characteristics such as timed up and go test (TUG) and four step square test (FSST) were assessed using two wearable sensors (LegSys™, BioSensics, Watertown, MA, USA). Also, we assessed fear of falling using the Falls Efficacy Scale–International (FES-I) 41 and pain level in the foot using the Virtual Analog Scale (VAS).
We performed several clinical assessments at baseline and conclusion of the intervention. We measured vibration perception threshold (VPT) for assessing severity of neuropathic symptoms, skin perfusion pressure (SPP) and ankle brachial index (ABI) for assessing peripheral vascular status, and circumferences in the calf and ankle for assessing lower extremity edema. We measured VPT at the first and fifth metatarsal head and heel in the plantar surface of both feet using a Biothesiometer (Bio-Medical Instrument Co, Newbury, OH, USA) as indicated in previous studies.12,42 Briefly, we had placed the probe of the Biothesiometer on one of the sites in the plantar surface of the foot for a participant, and had gradually increased the magnitude of electrical vibration from 0 V until the participant responded “I am feeling the vibration now”. To confirm the threshold for perception of sensation, we had increased the voltage from the participant self-reported value and then gradually reduced until the participant responded “I am not feeling the vibration now”. If the two values were close (< 2 V difference), the max value was considered as VPT. Otherwise, the process was repeated. Then, we repeated this method for the other sites for the participant. We defined VPTmax as maximum measured VPT values from all sites from both feet. A cutoff of equal or greater than 25 V43-45 was used to distinguish between those with severe (severe PN: VPT ≥ 25 V) and mild PN (mild PN: VPT < 25 V). We measured ABI and SPP using PAD-IQ (VÄSAMED, Eden Prairie, MN, USA).
We measured balance characteristics using two validated wearable sensors (BalanSens™, BioSensics, Watertown, MA, USA) attached on the shank in the dominant leg and lower back. 46 For balance assessment, participants were asked to stand as quietly as possible for 30 seconds while the feet stay close together but no touching (ie, double stance), and the dominant foot stays half step behind the nondominant foot (ie, semitandem stance). For each stance, participants performed balance tasks with eyes open (EO) and eyes closed (EC) conditions. For each balance task, we measured total sway areas (cm2) in the ankle, hip, and center of mass (CoM), and mediolateral (ML) sway (cm) in the CoM.
We measured gait characteristics using five validated wearable sensors (LegSys™, BioSensics, Watertown, MA, USA) attached on the middle of the thigh and distal shank in both legs, and lower back. 47 For gait assessment, participants were asked to walk 10 meters at their normal and fast paces (ie, normal walking and fast walking). In addition, participants were asked to perform a cognitive task (eg, counting backward by twos) while walking (ie, dual-task walking). For each gait task, we measured stride velocity (m/s), stride length (m), stride time (seconds) and double limb support (%).
Statistical Analysis
Descriptive results are expressed as mean ± standard deviation (SD). To compare outcome values between baseline and 4-week follow-up (ie, repeated measurements at two time points), we used a linear mixed model with random effects of participants and fixed effects of two time points (ie, baseline and follow-up), and age and BMI (ie, covariates). P values < .05 were considered significant differences in 4-week follow-up assessment compared to baseline assessment after Bonferroni correction. We estimated effect size for quantifying the difference in outcome values between baseline and follow-up using Cohen’s d, and denoted it as d in the results section. We classified the magnitude of effect size in the following categories: d < 0.20 as no noticeable effect, 0.20 ≤ d < 0.50 as small effects, 0.50 ≤ d < 0.79 as medium effects and 0.80 ≤ d < 1.29 as a large effects. 48 All statistical analyses were performed using SPSS® version 25 (IBM, Armonk, NY, USA).
Results
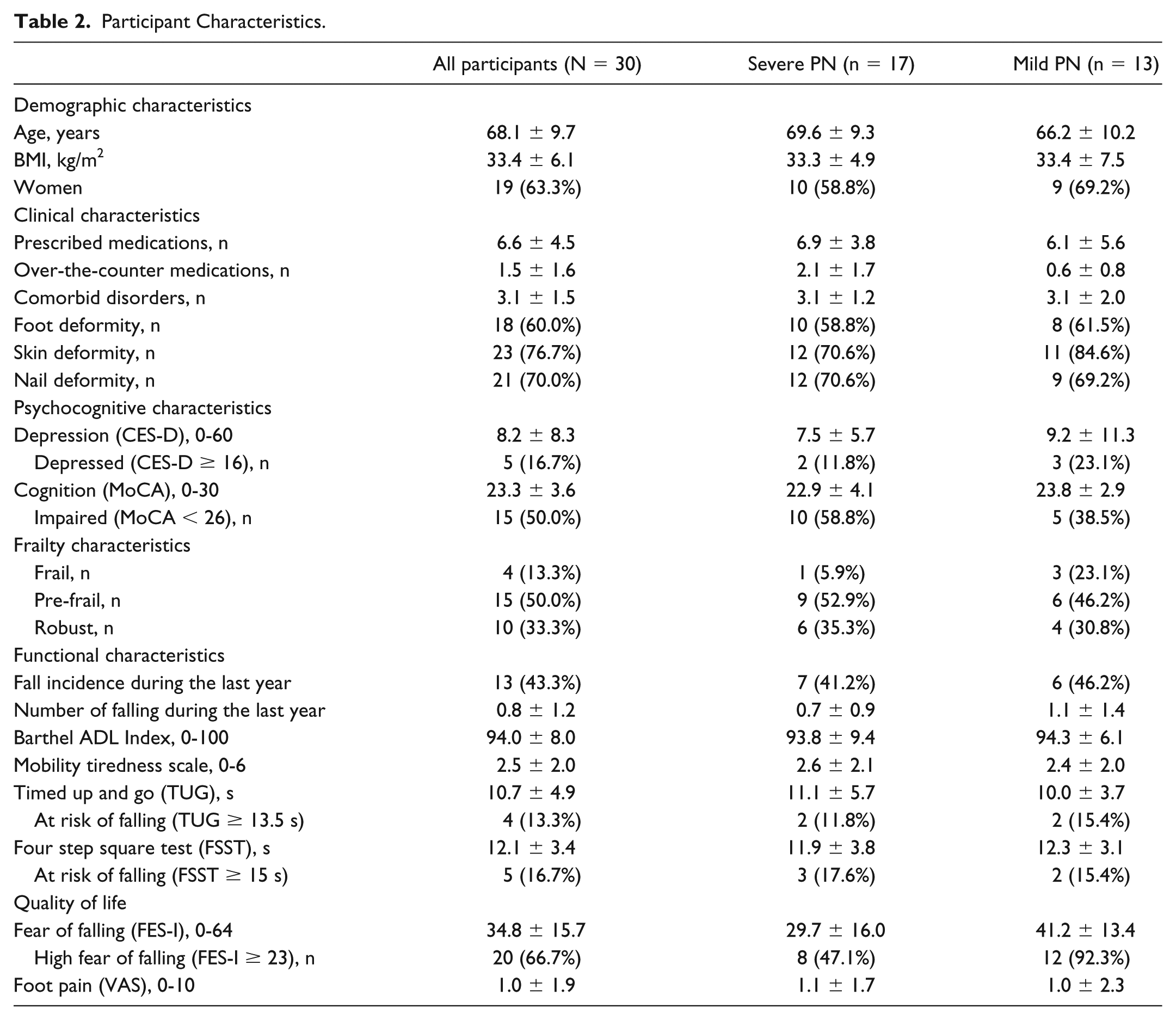
Thirty people with type 2 diabetes met the inclusion and exclusion criteria, and completed the full protocol. We summarized baseline characteristics for all participants in Table 2. We summarized characteristics of pathophysiology for baseline and follow-up for all participants in Table 3. We found significant improvement in neuropathic symptom. All participants received the same mechanical stimulation to the arch of the plantar surface of the foot through the wearable foot compression device. Across all participants, VPTmax reduced significantly in follow-up compared to baseline (before = 27.4 ± 12.6 V, after = 23.3 ± 11.9 V, 15.0% decrease, P = .007, d = 0.33). When participants were divided into two subgroups of severe PN (VPTmax ≥ 25 V) and mild PN (VPTmax < 25 V) in baseline evaluation, the subgroup of severe PN had significant reduction in VPTmax in follow-up evaluation compared to baseline evaluation (before = 36.5 ± 7.6 V, after = 30.5 ± 10.5 V, 16.4% decrease, P = .005, d = 0.65). VPTmax in follow-up evaluation tended to reduce compared to baseline evaluation in the subgroup of mild PN, however the reduction was not significant (before = 15.5 ± 5.8 V, after = 14.0 ± 5.2 V, 9.7% decrease, P = .496, d = 0.27). There were no significant changes in lower extremity vascular status as measured by SPP and ABI, and lower extremity edema as measured by calf and ankle circumferences between baseline and follow-up (all P > .05).
Participant Characteristics.
Characteristics of Pathophysiology for Baseline and 4-Week Follow-Up for All Participants.
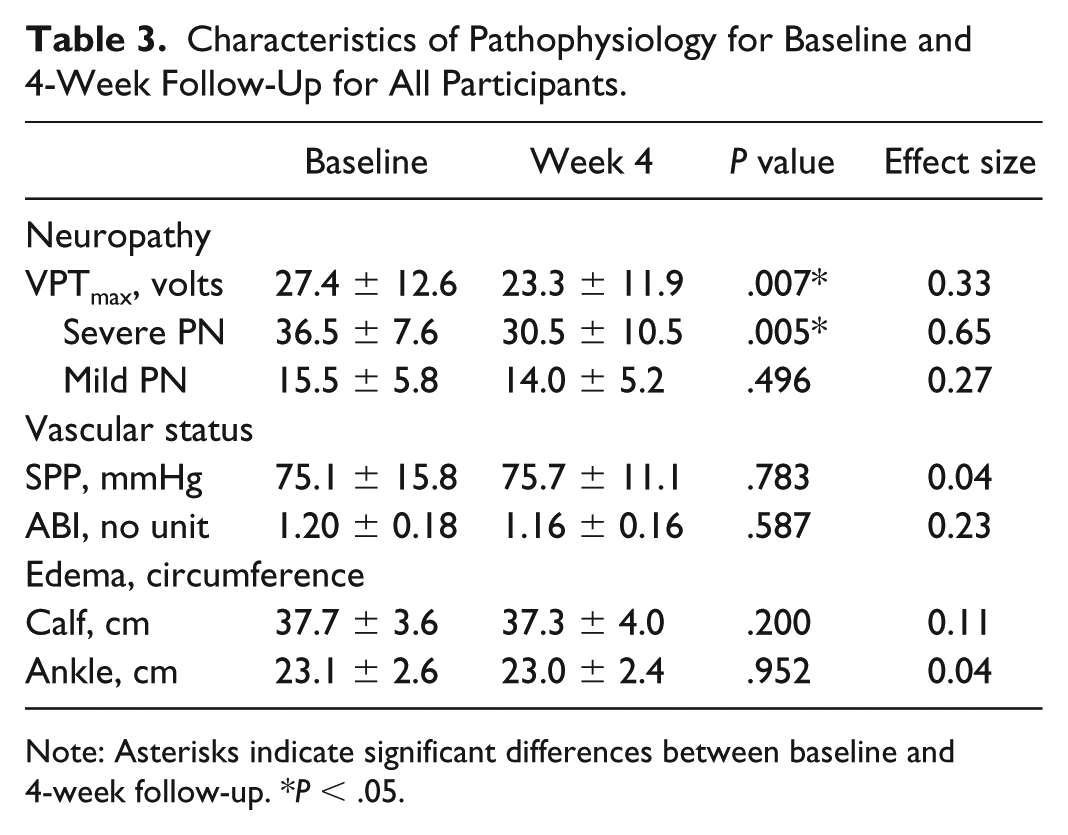
Note: Asterisks indicate significant differences between baseline and 4-week follow-up. *P < .05.
We summarized balance characteristics for baseline and follow-up for all participants in Table 4. Across all participants, there were no significant improvements in ankle (deg2), hip (deg2) and CoM sway (cm2), however we found significant improvement in some characteristics for balance control during quiet standing with double stance. Importantly, CoM sway in the ML direction reduced significantly for double stance with EO and EC conditions in follow-up compared to baseline (before = 0.94 ± 0.43 cm, after = 0.76 ± 0.32 cm, 21.3% decrease, P = .020, d = 0.47; before = 1.10 ± 0.45 cm, after = 0.83 ± 0.37 cm, 24.5% decrease, P = .033, d = 0.66, respectively). Similar to the results for VPTmax, the subgroup of severe PN in baseline evaluation had significant reduction in CoM sway in the ML direction for double stance with EO and EC conditions in follow-up evaluation (before = 0.94 ± 0.35 cm, after = 0.75 ± 0.37 cm, 20.2% decrease, P = .024, d = 0.53; before = 1.22 ± 0.55 cm, after = 0.83 ± 0.36 cm, 32.0% decrease, P = .041, d = 0.84, respectively). Although CoM sway in the ML direction for double stance with EO and EC conditions tended to decrease in the subgroup of mild PN but the decrease was not significant.
Characteristics for Balance Control for Baseline and 4-Week Follow-Up for All Participants.
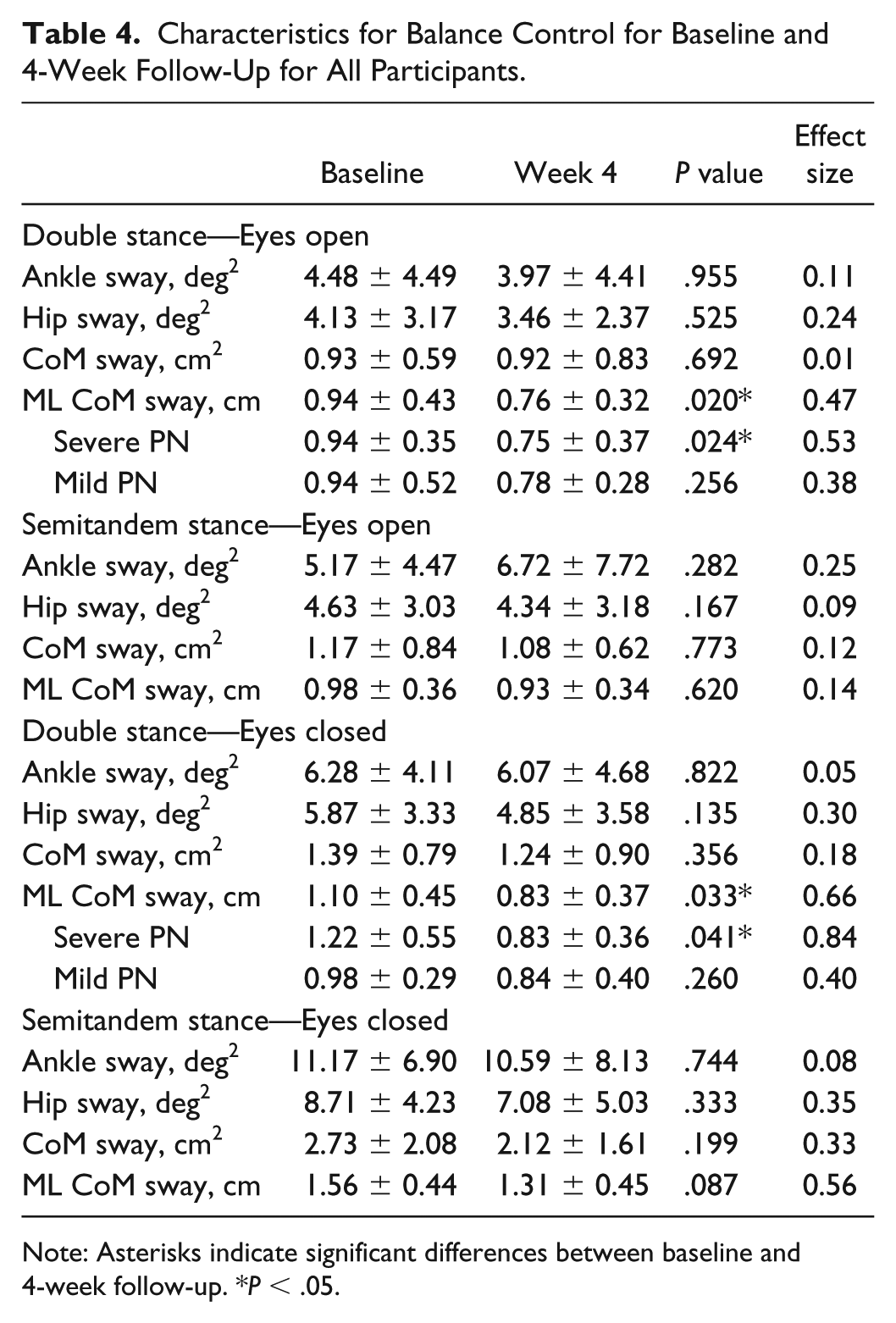
Note: Asterisks indicate significant differences between baseline and 4-week follow-up. *P < .05.
We summarized gait characteristics for baseline and follow-up for all participants in Table 5. We found significant improvement in several gait variables for all walking tasks. Most importantly, across all participants, stride velocity increased significantly from baseline to follow-up for all walking tasks (before = 0.87 ± 0.21 m/s, after = 0.96 ± 0.23 m/s, 12.6% increase, P = .017, d = 0.41 for normal walking; before = 0.75 ± 0.18 m/s, after = 0.91 ± 0.23 m/s, 21.3% increase, P = .001, d = 0.77 for dual-task walking; before = 1.10 ± 0.33 m/s, after = 1.20 ± 0.27 m/s, 9.1% increase, P = .043, d = 0.33 for fast walking). In addition to improvement in stride velocity, we found significant improvement in stride length for normal walking and dual-task walking tasks (before = 1.05 ± 0.21 m, after = 1.13 ± 0.20 m, 7.6% increase, P = .030, d = 0.35; before = 1.03 ± 0.19 m, after = 1.14 ± 0.24 m, 10.7% increase, P = .009; d = 0.51, respectively), and marginal improvement in stride length for fast walking task (before = 1.15 ± 0.27 m, after = 1.24 ± 0.24 m, 7.8% increase, P = .050, d = 0.35). Also, stride time decreased in follow-up compared to baseline for dual-task walking (before = 1.41 ± 0.16 s, after = 1.28 ± 0.15 s, 9.2% decrease, P < .001, d = 0.84), and double limb support decreased in follow-up compared to baseline for dual-task walking and fast walking (before = 31.02 ± 6.23 %, after = 28.22 ± 5.48 %, 9.0% decrease, P = .004; d = 0.48; before = 23.96 ± 7.61 %, after = 22.14 ± 5.84 %, 7.6% decrease, P = .031, d = 0.27, respectively).
Characteristics for Gait Performance for Baseline and 4-Week Follow-Up for All Participants.
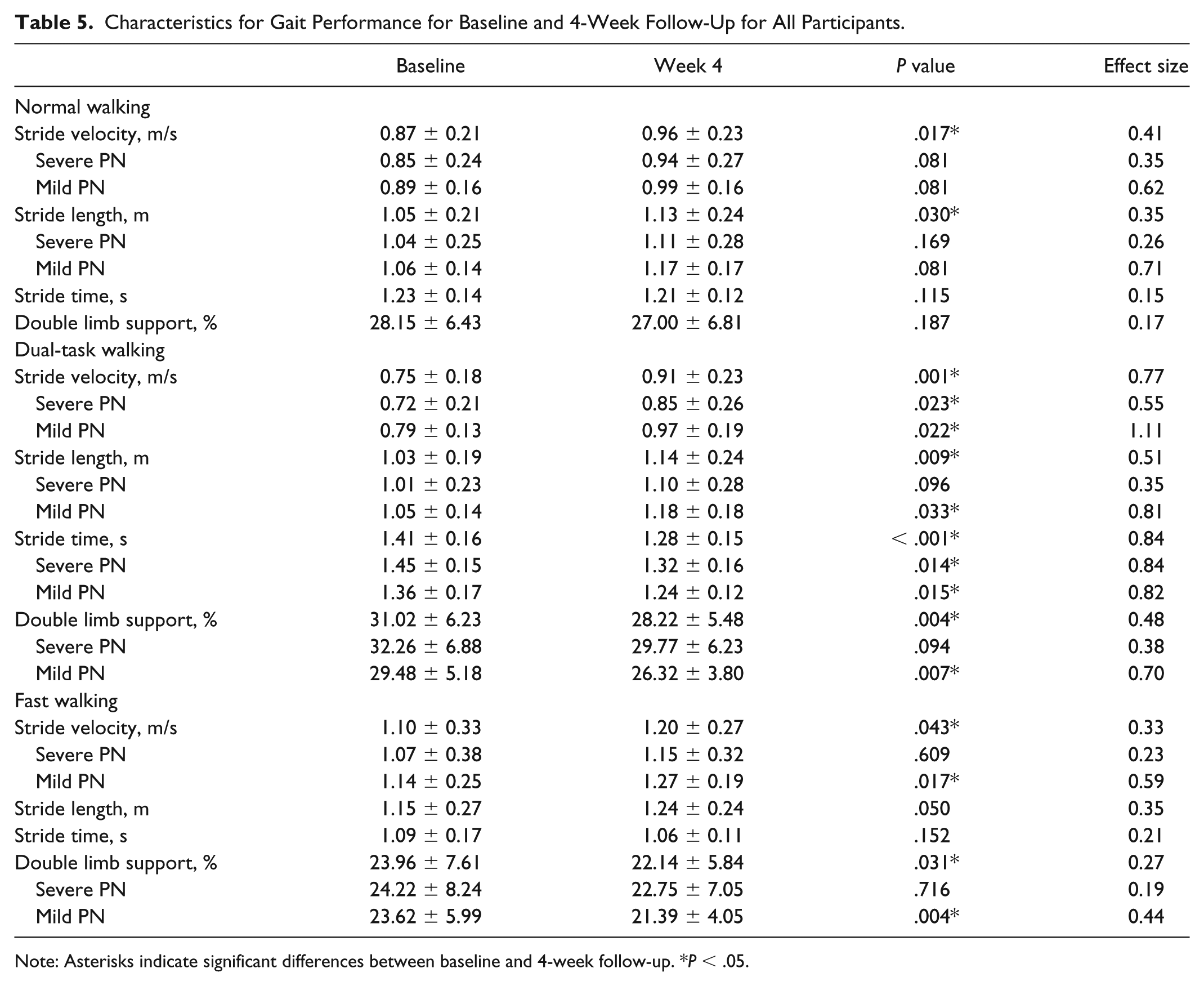
Note: Asterisks indicate significant differences between baseline and 4-week follow-up. *P < .05.
After dividing into two subgroups, both subgroups had significant increase in stride velocity for dual-task walking in follow-up compared to baseline (before = 0.72 ± 0.21 m/s, after = 0.85 ± 0.26 m/s, 18.1% increase, P = .023, d = 0.55 for the subgroup of severe PN; before = 0.79 ± 0.13 m/s, after = 0.97 ± 0.19 m/s, 22.8% increase, P = .022, d = 1.11 for the subgroup of mild PN). Also, the subgroup of mild PN in baseline evaluation had significant increase in stride velocity for fast walking in follow-up (before = 1.14 ± 0.25 m/s, after = 1.27 ± 0.19 m/s, 11.4% increase, P = .017, d = 0.59). Both subgroups’ stride velocity tended increase for normal walking and the subgroup of severe PN tended to walk faster for fast walking, however the increase was not significant. For all other gait parameters, significant improvements were found for stride length for the subgroup of mild PN, stride time for both subgroups and double limb support for the subgroup of mild PN for dual-task walking, and double limp support for the subgroup of mild PN for fast walking.
Discussions
We demonstrated that daily use of plantar mechanical stimulation through a micro-mobile foot compression device installed in a shoe insole is effective for improving vibration perception, which likely results in improvements in some balance outcomes and some gait parameters. Key findings were improvements in plantar sensation in the foot, CoM sway in the ML direction during quiet standing, and stride velocity and other spatiotemporal gait parameters after using the wearable foot compression devices for four weeks. These findings highlight the potential of plantar mechanical stimulation as an adjunctive therapy for treating symptoms related to DPN. To our knowledge, this is the first trial that investigated therapeutic effectiveness of daily use of mechanical stimulation under natural circumstances on neuropathic symptoms, vascular status, lower extremity edema, balance and gait in people with DPN.
In this study, as hypothesized, we found 15% reduction in VPTmax in the foot after receiving 4 weeks of the treatment. In addition, as hypothesized, we found significant improvements in gait and balance in this study. A possible explanation for the recovery in plantar sensation is accelerated local blood flow in the foot due to the mechanical stimulation. The association between diabetic neuropathic foot and reduced microvascular blood flow (ie, reduced oxygenation) is well established, 49 and improving local blood flow is recommended for clinical management of diabetic foot.2,34 Together with the results from previous studies,27-29 our findings support that mechanical stimulation through wearable foot compression device may be a potential clinical option for neuropathic symptoms. Sensory information that is delivered to the central nervous system plays a critical role for successful completion of gait and balance tasks. 50 People with sensory impairment such as DPN have poor performance in gait and balance.5-10 In healthy people, artificial reduction in sensory function worsens balance control,51,52 and also enhanced sensory information improves gait and balance tasks.32,53 Our findings were consistent with previous studies that reported improvements in plantar sensation, balance (ML sway) and gait (stride velocity, stride length, overall dual-task performance, and overall fast walking performance) in people with DPN after receiving electrical stimulation.12,23
In addition, higher intervention response for ML sway postural balance may have been related to the specific ML baseline balance deficit in our fall prone participants, in particular among those with severe PN as described in previous studies.54-56 Similarly, we observed higher improvement during dual-task gait and fast walking, which could be also link to baseline gait and cognitive-motor deficits in particular among those with severe PN.57-59 Thus, it is suggested that wearing the foot compression device may be also effective in treating motor impairments in DPN in particular among those with severe PN.
Among our study sample, 77% (n = 23) were aged 65 years and older (ie, were older adults). Increased ML CoM sway during balance tasks 60 and decreased gait speed during gait tasks 61 are associated with increased risk of falling in older adults. Thus, the improvement in gait and balance that was found in this study suggests the foot compression device may be beneficial in decreasing risk of falling in people with DPN. Importantly, even after the participants were divided into two subgroups based on the baseline VPTmax, we found significant improvements or tendency of improvements in VPTmax, balance outcomes and gait parameters in both subgroups. Thus, the mechanical stimulation may be beneficial across diabetic people with varied severities in neuropathy symptoms.
In this study, we asked participants to wear the shoes four hours per day. In fact, our previous studies demonstrated the medium values for the longest unbroken sitting bout during the daytime was less than four hours.8,19 Thus, we anticipate that participants will be more likely to get benefit from the foot compression device when they were sitting thus the choice of four hours may replicate the use of the system during daily activities as well.
There are several limitations in this study. First, the study design was single-arm-intervention study, and the potential training effect in balance outcomes and gait parameters were not considered. Also, we included people with type 2 diabetes in this study only, and the effectiveness of the intervention for people with type 1 diabetes needs to be investigated in future studies. Given the improvements in dual-task walking task in this study, it is likely that the treatment may improve dual-task balance control as well but it was not tested in this study. It is suggested to investigate dual-task balance control after using the wearable foot compression device in future studies. Our sample was a convenience sample, and relatively small as we were not able to find differences in several balance measurement. The relatively small sample size may also limit the generalizability of our findings. Although we asked participants to wear the shoes for at least four hours per day during four weeks, the adherence was not objectively controlled, thus there is a possibility that time of wearing would have affected the results. The baseline motor assessment has been performed while participants were wearing their own footwear, however the follow-up assessment has been performed while they were wearing the study footwear, which may have affected results for the motor tasks. However, given the improvements in VPTmax that is independent of footwear type, it is likely that the improvements in motor tasks are due to the treatment. In addition, potential effect of being familiar to the motor tasks in the follow-up assessment may have affected the results.
Conclusion
This study suggests mechanical stimulation applied to the arch of the foot through a micro-mobile foot compression device improves neuropathic symptoms, and gait and balance performances in people with DPN. The device is equipped in a shoe insole thus wearable and proper for daily use without additional discomfort. The technique may be considered as an alternative adjunct treatment for exercise intervention, electrical stimulation, or exoskeleton.
Footnotes
Acknowledgements
The authors thank Ms Ana Enriquez, Mr Ivan Marin, Mr Louie Morsy, Mr Manuel Gardea, Ms Luciana Narvaez for their help with data collection and analysis. The study was registered in ClinicalTrials.gov (study identifier: NCT03135535)
Abbreviations
ABI, ankle brachial index; ADL, activities of daily living; CES-D, Center for Epidemiological Studies Depression Scale; CoM, center of mass; DPN, diabetic peripheral neuropathy; EC, eyes closed; EO, eyes open; FES-I, Falls Efficacy Scale–International; FSST, Four Step Square Test; IWDGF, International Working Group on the Diabetic Foot; ML, mediolateral; MoCA, Montreal Cognitive Assessment; PN, peripheral neuropathy; PROMIS, Patient-Reported Outcomes Measurement Information System; SPP, skin perfusion pressure; TUG, Timed Up and Go; VAS, Virtual Analog Scale; VPT, vibration perception threshold.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by AVEX LLC and BOA Technology Inc. However, the funding sources played no role in study design, data analysis, interpretation of the results, or preparation of the manuscript.