
Abstract

We have previously published an observational study summarizing a follow-up period of at least two years of five young male patients with T1DM who practiced combat sports under the care of a physical activity-oriented specialist diabetes outpatient clinic. 1 Three of the patients included in the study were mixed martial arts competitors and two were kick-boxing competitors. We concluded that an individualized approach to diabetes management for T1DM patients practicing combat sports may result in achieving and maintaining satisfactory glycemic control without increased risk of metabolic decompensation. 1 We believe it was an important finding, since combat sport is a mixture of different types of exercise (often with unpredictable proportions of aerobic vs anaerobic vs intermittent exercise) with variable effects on glucose patterns.2-5 It was unclear, however, if those results would be sustainable upon longer observation. Here we present the metabolic statuses of those patients after another 3 years of follow-up.
One individual (patient 3 in the original publication) gave up his career as a competitor two years ago and has established his own gym. He is still physically active (approximately 1 hour of exercise per day), but his activity is much lower compared to that of a combat competitor. His current HbA1c is 6.9% (51.9 mmol/l). During the entire follow-up period he had no episodes of metabolic decompensation or severe hypoglycemia, and no late complications of diabetes were observed. Unfortunately, the patient has gained 7 kg since giving up his career. His current BMI is 27.4 kg/m 2 , and his insulin dose per kg increased from 0.56 IU/kg to 0.71 IU/kg.
Another patient (number 2 in the original publication) was not available for follow-up. Neither his activity nor his glycemic status is known. It is probable that he gave up sports, as there is no information in the Internet concerning him in current combat sport events. The reason he abandoned the sport is unknown.
All three remaining patients are still active competitors. Their past and current metabolic statuses are presented in Table 1.
Clinical Characteristics of Study Participants, Based on the Previously Published Data.
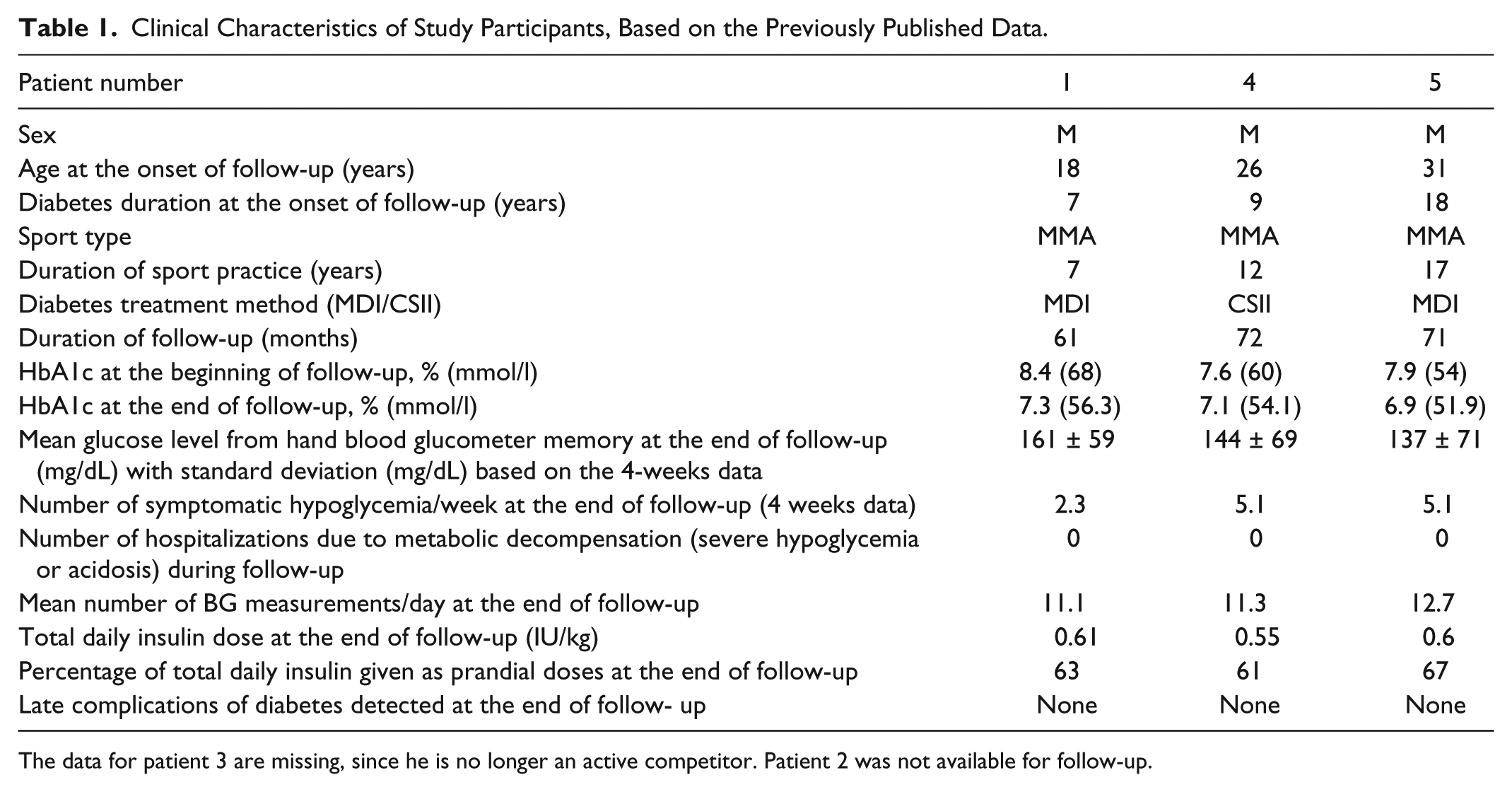
The data for patient 3 are missing, since he is no longer an active competitor. Patient 2 was not available for follow-up.
In comparison to data published previously, all patients were able to decrease their HbA1c without increasing the rate of symptomatic hypoglycemia. All the patients declared that this improvement was mainly due to gaining experience in diabetes management under unusual, extreme conditions, as well as to an individualized approach to the treatment.
Of note, all the patients follow the same pattern of diabetes management regarding self-monitoring of blood glucose and insulin therapy, which is different from that of most T1DM patients seen at our department: 6
- They perform a high number of blood glucose measurements (11.1-12.7/day). Since all the patients practice combat, contact sports, they do not use continuous/flash blood glucose systems. Wearable devices are not allowed during competition and could be dangerous during training. Patients on CSII simply disconnect pumps for training and competition.
- They administer a low dose of insulin per kilogram (0.55-0.61 IU/kg). This is due to the high intensity of the exercise and high protein consumption (approximately 30-40% of daily calorie intake).
- They administer a relatively high percentage of insulin as prandial dose (61-67%).
In summary, we present a relatively long follow-up of 3 patients with T1DM who practice combat sports. These are not the sports of choice of most patients with T1DM, but for those that choose to practice them, achieving and maintaining satisfactory glycemic control without increased risk of metabolic decompensation is possible.
It is worth to underline that glycemic control tends to improve with time, probably due to gaining experience in diabetes self-management while practicing combat sports.
Footnotes
Abbreviations
BG, blood glucose; CSII, continuous subcutaneous insulin infusion; HbA1c, glycated hemoglobin A1c; MDI, multiple daily injections; MMA, mixed martial arts; T1DM, type 1 diabetes mellitus.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.