
Abstract
Background:
The detection of insulin infusion set (IIS) occlusions is an important feature of insulin pumps with regard to patient safety. However, there are no requirements for a time limit until an alarm has to be triggered after an occlusion occurred. The standard IEC 60601-2-24 is applicable for insulin pumps and describes test settings and procedures to determine occlusion detection time (ODT).
Methods:
In this study, ODT of six different insulin pump models with different IIS (in total 10 different insulin pump systems) was tested for two basal rates (1.0 U/h and 0.1 U/h).
Results:
Differences were seen between the tested pump systems. At a basal rate of 1.0 U/h all insulin pump systems showed an acceptable ODT of less than 5 hours. However, at a basal rate of 0.1 U/h, as often used in children, the median ODT ranged from approximately 4 hours to more than 40 hours. With the lower basal rate, median ODT was longer than 6-8 hours for 9 of the 10 systems.
Conclusions:
Insulin pump users should not blindly rely on occlusion alarms but perform regular glucose monitoring and manufacturers should develop mechanisms that allow an earlier detection at low basal rates.
An important safety feature of insulin pumps is the detection of occlusions in the insulin infusion set (IIS) and the release of an alarm to notify the user. Unresolved occlusions may lead to retention of insulin delivery and subsequent high glucose levels and diabetic ketoacidosis (DKA) at worst; early detection is therefore important to ensure patient safety. Occlusions are among the most common IIS problems in continuous subcutaneous insulin infusion (CSII) therapy. 1 There are different factors that might influence the occurrence and detection of occlusions, such as material and length of cannula and tubing, current basal rate or bolus volumes, and specific detecting mechanisms within the insulin pump. Some insulin pumps also allow the user to adjust the sensitivity of the alarm.
Requirements for infusion pumps are described in the standard IEC 60601-2-24:2012, 2 but as the standard addresses infusion pumps in general, only technical requirements are specified without particular consideration of clinical needs or impact. Acceptance criteria or individual requirements for insulin pumps are not included.
In this study, the occlusion detection time (ODT) was investigated for six different insulin pumps with different infusion set types.
Methods
All experiments were performed by an independent GLP-certified testing laboratory, data analyses and interpretation were performed by the Institut für Diabetes-Technologie Forschungs- und Entwicklungsgesellschaft mbH an der Universität Ulm, Ulm, Germany.
Insulin Pump Systems
For this investigation, six different insulin pump models with up to 3 different IIS each were evaluated (pump system = insulin pump model + IIS type) (Table 1). For each system, an IIS with soft cannula was tested; in addition, some pumps were also tested with IIS with steel cannula. All cartridges were filled with insulin aspart (NovoRapid, Novo Nordisk, Bagsværd, Denmark).
Tested Insulin Pump Systems.
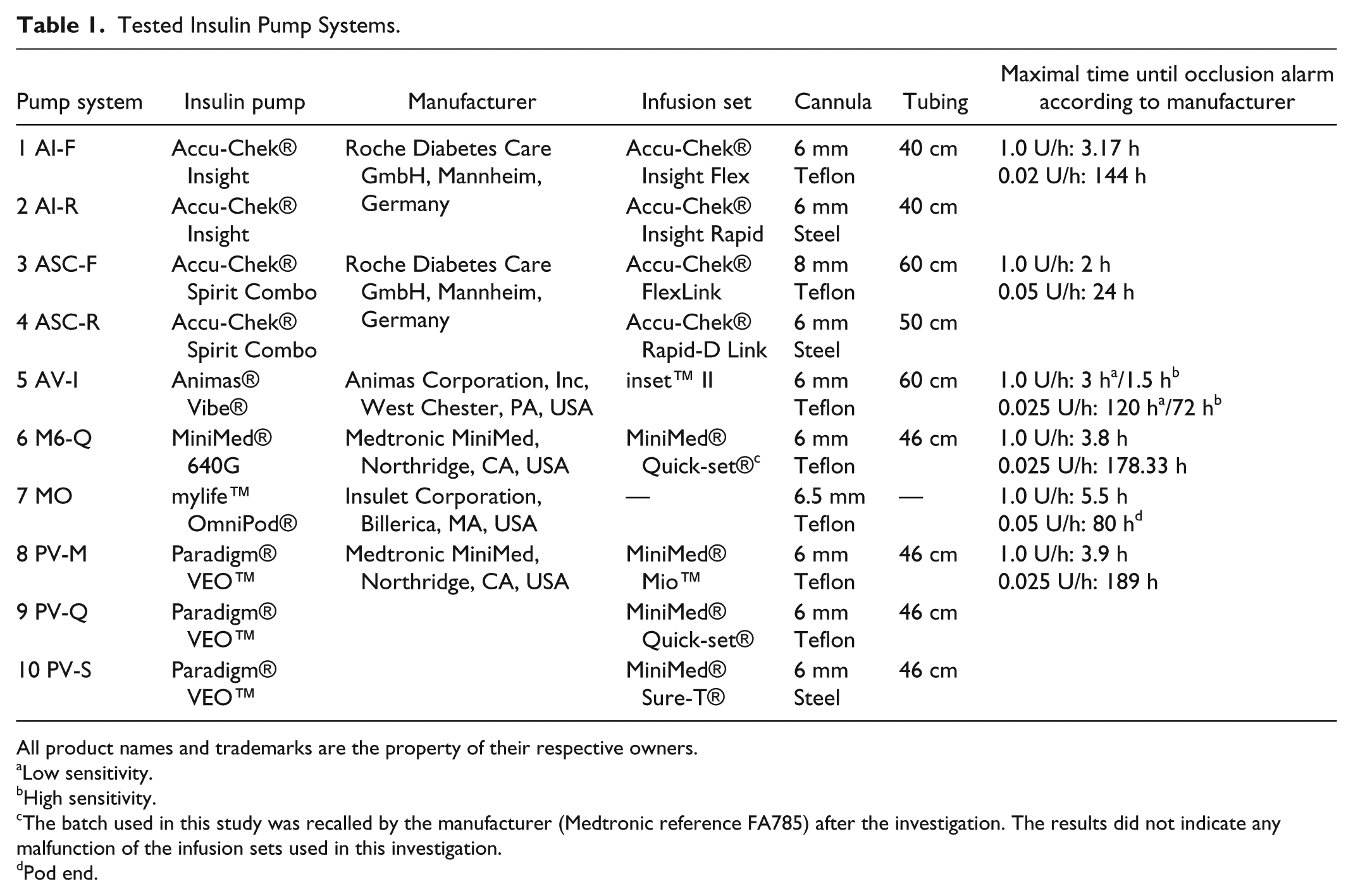
All product names and trademarks are the property of their respective owners.
Low sensitivity.
High sensitivity.
The batch used in this study was recalled by the manufacturer (Medtronic reference FA785) after the investigation. The results did not indicate any malfunction of the infusion sets used in this investigation.
Pod end.
Test Setting
ODT was evaluated following IEC 60601-2-24-1998 3 section 51.101, but a different test setting was used (Figure 1). No pressure transducer was used because it would have caused additional dead volume that might have impaired the results for the very small flow rates that were investigated.
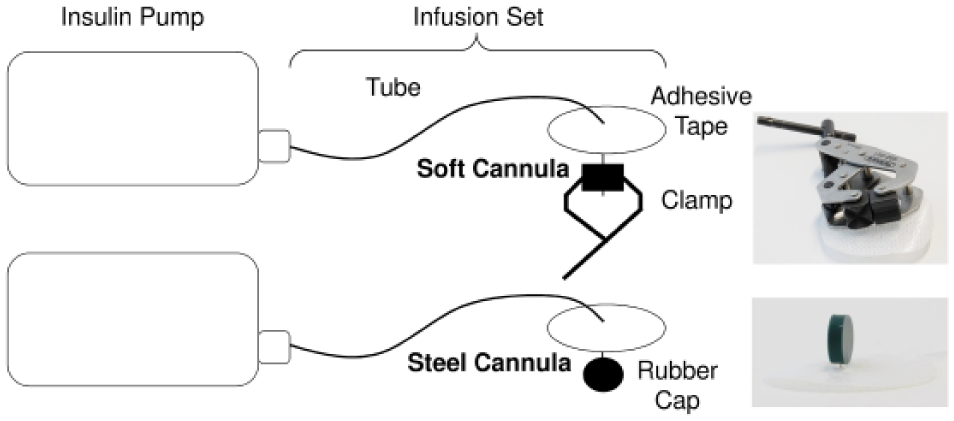
Occlusion induction in soft cannulas (above) and steel cannulas (below).
Two different basal rates were evaluated: 1.0 U/h (used in adolescents and adults) and 0.1 U/h (often used in children). If a pump had adjustable sensitivity settings for the occlusion alarm, all available settings were used.
Prior to the measurements, insulin cartridges were preconditioned for 24 hours at room temperature to avoid formation of air bubbles during the measurements. Insulin pumps were prepared and IIS were primed according to the manufacturers’ instructions. Before an occlusion was induced, the systems were run at the tested basal rate for 1 h ± 5 min. For measurements at 0.1 U/h, the systems were first run at 1.0 U/h for 1 hour before the run-in at the tested rate. Soft cannulas were occluded with a metal clamp whereas steel cannulas were obstructed by placing a rubber cap on their tip (Figure 1). Two different occlusion methods had to be applied because steel cannulas could not be completely occluded using the clamp. Appropriate occlusion was checked visually and the starting time was noted. The insulin pumps ran on the predefined basal rate until the occlusion alarm was triggered and then the timestamp of the alarm was read out of the data storage of the pumps. If no alarm occurred after 24 hours (basal rate 1.0 U/h), or 72 hours (0.1 U/h), respectively, the measurement was stopped and not repeated. The IIS were checked for ruptures and leakage over their entire length by visual and olfactory (typical smell of excipients) examination.
After an alarm occurred (for basal rate 1.0 U/h, as IEC 60601-2-24-1998 requires an intermediate rate), the noninjected volume was determined by weighing the complete system, then removing the occlusion and draining the accumulated volume, and weighing the system again.
For each pump system, three individual insulin pumps with IIS were tested three times each to obtain nine data sets per insulin pump system.
Statistical Analysis
From nine ODT values per pump system, mean, median, first and third quartiles, and minimum and maximum were calculated.
Results
Median ODT of all insulin pump systems ranged from 00:34 h to 03:55 h at a basal rate of 1.0 U/h and from 03:56 h to 41:21 h at 0.1 U/h (Figures 2 and 3). The longest individual ODT was 04:48 h for 1.0 U/h with soft cannula and 04:22 h with steel cannula; and 65:40 h and 39:27 h, respectively, for 0.1 U/h (Table 2). In four experiments (soft cannula), no alarm was recorded until the end of the experiment (24 h for 1.0 U/h; 72 h for 0.1 U/h): once with pump system AV-I (set at high sensitivity) at a basal rate of 1.0 U/h, twice with pump system M6-Q at 1.0 U/h and once with pump system M6-Q at 0.1 U/h. No ruptures or leakages were found in the IIS.
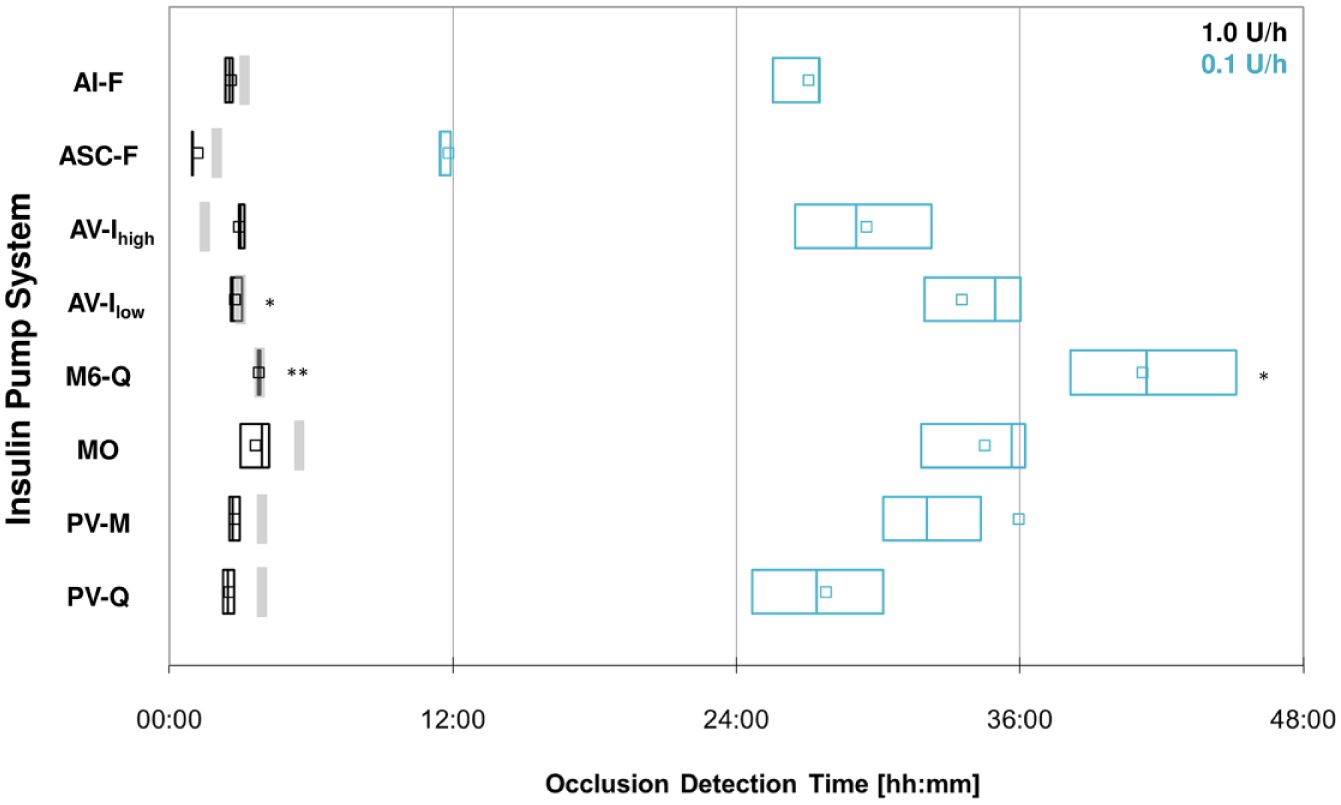
Occlusion detection time of insulin pump systems with soft cannula at basal rates of 1.0 U/h (black) and 0.1 U/h (blue), 9 measurements each. Squares show the mean value, boxes the interquantile range (25-75%) with median, and gray bars the maximal occlusion detection time for 1.0 U/h as indicated by the manufacturer. *8 measurements (no alarm in 1 measurement). **7 measurements (no alarm in 2 measurements).
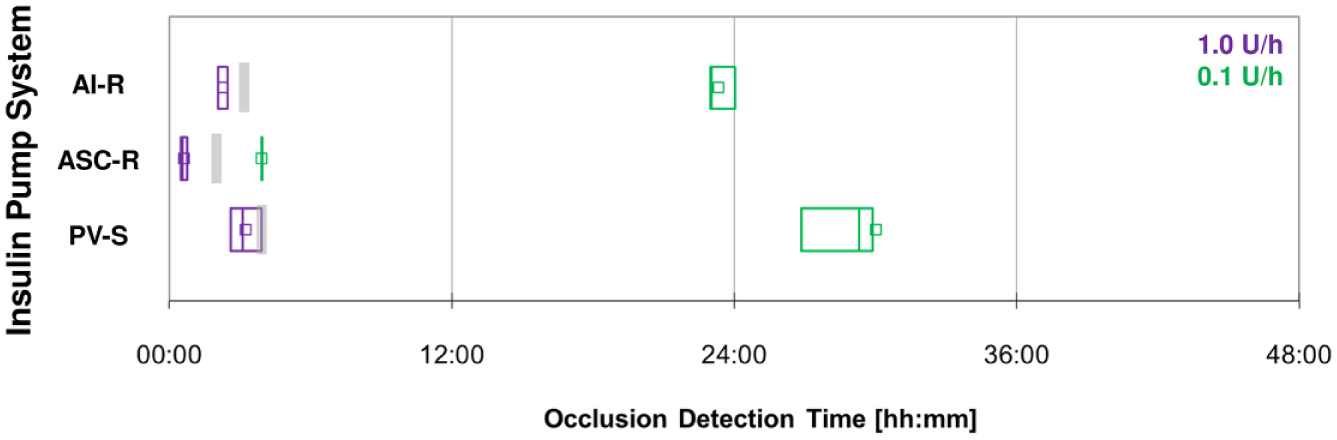
Occlusion detection time of insulin pump systems with steel cannula at basal rates of 1.0 U/h (purple) and 0.1 U/h (green), 9 measurements each. Squares show the mean value, boxes the interquantile range (25-75%) with median, and gray bars the maximal occlusion detection time for 1.0 U/h as indicated by the manufacturer.
Occlusion Detection Time for Pump Systems With Soft (Left) or Steel (Right) Cannula: Median of 9 Measurements.
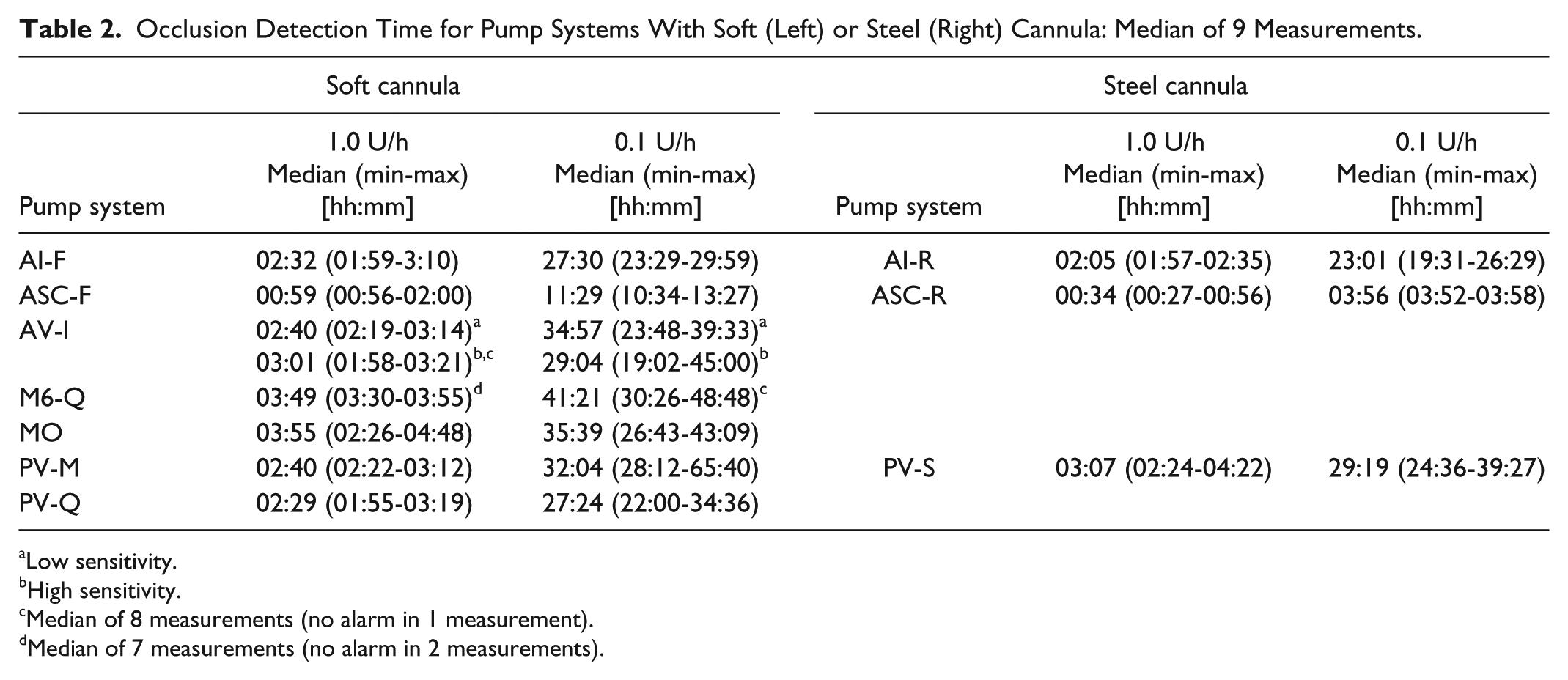
Low sensitivity.
High sensitivity.
Median of 8 measurements (no alarm in 1 measurement).
Median of 7 measurements (no alarm in 2 measurements).
Among systems with soft cannula, pump system ASC-F showed the earliest median ODT in both experiments, whereas pump systems M6-Q and MO showed the longest median ODT. Among systems with steel cannula, ASC-R showed the earliest median ODT in both experiments and PV-S the longest median ODT.
For all pump systems, the ODT was about 9 to 11 times longer with the 0.1 U/h basal rate compared to the rate of 1.0 U/h (Table 2).
Pump system AV-I allowed adjustment of occlusion sensitivity, thus both low and high sensitivity were tested. At 0.1 U/h, faster occlusion detection was observed with the high sensitivity setting, at the higher basal rate, no clear difference was observed.
The investigation of different IIS with the same insulin pump showed that, at least in some pumps, there is an influence of the type of IIS. In two pumps, systems with steel cannulas showed faster occlusion detection than the respective IIS with soft cannulas.
Compared to the maximum time for ODT indicated by the respective manufacturers for 1.0 U/h (Table 1), maximum measured times for seven of the pump systems were equal to or below the specified time in this investigation, three pump systems exceeded the indicated maximal time. Measured noninjected volumes for all systems were far below the expected volumes with large variations between the individual measurements (data not shown).
Discussion
Occlusion alarms are an important feature of insulin pumps, because the users may not notice nondelivery of insulin in the absence of alarms until glucose monitoring shows unexpected high values. An early detection might prevent subsequent hyperglycemia and potential development of DKA.
Unfortunately, there is no common standard that specifies a maximum detection time for insulin pumps. From a clinical point of view, insulin retention for up to 6 hours is supposed to be acceptable;4-7 however, an exact time limit cannot be determined. It depends, among others, on the size of the insulin depot from previous basal rate and bolus injections. 8 Considering the medium basal rate of 1.0 U/h that might be used by adolescent or adult CSII patients, all tested pump systems detected the occlusion in less than 5 hours which seems early enough. Using a very small basal rate, like, for example, children do, the observed time to occlusion alarm might not be sufficient. Only one pump system gave an occlusion alarm after approximately 4 hours, in most of the other systems it took more than 24 hours. If a lower basal rate than 0.1 U/h is used, even longer times are to be expected. One might argue that it is likely that bolus doses are given in the meantime that contribute to the delivered volume and therefore lead to an earlier detection. But during night usually no bolus is given and younger children might easily sleep for 8 hours or more. In a study, DKA was not observed in any of 22 children that were deprived from insulin for 6-8 hours. 5 Although DKA is only the worst-case complication of acute insulin deficiency, it becomes more likely in particular situations like acute infections. 9 Prolonged or recurrent hyperglycemia, which might occur due to frequent or continued occlusion, decreases the time in target range of glucose levels and therefore can increase the risk for late complications like retinopathy or diabetic nephropathy. 10
In this investigation, varying detection times of the tested insulin pump systems might not only be explained by different detection mechanisms in the insulin pumps, although this is the major technical difference in the different insulin pump models, but also by different materials used in the respective IIS and by different insulin reservoirs. The study results suggest that there may be an influence of whether a steel or soft cannula is used, but this has to be validated in additional studies with an appropriate selection of systems. In addition, the length of the tube could have an impact but this was not investigated in this study. 11 A new IIS development demonstrated that an alternative catheter design, the so-called FlowSmart technology, is able to reduce silent occlusions, that is, pressure rises that do not trigger an alarm, but might be clinically relevant nevertheless. 12
This investigation has some limitations, like no evaluation of noninjected volumes to appraise clinical relevance, as these were not plausible. In addition, the number of valid measurements differs between the pump systems, because in cases when no alarm occurred, the respective measurement was not repeated nor included in the calculation. In these cases, proper occlusion was checked as described above; however, no examination of the noninjected volume was performed. This investigation did not include all available IIS for every tested insulin pump; it is thus not intended to provide a market overview or decision support. For every pump, an IIS with soft cannula was tested; however, tests with steel cannulas were only performed for some pumps. Nonetheless, this does not influence the main findings of the investigation.
Time until occlusion alarm was already investigated by others. Van Bon and colleagues also tested three of the pumps used in this study and found clearly longer times for systems ASC-F/ASC-R and MO at 1.0 U/h, but somewhat shorter times for systems PV-M/PV-Q/PV-S. 11 Interestingly, the times until the alarm occurred at basal rates of 1.0 U/h and 0.5 U/h did not noticeably differ in 2 insulin pumps in their study. Unfortunately, they did not give any information about the infusion sets used. Borot and colleagues also performed occlusion experiments with different insulin pumps, but used basal rates of 2.0 U/h and 0.5 U/h, the results can therefore not be directly compared to this study. 13 Nevertheless, mean ODT at 0.5 U/h were shorter for systems AV-I and PV-M/PV-Q/PV-S compared to the 1.0 U/h results presented here. In both publications, the methods are not described extensively enough to compare the test setups and their influence on the results.
Conclusions
In conclusion, this study showed differences in the sensitivity of occlusion detection between different insulin pump models and IIS. While for medium basal rates the time until an alarm occurs seems acceptable, especially for children using very small basal rates, the times measured might not be sufficient and clinically relevant. CSII patients should therefore not blindly rely on occlusion alarms but perform regular glucose monitoring and check for blood ketones in case of prolonged high blood glucose values. In addition, manufacturers should develop IIS less prone to occlusions and mechanisms that allow for a timely detection of occlusions. 14
Footnotes
Abbreviations
CSII, continuous subcutaneous insulin infusion; DKA, diabetic ketoacidosis; IIS, insulin infusion set; ODT, occlusion detection time.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GF is general manager of the IDT (Institut für Diabetes-Technologie Forschungs- und Entwicklungsgesellschaft mbH an der Universität Ulm, Ulm, Germany), which carries out clinical studies on the evaluation of BG meters and medical devices for diabetes therapy on its own initiative and on behalf of various companies. GF/IDT have received speakers’ honoraria or consulting fees from Abbott, Ascensia, Bayer, Berlin-Chemie, Becton-Dickinson, Dexcom, LifeScan, Menarini Diagnostics, Novo Nordisk, Roche, Sanofi, Sensile, and Ypsomed. UK, DW, and CH are employees of the IDT. RZ has received speaker’s honoraria and/or served on advisory boards from/of Abbott, Animas, Ascensia, AstraZeneca, Lilly, Novo Nordisk, and Roche Diabetes Care.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Performance of the study and scientific writing were funded by Roche Diabetes Care, Germany.