
Abstract
Background:
Temperature sensors are an objective way to assess adherence to diabetic footwear. Good adherence is essential for the prevention of diabetic foot problems. Little is known about the long-term course of adherence in patients at risk for diabetic foot problems.
Method:
A temperature sensor was incorporated into the specialized footwear of patients with type 2 diabetes after their first plantar ulceration. Kaplan-Meier curve was used to analyze when patients started to become nonadherent (not wearing the footwear for two straight weeks). Gender effects on adherence were also analyzed.
Results:
26 patients with a mean observation time of 133.5 days could be analyzed. Mean wearing time of diabetic footwear was 4.2 ± 3.6 h/day (Mdn = 3.4 h/day; interquartile range = 0.5-7.0 h/day) and on 51% of the days patients did not wear their footwear at all. Kaplan-Meier curve revealed that the mean time of adherence was 27.5 weeks. Men achieved a mean time of adherence of 30.5 weeks, while women only achieved 14 weeks. However, due to the small sample size, this difference was not statistically significant.
Conclusions:
Temperature sensors revealed a low long-term adherence to diabetic footwear. Women seemed to be at a higher risk for earlier nonadherent behavior. Adherence to diabetic footwear should be closely monitored and tailored intervention strategies should be developed.
People with diabetes have a higher risk for amputations compared to people without diabetes; 1 thus, the majority of all amputations are still a direct consequence of diabetic foot problems.1,2 This increased risk can be attributed to diabetic neuropathy and circulating problems that lead to foot ulcerations and impaired healing.2,3 Nearly 20% of all infected diabetic foot ulcers lead to amputation.4,5 In a population-based cohort study, the risk of death was 2.5 times higher for diabetes patients with a foot ulcer compared to diabetes patients without a foot ulcer. 6 According to recent estimations, the lifetime incidence of foot ulcers in people with diabetes is between 19% and 34%. 3 Foot ulcerations often occur because of elevated plantar pressure due to neuropathy-related malpositioning of the foot that lead to mechanical stress.3,7,8 In addition, neuropathic sensory loss is another pathogenic factor for foot ulcerations as this increased stress remains unnoticed.9,10 Furthermore, foot ulcerations have a high annual recurrence rate of 40-60%11-13 leading to a high maintenance and relevance of the problem. Prevention of diabetic foot ulcers or increasing ulcer-free days is therefore essential for diabetes patients with an increased risk for diabetic foot problems.2,3,14,15
Therefore, international guidelines strongly recommend the use of customized diabetic footwear and insoles for people with diabetes at risk for diabetic foot problems.14,16 The customized footwear reduces the mechanical stress by redistributing pressure to the plantar tissue, thereby aiming to reduce the risk for (re)ulcerations. Thus, patients are instructed to wear their footwear at every step. While there is some evidence for the efficacy of customized diabetic footwear,17,18 a big problem in efficacy studies remains patients’ adherence.3,18 Due to the difficulties in assessing adherence (eg, reporting bias, demand effects), it is often neglected. Accordingly, in a meta-analysis on the efficacy of diabetic footwear and offloading interventions from 2008, 17 out 21 trials did not have any information about patients’ adherence. 17 Those trials that included adherence data relied mainly on self-report. Therefore, inferences on the true efficacy of footwear were hard to draw because the efficacy is underestimated when it remains unclear whether the footwear was worn.
More recent approaches in assessing adherence tried to avoid the evident problems of reporting bias and demand effects that come with self-report measures and used technological approaches. Temperature sensors are being used to determine whether the footwear was worn, thereby allowing an inference on patients’ adherence. Combined with a step activity monitor, Waaijman et al were able to show that only 75% of all steps were taken with the prescribed footwear. 19 Furthermore, a randomized controlled trial that used the same approach for adherence measurement found that only 46% of patients had an adherence rate ≥ 80%. 11 Interestingly, only for those patients the efficacy of diabetic footwear could be demonstrated. Similarly, Crews et al found that off-loading adherence was associated with the amount of healing of diabetic foot ulcers. 20 The innovative approach of using temperature sensors offered objective data for adherence of diabetic footwear for the first time. However, with the temperature sensors used in these studies only 7-14 days,11,19 respectively 35 days 20 could be analyzed. With such an objective measure, however, it would be interesting to have more long-term data. This way, it would be possible to analyze the long-term course of adherence. The aim for this observational study was to extend the observation period of adherence to diabetic footwear and to analyze when patients become nonadherent. Specifically, we were also interested in possible gender effects of adherence; there are many clinical observations about gender differences regarding therapeutic footwear that might impact adherence21-23 but empirical evidence on actual adherence is missing.
Methods
Sensor
For a continuous, long-term measurement of adherence, we used a sensor that measured the temperature within the footwear every 15 minutes (96 measurements per day) and stored these data for 100 days before overwriting the oldest data (orthotimer®; rollerwerk medical engineering & consulting, Balingen, Germany). Hence, by reading out the sensor data before this deadline, longer observation periods were possible. Every sensor reading was stored with a date- and timestamp. In case patients were prescribed more than one footwear (eg, for work, at home) data from different sensors could easily be combined.
Defining a Cutoff Temperature for Wearing
To determine the right cutoff temperature that optimally distinguishes between wearing and not wearing the footwear, the sensor was first tested in volunteers without diabetes. The exact times of donning and doffing the footwear were noted in a logbook and compared with the temperature data of the sensors. A receiver operating characteristic (ROC) analysis was conducted to identify the optimal cutoff temperature based on sensitivity and specificity.
Procedure
This study was designed as an observational study and followed diabetes patients after plantar ulceration who received their first customized diabetic insoles. The insoles were prescribed by patients’ treating diabetologist and customized as usual by specialized orthopedic shoemakers based on pressure distribution scans, static 2D footprint of the plantar sole and 3D recording of the foot on a specially made foam footprint. The materials used for the DIABETEC individual orthotic consisted of at least three different layers that were adapted depending on walking speed and weight of the patient. At the thinnest point, this medical product is 8 millimeters thick and is worn in an extra-depth stiff, rocker shoe. Patients received care as usual; no additional interventional measures were introduced by the study.
All patients were informed about the temperature sensor prior to customization and gave written informed consent. The temperature sensor was then incorporated into the longitudinal arch of one insole without impairing the offloading capability of the insole. Demographic (age, gender, height, weight) and basic medical data (diabetes duration, HbA1c) were collected at the first visit to the orthopedic shoe-technician. The study was approved by the ethics committee of the Fulda University of Applied Sciences.
Statistical Analyses
For each patient, wearing time was calculated as hours per day as a marker of overall adherent behavior. In addition, the percentage of days in which the temperature never exceeded the predefined cutoff temperature was calculated for each patient. This way, the percentage of days on which the footwear was never worn could be calculated as a specific marker for nonadherence. To analyze when patients started to become nonadherent, biweekly intervals for each patient were defined. For each interval, the total wearing time was calculated. When patients did not wear their footwear at any time over the course of a 2-week interval, this interval was marked as the start of being nonadherent. By using biweekly intervals, fluctuations in adherent behavior were taken into account and a more stable period of nonadherence could be identified. Kaplan-Meier analysis then analyzed the time to the first incidence of such nonadherent behavior (ie, survival time). In a second analysis, gender was entered as a stratifying variable. Besides testing for statistical significance, Cramer’s V was calculated as a measure of the effect size of possible gender effects.
Results
Cutoff Temperature for Wearing
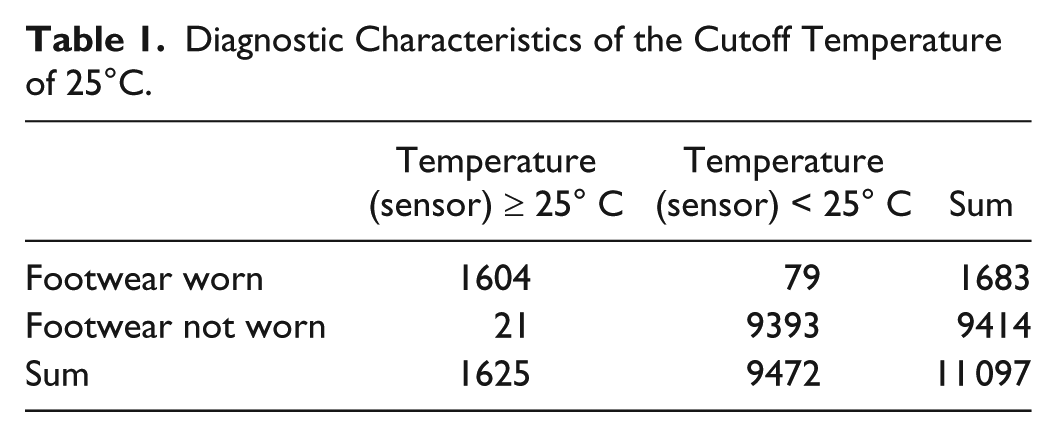
A total of 11 097 data points from volunteers without diabetes could be analyzed. The ROC analysis revealed an area under the curve of .996 (P < .0001; Figure 1). Therefore, wearing time of the customized diabetic insoles could be adequately monitored by measuring the temperature inside the footwear. Subsequently, a cutoff value of 25°C was determined that achieved a sensitivity of 95.3%, a specificity of 99.8%, a positive predictive value of 98.7%, and a negative predictive value of 99.2% (Table 1). Furthermore, based on this cutoff, the distribution of temperature values when the footwear was worn can be clearly distinguished from the distribution of temperature values when the footwear was not worn (Figure 2).
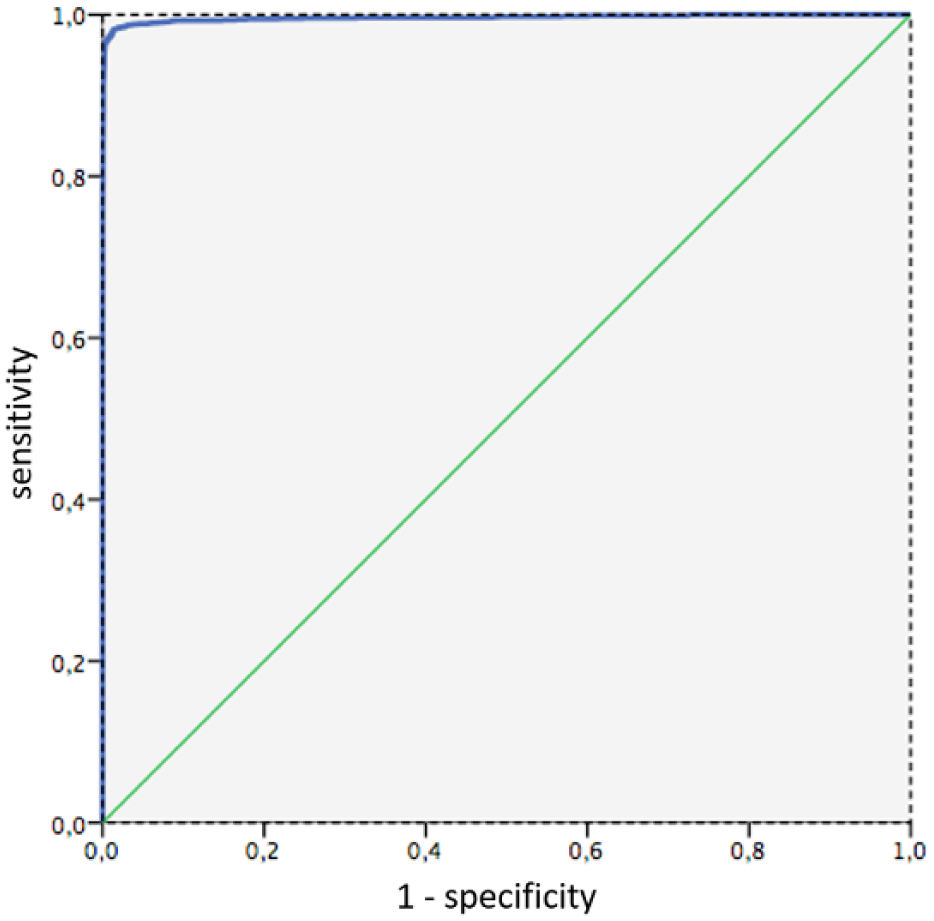
ROC curve for the diagnostic performance of temperature.
Diagnostic Characteristics of the Cutoff Temperature of 25°C.
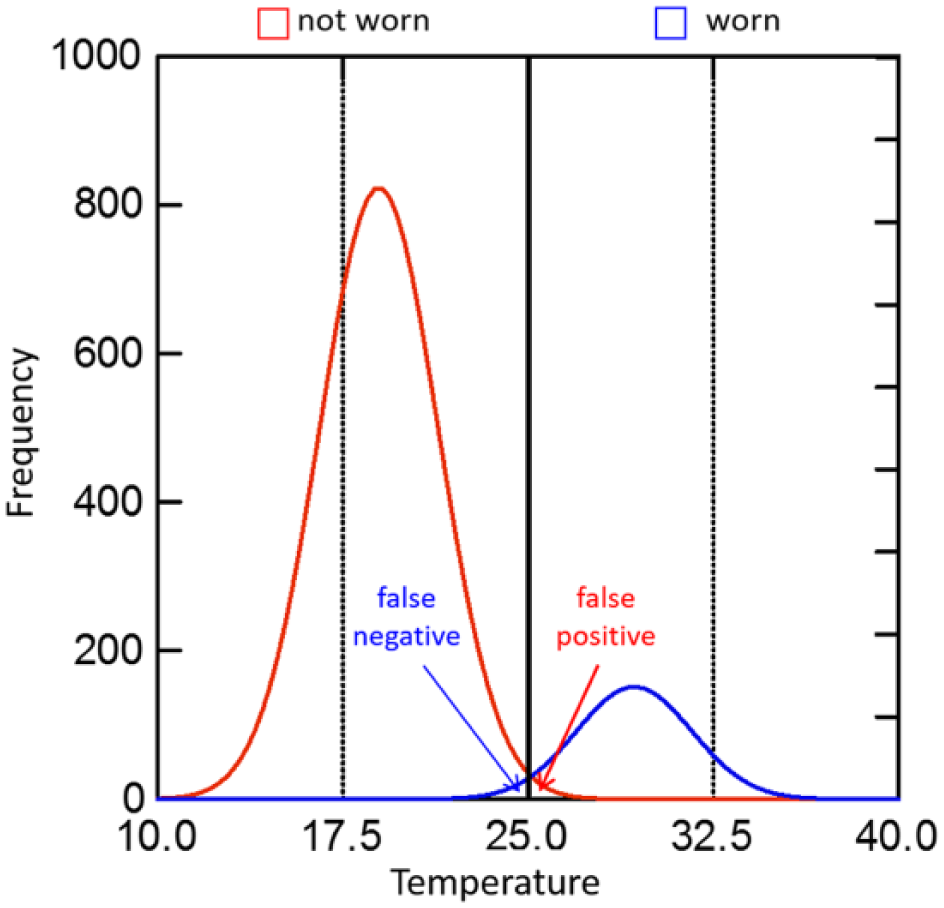
Distribution of the frequency of temperatures when footwear was worn versus not worn.
Adherence
A total of 26 patients with type 2 diabetes could be analyzed. As expected, patients were older, with a mean age of 67 years and a mean diabetes duration of 10 years (see Table 2). On average, data from 133.5 days per patient could be analyzed. Over this total observation period, mean wearing time was 4.2 ± 3.6 h/day. Due to the limited sample size, the median was also calculated that revealed an average wearing time of 3.4 h/day. The interquartile range (IQR) was rather wide, ranging from 0.5 to 7.0 h/day. Women and men did not differ with regard to the total observation period.
Sample Characteristics.
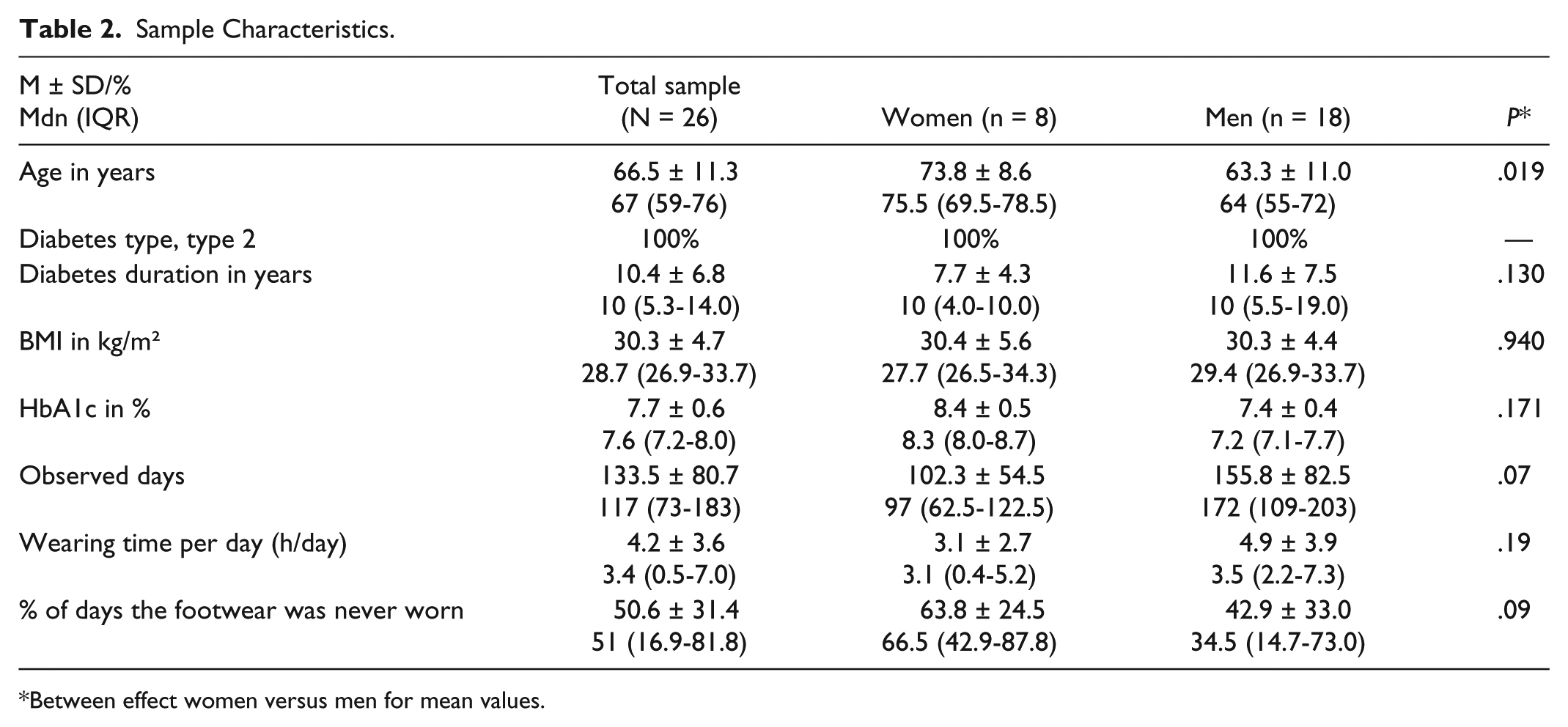
Between effect women versus men for mean values.
On an average of 51% of days, the temperature inside the shoe never exceeded 24.9°C. This indicates that patients did not wear their diabetic footwear at all on half of their observed days. Excluding those days from the analysis, a mean wearing time of 6.9 ± 3.7 h/day (Mdn = 7.1 h/day, IQR = 3.8-8.9) resulted.
Kaplan-Meier analysis revealed a mean survival time of 13.75 biweekly intervals. This indicates that the mean time of adherent behavior lasted 27.5 weeks. As can be seen in Figure 3, adherent behavior lasted 10 and 15 biweekly intervals for 53% and 35% of the studied patients, respectively. Gender effects on adherence can be seen in Figure 4. Mean survival time for men was 15.21 biweekly intervals and 6.91 biweekly intervals for women, χ2(1) = 2.13, P = .145. Thus, after just 14 weeks, women started to become nonadherent compared to 30.5 weeks for men. This difference failed to reach significance but yielded a moderate effect size of Cramer’s V = 0.42.
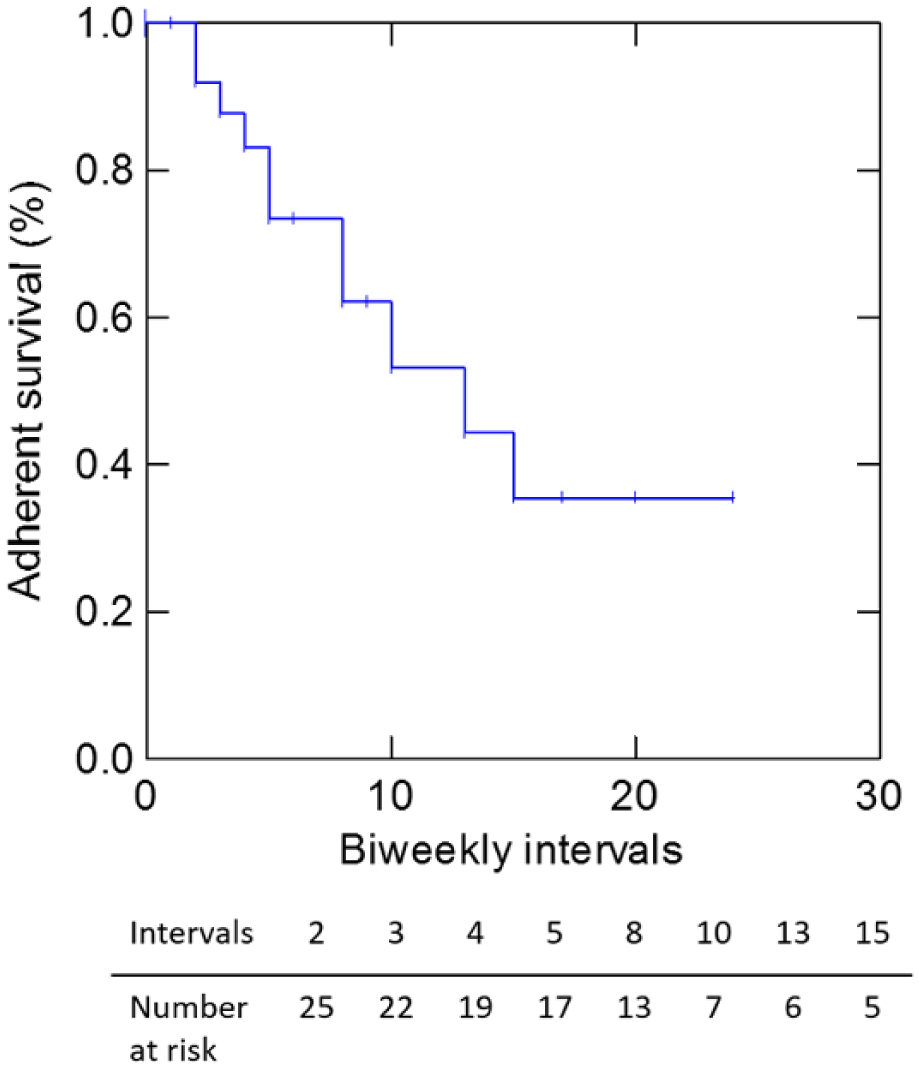
Kaplan-Meier curve for the time until the beginning of nonadherent behavior (not wearing the footwear for two straight weeks) for all patients.
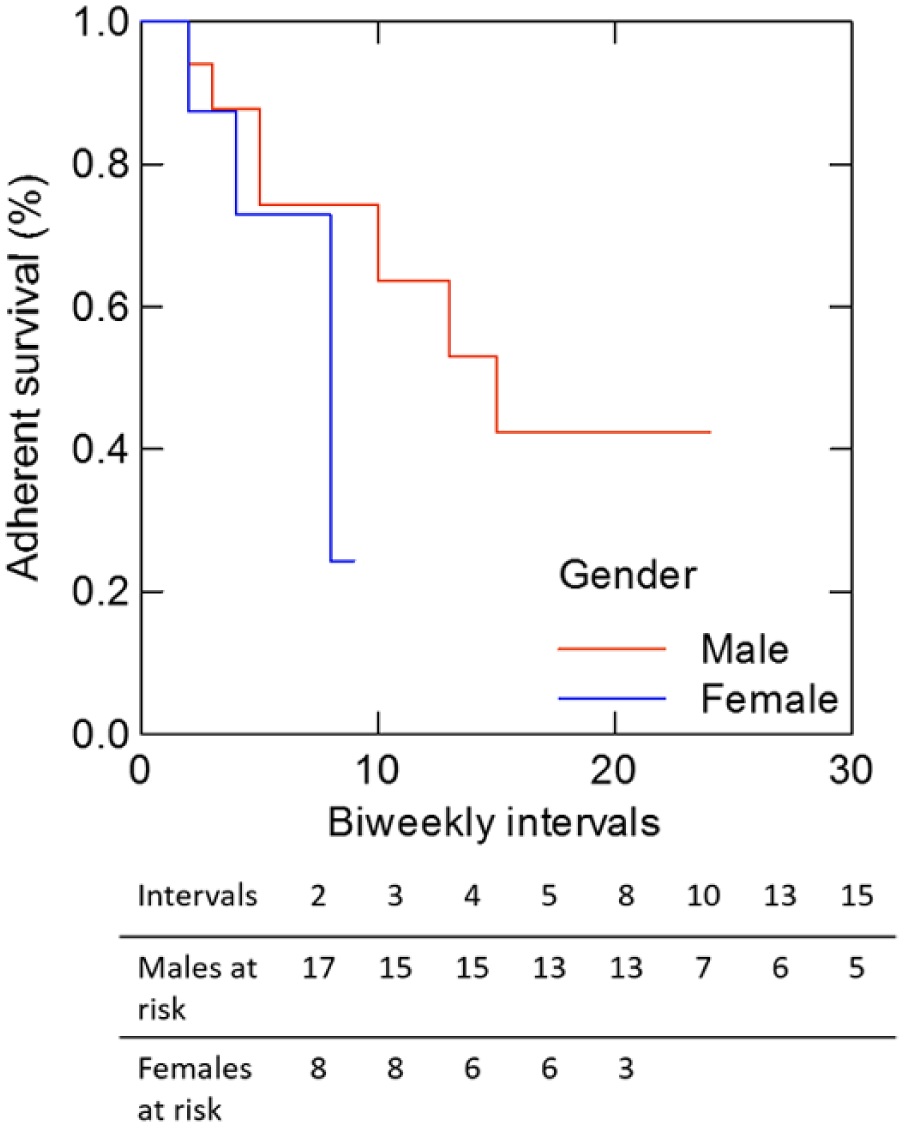
Kaplan-Meier curves for the time until the beginning of nonadherent behavior (not wearing the footwear for two straight weeks) for women and men.
Discussion
For the first time, the study offers continuous data of wearing behavior of diabetic footwear over a longer period of time in patients at high risk for serious diabetic foot problems. By using a temperature sensor, objective data on patients’ wearing behavior could be analyzed. It was not only possible to calculate the hours per day the footwear was worn but also the percentage of days the footwear was never put on. Results suggest that the overall wearing time was rather low as patients have only worn their footwear for about 4 hours a day. Furthermore, as the percentage of days on which the temperature inside the shoe never exceeded 24.9°C indicates, patients never have worn their footwear half of the time. Based on the low wearing time together with the overall unwillingness to put the footwear on in the first place, the adherence can be regarded as low. Overall, adherence substantially dropped after 27.5 weeks. Thus, the long-term preventive effect of the diabetic footwear can be questioned. However, it is important to note that no reulceration occurred during the observation period. Interestingly, there was a medium-sized gender effect on the beginning of nonadherence that showed that mean “survival time” for men was doubled compared to women. Kaplan-Meier curves hinted at the trend that women have more problems with being adherent for a longer time. While there was no statistically significant gender effect, probably due to the lack of power, the effect size of Cramer’s V = 0.42 indicates that this might be a clinically important effect that deserves further investigation. Also, the nature of this effect should be a focus of further studies on adherence. A possible explanation could be that women gather more negative experiences with the footwear over time (eg, social perceptions). 21
Nonetheless, these findings demonstrate the importance of an ongoing support of diabetes patients with foot problems by health care professionals. This support should not only focus on medical examinations and asking patients whether they were being adherent, but rather on educational and motivational aspects to foster or increase adherence. A central aspect of being adherent is to understand the urgency and the need for the diabetic footwear. In addition, patients need to grasp the utility and the benefit of the prescribed footwear. Therefore, interventional strategies are needed that educate patients about diabetic foot problems and possible interventions. These educational concepts should also discuss possible reasons for nonadherence. Furthermore, family members should also be informed and educated about the prescribed footwear and the risks of diabetes foot problems. The sensor technology could also be used to improve adherence by providing feedback to the patients or directly to the health care provider. 3 The health care provider could then use the adherence data to tailor intervention strategies. However, this approach is accompanied with ethical issues that need to be resolved such as ownership and access to the data. 24 When interpreting the study, the following limitations should be considered. First, no step activity monitor was used. Therefore, no inferences can be made regarding how often and how long patients were active and whether the footwear was worn during those activity periods. However, the use of a step activity monitor over such a long period of time would have been difficult to implement. Furthermore, such an externally worn monitor could have led to a rather reactive observation in which patients would have been constantly aware that there were being monitored. The current approach was rather covert as patients could not see or feel the temperature sensor and were not reminded of it. Second, only a limited number of patients could be included. This is due to the fact that we only wanted to include patients after the first occurrence of an ulceration. Subsequently, only patients with their first prescribed insoles were analyzed, which in turn guaranteed that patients did not already have other footwear at home. However, the results might not be generalizable to patients with more experience with reulceration; since these patients might behave differently and show more or less adherent behavior. Similarly, only a small number of women could be analyzed. Thus, the gender effect must be regarded as preliminary. Nevertheless, the gender effect seems clinically relevant as indicated by the effect size; thus, further research on the gender-specific courses of adherence to diabetes footwear is needed to address this preliminary gender effect. Although, the validity of the cutoff temperature was evaluated, we cannot completely rule out the possibility that the temperature inside the shoe exceeded 24.9°C due to environmental factors (eg, sun, overheated rooms). However, we recorded just 21 out of 1625 instances in which the temperature exceeded 24.9°C without the footwear being worn (see Table 1); thus, the risk for false positive events seemed to be rather low.
Conclusions
In summary, the course of wearing time and willingness to wear diabetic footwear showed clear room for improvement. This has major consequences with regard to possible preventive effects of the footwear. The prevention of serious diabetic foot problems, such as amputation, is not just of medical and psychological importance, but also has health-economic consequences. The costs of an amputation add up to €20 000 to €25 000 with additional annual costs of up to €3500. 25 Customized diabetic footwear seems to be an effective strategy but it all comes down to patients actually wearing their prescribed footwear. Hence, continuous monitoring of patients’ behavior could be an effective means for an early detection of adherence problems which would then allow for a timely intervention. Continuous adherence monitoring combined with specific feedback strategies can be a promising way to improve adherence in the long-term, thereby making a substantial contribution to the prevention of diabetic foot problems.
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to Bornmann und Schroeder Orthopaedie, who helped with data collection.
Abbreviations
IQR, interquartile range; ROC, receiver operating characteristic.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DE, DN, TH, BK, and NH have no conflict of interest to disclose. MS and MJ are employees of IETEC foot orthotics GmbH, which was responsible for manufacturing the diabetic insoles used in this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project (HA project 331/12-21) is funded in the framework of Hessen Modell-Projekte, financed with funds of LOEWE—Landes-Offensive zur Entwicklung Wissenschaftlich-oekonomischer Exzellenz, Foerderlinie 3: KMU-Verbundvorhaben (State Offensive for the Development of Scientific and Economic Excellence).