
Abstract
Adhesives used for continuous glucose monitoring (CGM) devices can cause skin irritations, which sometimes lead to abandonment of the therapy. A previous sensor manufacturing process involved two separate adhesives—one applied to the skin-facing surface of the fabric patch, and a second, ethyl cyanoacrylate-based adhesive, which secured the plastic transmitter housing to the superficial side of the patch. Our current process for attaching the transmitter housing to the fabric patch uses heatstaking, wherein the housing is heated and pressed against the patch with a specialized assembly apparatus. Heatstaking simplifies the sensor assembly process and obviates the need for the second adhesive, which may lead to lower risk of skin irritation(s) in some patients.
Keywords
Medical adhesives are widely used in inpatient and outpatient settings, and hypersensitivity to them represents a particular challenge to users of continuous subcutaneous insulin infusion (CSII) equipment or continuous glucose monitoring (CGM) devices. 1 In some cases, acrylate-based adhesives used for assembly of CGM sensors, usually worn for prolonged periods, can cause skin hypersensitization, resulting in allergic contact dermatitis (ACD). If the reaction is severe or intractable, patients may abandon the CSII and/or CGM devices in favor of insulin injections and capillary blood glucose testing.
The central structural component of Dexcom G4 PLATINUM / G5 Mobile sensor assemblies (Dexcom, Inc, San Diego, CA) is a polyester spunlace fabric patch with adhesive on the skin-facing side and a plastic transmitter housing on the superficial side. The transmitter housing is flexible enough to allow for insertion and eventual removal of the transmitter, but rigid enough to hold the transmitter securely during normal use. A previous manufacturing process included a liquid cyanoacrylate-based glue applied to the housing, which was then affixed to the fabric patch. The resulting pattern of glue is visible on the skin-facing surface of the fabric patch (Figure 1A). The current manufacturing process involves heatstaking, where heat and pressure are applied to the pieces to be bonded. The resulting pattern of attachment points corresponds to the areas of the housing that were heated and is visible on the skin-facing surface of the patch (Figure 1B). Importantly, heatstaking does not rely on a chemically distinct glue and is amenable to automation.
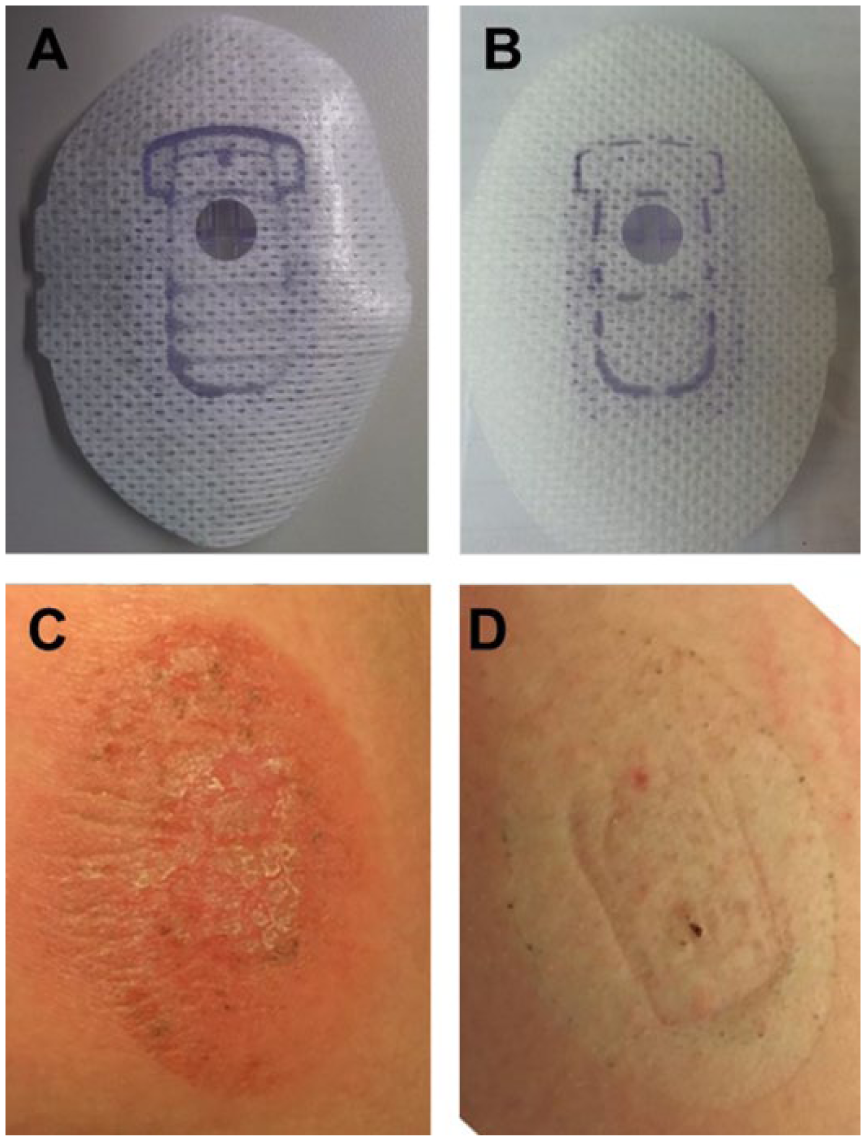
Upper panels show skin-facing surfaces of patches made with the cyanoacrylate-based adhesive (A) and the heatstaking process (B). Lower panels show skin exposed to a cyanoacrylate-containing patch (C) or the heatstaked patch (D).
A patient sequentially exposed to both types of patches allows for limited comparison of corresponding skin reactions. The case was reported to Dexcom’s postmarketing surveillance program on four separate occasions in 2016; all of the complaints were associated with patches that were manufactured with the cyanoacrylate-containing glue. The skin reaction to one of these patches (Figure 1C) included erythema and excoriation. To our knowledge, no diagnostic patch testing was performed. In early 2017, the patient was provided with sensors that were manufactured using the heatstaking process. After a period of normal use and removal of one of these sensors, a photo of the underlying skin (Figure 1D) was provided. The heatstaked sensor was reported to have produced no skin reaction.
Anecdotal and peer-reviewed reports suggest that adhesive failures or skin reactions are an important reason for discontinuation of CGM,1,2 and satisfactory adhesion (adequate stickiness with minimal skin irritation) can significantly improve the tolerability of CGM devices. 3 Because the benefits of CGM systems depend to a large extent on the proportion of time that they are worn,4,5 many patients wear them almost constantly, thereby increasing the risk of adhesive-related adverse skin events. In the cases involving Dexcom sensors reported here and elsewhere,6,7 ethyl cyanoacrylate used to adhere the transmitter housing to the superficial surface of the patch, even though not in the adhesive directly in contact with the skin, may have caused unintended sensitization. Pressure-sensitive acrylate-based adhesives employed in other continuously-worn glucose monitoring systems 8 and other cyanoacrylate-based adhesives9-11 have also been implicated in ACD reactions. The recently-changed manufacturing process described here has eliminated the ethyl cyanoacrylate adhesive. As shown here and reported elsewhere, 7 the new sensors were associated with less skin reactions.
Cyanoacrylate-based adhesives are an important class of medical adhesives to consider in cases of ACD related to glucose sensors and insulin infusion sets. Patch testing is a straightforward diagnostic method in such cases, and would contribute to our knowledge of the safety of medical device adhesives if routinely implemented. Sensors made using the heatstaking process may lessen the potential for cyanoacrylate exposure and allow some patients to resume or continue sensor wear with less risk of cutaneous sensitization and skin reactions.
Footnotes
Abbreviations
ACD, allergic contact dermatitis; CGM, continuous glucose monitoring; CSII, continuous subcutaneous insulin infusion.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors are employees of Dexcom, Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.