
Abstract
Background:
The association of glucose variability (GV) with other glycemic measures is emerging as a topic of interest. The aim of this analysis is to study the correlation between GV and measures of glycemic control, such as glycated hemoglobin (HbA1c) and daily mean glucose (DMG).
Methods:
Data from 5 phase 3 trials were pooled into 3 analysis groups: type 2 diabetes (T2D) treated with basal insulin only, T2D treated with basal-bolus therapy, and type 1 diabetes (T1D). A generalized boosted model was used post hoc to assess the relationship of the following variables with glycemic control parameters (HbA1c and DMG): within-day GV, between-day GV (calculated using self-monitored blood glucose and fasting blood glucose [FBG]), hypoglycemia rate, and certain baseline characteristics.
Results:
Within-day GV (calculated using standard deviation [SD]) was found to have a significant influence on endpoints HbA1c and DMG in all 3 patient groups. Between-day GV from FBG (calculated using SD), within-day GV (calculated using coefficient of variation), and hypoglycemia rate were found to significantly influence the endpoint HbA1c in the T2D basal-only group.
Conclusions:
Lower within-day GV was significantly associated with improvement in DMG and HbA1c. This finding suggests that GV could be a marker in the early phases of new antihyperglycemic therapy development for predicting clinical outcomes in terms of HbA1c and DMG.
The pivotal goal of diabetes treatment is to prevent or minimize the acute and chronic complications of diabetes by maintaining normo- or near-normoglycemia. Hypoglycemia is a major limitation in achieving glycemic goals in patients with diabetes, especially for patients with type 1 diabetes (T1D).1,2
Glycated hemoglobin (HbA1c) is the gold standard metric for assessing diabetes control. However, HbA1c is an indirect measure of the average blood glucose and there is some evidence to suggest that HbA1c alone may not be sufficient to completely assess the metabolic status of patients with diabetes.3,4
Recently, the association of glucose variability (GV) with standard glycemic control parameters, such as HbA1c and daily mean glucose (DMG), hypoglycemia, and long-term complications of diabetes has been a topic of interest. It has been observed that patients with similar HbA1c and DMG values can have remarkably different within-day or between-day GV. 5 The possibility of an association between GV and complications of diabetes is supported by the hypothesis that oxidative stress, which is considered to be a mediator of diabetic complications, is greater with intermittent hyperglycemia as compared to sustained hyperglycemia;6,7 however, this association is controversial. 5 Previous studies have suggested that patients with greater GV are at higher risk of developing hypoglycemia. 8 Both within-day and between-day GV have been significantly associated with the risk of hypoglycemia in patients with type 2 diabetes (T2D) receiving insulin, even after adjusting for HbA1c and DMG. 9
In previous studies, several measures have been used to measure GV. These include standard deviation (SD), mean amplitude of glycemic excursions (MAGE), mean absolute glucose (MAG), coefficient of variation (CV), high blood glucose index (HBGI), low blood glucose index (LBGI), and average daily risk range (ADRR). Simulations have demonstrated that all GV measurements are highly correlated with each other. 10 A study evaluating the relationship of GV with hypoglycemia showed that CV was the most significant predictor, while MAGE, MAG, and ADRR were not significant predictors of hypoglycemia, in a gradient boosting method for relative influence of input variables. 9
Currently, there is limited research to quantify the relationship of GV with HbA1c. In the early phases of insulin development, it is difficult to predict the effect of GV on HbA1c. Larger studies and longer follow-up is required to observe an effect on HbA1c.
The aim of this analysis was to further evaluate the correlation between GV and established measures of glycemic control, such as HbA1c and DMG using a large dataset comprising 5 phase 3 insulin studies. Specifically, we wished to understand the role of within-day or between-day GV in relation to HbA1c and DMG. In all these studies, basal insulin peglispro (BIL) demonstrated greater HbA1c reduction with lower between-day GV as compared with insulin glargine (GL); 4 out of 5 studies demonstrated that BIL also had lower within-day GV as compared to GL.11-15 We hypothesized that greater HbA1c reduction with BIL as compared to GL may be partially attributed to lower GV with BIL. Therefore, this post hoc analysis was conducted using pooled data from these 5 phase 3 IMAGINE trials to examine whether a change in GV could influence glycemic control endpoints such as HbA1c and DMG.
Research Design and Methods
Study Design
Data from 5 BIL phase 3 trials with GL as the active comparator were combined across treatments and pooled into 3 post hoc analysis groups: T2D patients treated with basal insulin only (IMAGINE 214 and IMAGINE 513); T2D patients treated with basal-bolus therapy (IMAGINE 412); and T1D patients (IMAGINE 115 and IMAGINE 311).
Table 1 provides the key features of the 5 BIL trials. All studies were conducted in accordance with the International Conference on Harmonization Guidelines for Good Clinical Practice and the Declaration of Helsinki. All patients provided informed consent, and the protocols and consent documents were approved by the local ethical review boards prior to study initiation. These studies were registered at clinicaltrials.gov as follows: NCT01435616, NCT01468987, NCT01481779, NCT01454284, and NCT01582451. Patients were randomized to BIL or GL basal insulin treatment alone (IMAGINE 2 and 5) or in combination with prandial insulin lispro (IMAGINE 1, 3, and 4). The detailed study designs, baseline characteristics, efficacy, and safety results have been previously published.11-15
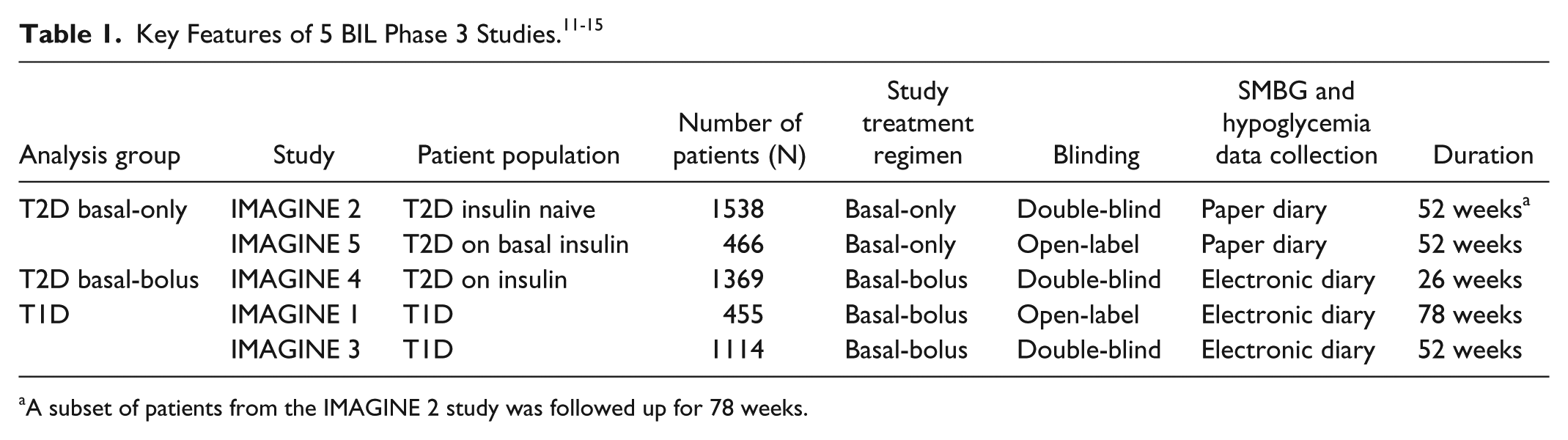
A subset of patients from the IMAGINE 2 study was followed up for 78 weeks.
Patients used study-provided blood glucose meters to perform 6- to 9-point self-monitored blood glucose (SMBG) profiles (6-point SMBG for T2D basal-only patients: fasting, pre-midday meal, pre-evening meal, bedtime, 03:00 hours, and next day fasting; 9-point SMBG for T2D basal-bolus and T1D patients: 2 hours post-morning/midday/evening meal added to the 6-point profile) on 2 nonconsecutive days in the week prior to prespecified visits. In addition, patients in basal-bolus studies checked 4-point profiles (fasting, pre-midday/evening meal, bedtime) every day and patients in basal-only studies checked fasting self-monitored blood glucose (FBG) every day. Patients used study-provided paper diaries (IMAGINE 2 and 5) or electronic diaries 16 (IMAGINE 1, 3, and 4) to record SMBG profiles, FBG values, and hypoglycemic events. HbA1c was obtained at study endpoint (measured by a central laboratory), whereas DMG was calculated as the mean of the average glucose value over the 2 SMBG profiles measured on 2 nonconsecutive days. Hypoglycemia was defined as SMBG ≤70 mg/dL or presence of hypoglycemia signs and symptoms.
Three GV parameters were considered for the purpose of this analysis: within-day GV from SMBG, between-day GV from SMBG, and between-day GV from FBG. Each of the 3 GV measures was calculated as both SD of the glucose values and CV. The between-day GV from SMBG was calculated in 2 steps: (1) GV at each time point calculated from 2 values from 2 nonconsecutive days; (2) between-day GV from SMBG calculated by averaging GVs over 6-9 SMBG time points.
Statistical Methods
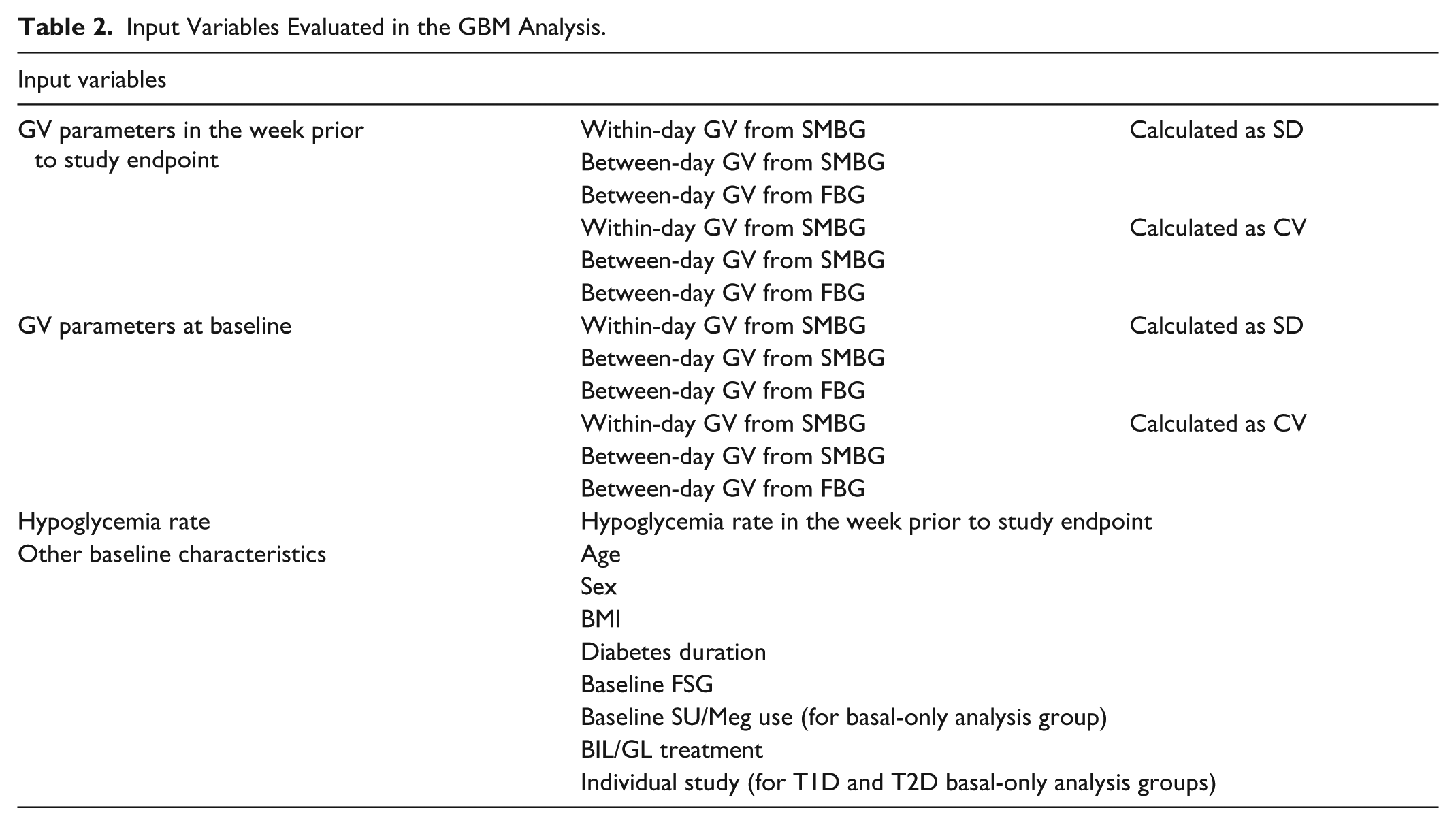
The main statistical approach is to investigate the relationship of GV and glycemic control parameters such as the endpoint HbA1c and DMG, which were measured after 26-52 weeks of treatment with BIL or GL. Therefore, the endpoints HbA1c and DMG were the outcomes in these analyses. With respect to the input variables, first, all the aforementioned GV measurements at baseline and in the week prior to study endpoint were included; second, other baseline characteristics which may be related to HbA1c and DMG were also included; third, the hypoglycemia rate in the week prior to endpoint HbA1c and DMG was also considered as an input variable since it was believed to have impact on glycemic control (Table 2).
Input Variables Evaluated in the GBM Analysis.
Due to the high correlation among these variables, a multiple linear regression could cause serious collinearity issues and might be an inappropriate statistical method in this analysis. In this research, a generalized boosted model (GBM)17,18 was used to assess the relationship between GV and HbA1c or DMG. The main advantage of a GBM model is that it can automatically consider the interaction effects among all input variables. Therefore, it is much more accurate than the traditionally used multiple regression models. In addition, the GBM model is more robust and reliable in selecting important predictors than multiple regression models when collinearity exists among these variables. For each of the input variables, GBM calculated its relative influence on endpoints HbA1c or DMG. The relative influence quantified the proportion of capability in prediction of HbA1c or DMG for each input variable and would sum up to 100% over all the variables. A permutation test was then applied to estimate the P value of the relative influence. An input variable with statistically significant P value of <.05 was considered as a predictor of the endpoint HbA1c or DMG. A multiple regression analysis was then used to further evaluate the influence of selected predictors on HbA1c and DMG. If multiple within-day or between-day GV measures were considered statistically significant based on the GBM model, the one with more relative influence was included in the multiple regression analysis.
The statistical analysis for GBM was carried out in R (3.1.1) with R package GBM (1.6-3.1). Multiple regression was performed using SAS 9.2 (SAS Institute, Cary, NC).
Results
This analysis included 4942 patients divided into 3 analysis groups: T2D patients treated with basal insulin only (N = 2004), T2D patients treated with basal-bolus therapy (N = 1369), and T1D patients (N = 1569). Baseline characteristics of these 3 analysis groups have been summarized in Table 3.
Demographics and Baseline Characteristics in the 3 Analysis Groups.
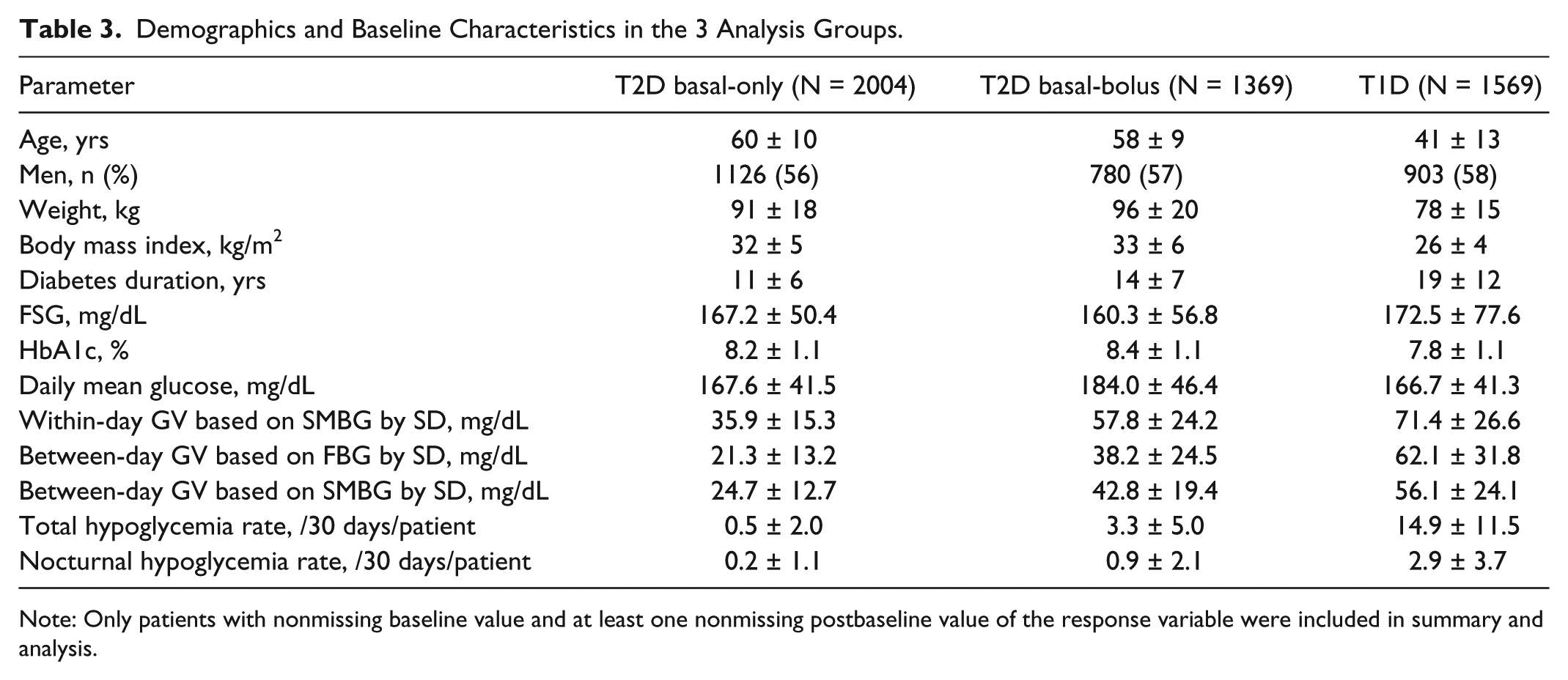
Note: Only patients with nonmissing baseline value and at least one nonmissing postbaseline value of the response variable were included in summary and analysis.
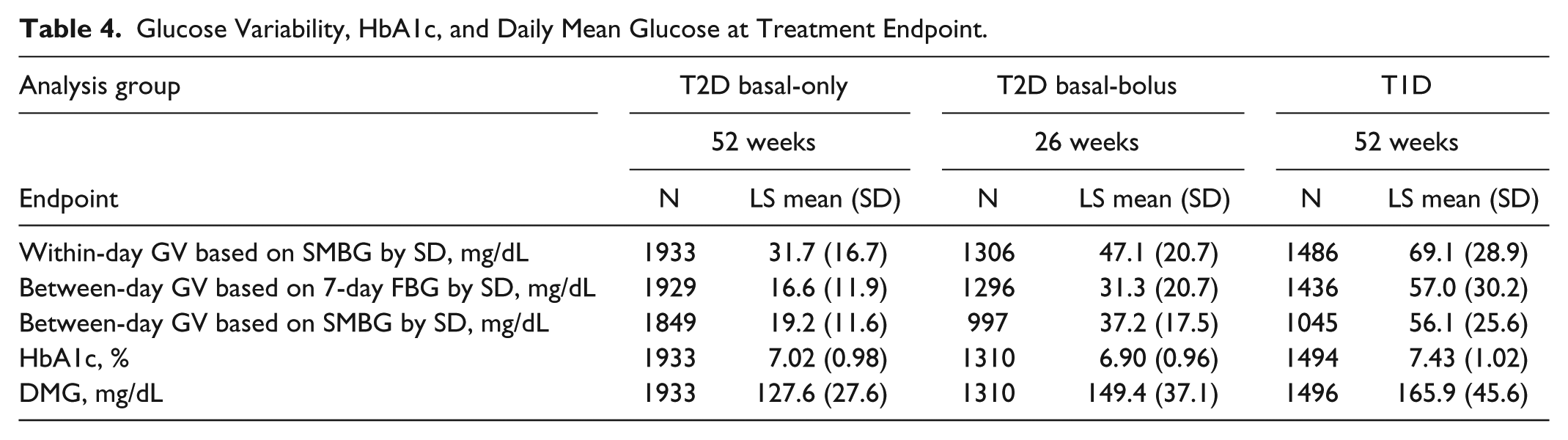
Table 4 shows the GV, HbA1c, and DMG values observed in each of the 3 analysis populations at treatment endpoint.
Glucose Variability, HbA1c, and Daily Mean Glucose at Treatment Endpoint.
Influence of Input Variables on Glycated Hemoglobin
Figure 1 shows the relative influence of input variables on HbA1c at treatment endpoint as evaluated by the GBM analysis.
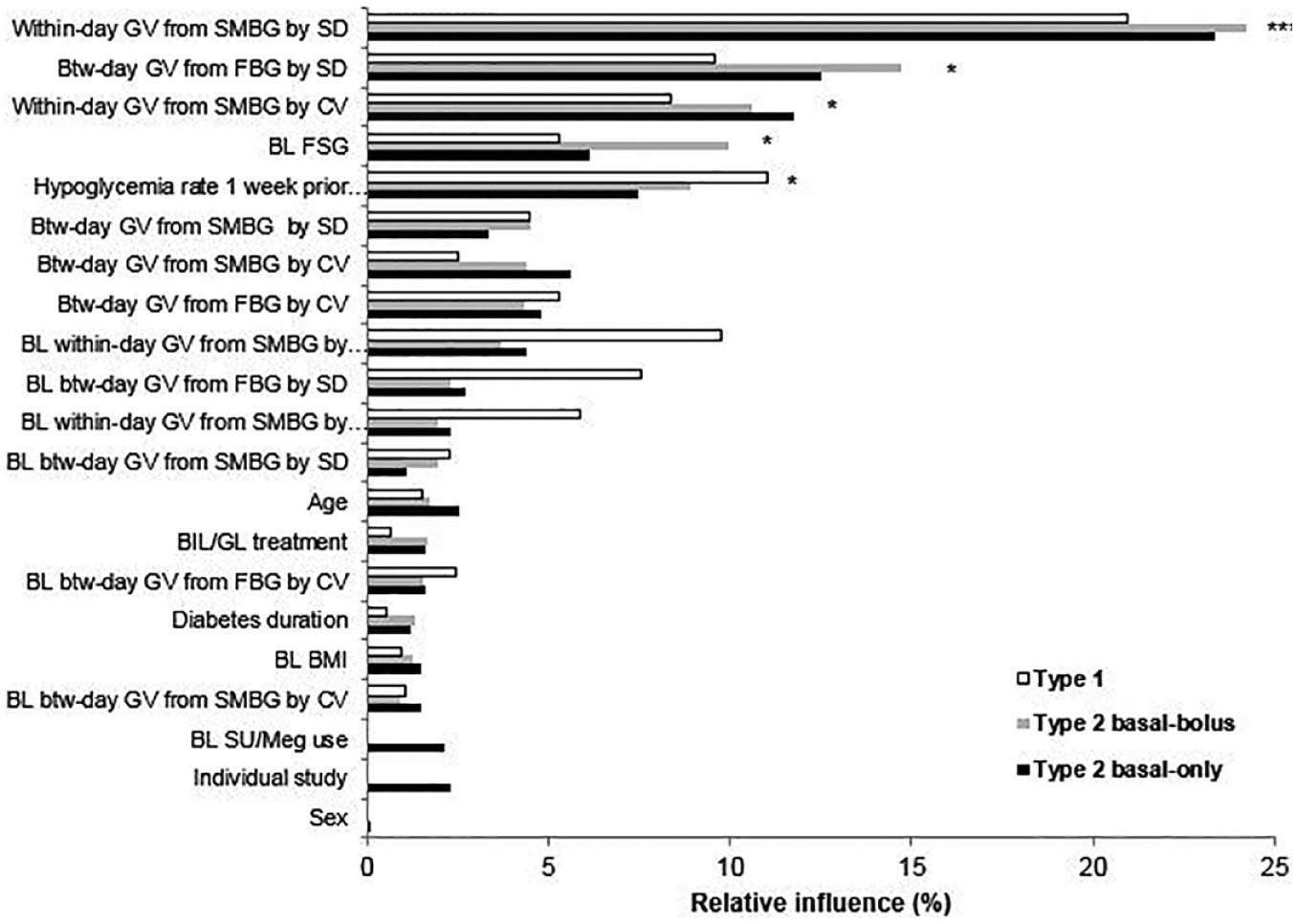
Order of relative influence of input variables on endpoint HbA1c.
Among the GV parameters evaluated in the week prior to endpoint, within-day GV assessed by SD was found to have a significant influence on endpoint HbA1c in all 3 analysis groups. The relative influence ranged from 21% to 24% among the 3 analysis groups. Other GV parameters which had a significant influence on endpoint HbA1c in the T2D basal-only group included: between-day GV from FBG by SD and within-day GV from SMBG by CV.
None of the baseline GV parameters were found to affect endpoint HbA1c.
Hypoglycemia rate in the week prior to study endpoint was found to significantly influence the endpoint HbA1c in the T2D basal-only group.
Among the other baseline parameters evaluated, only baseline central laboratory fasting serum glucose (FSG) was found to have a significant influence on endpoint HbA1c in the T2D basal-only group.
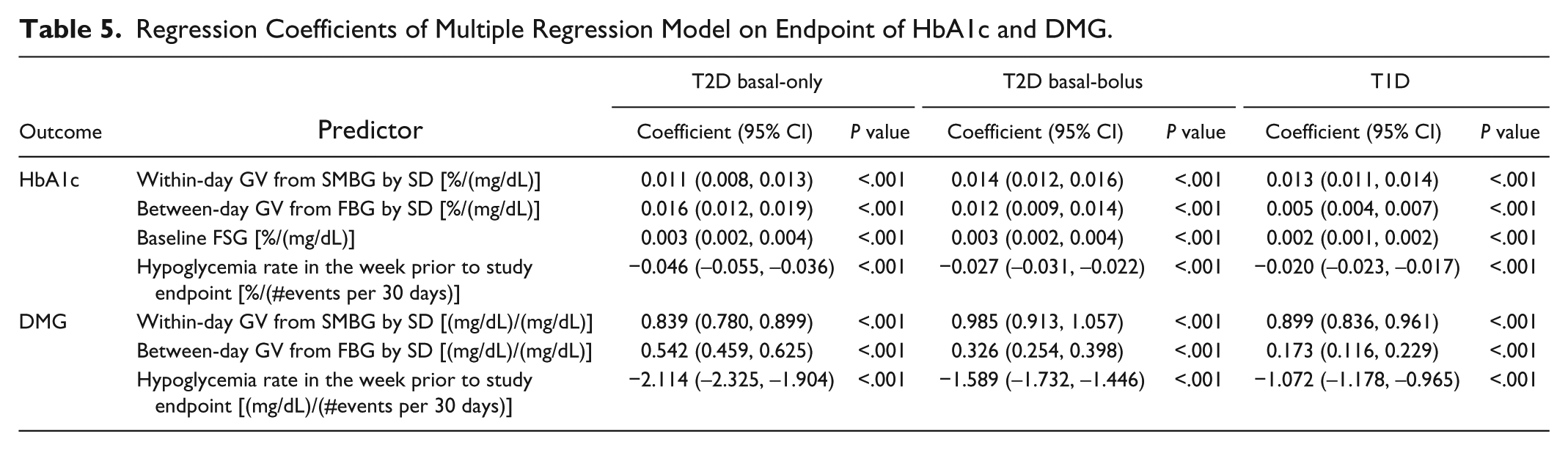
Since the GBM model identified within-day GV by SD, between-day GV from FBG by SD, baseline FSG, and hypoglycemia rate in the week prior to study endpoint as key predictors of endpoint HbA1c, we conducted a multiple regression analysis to further evaluate the prediction effects of these variables on HbA1c in all the 3 analysis populations (Table 5). This analysis showed that a decrease of 30 mg/dL in within-day GV by SD would reduce HbA1c by 0.33%-0.42% (P < .001 in all 3 populations). Reduction in between-day GV from FBG by SD and baseline FSG were also directly related to HbA1c reduction (all P < .001). Furthermore, the hypoglycemia rate in the week prior to study endpoint was inversely related to HbA1c.
Regression Coefficients of Multiple Regression Model on Endpoint of HbA1c and DMG.
Influence of Input Variables on Daily Mean Glucose
Figure 2 shows the relative influence of input variables on endpoint DMG.
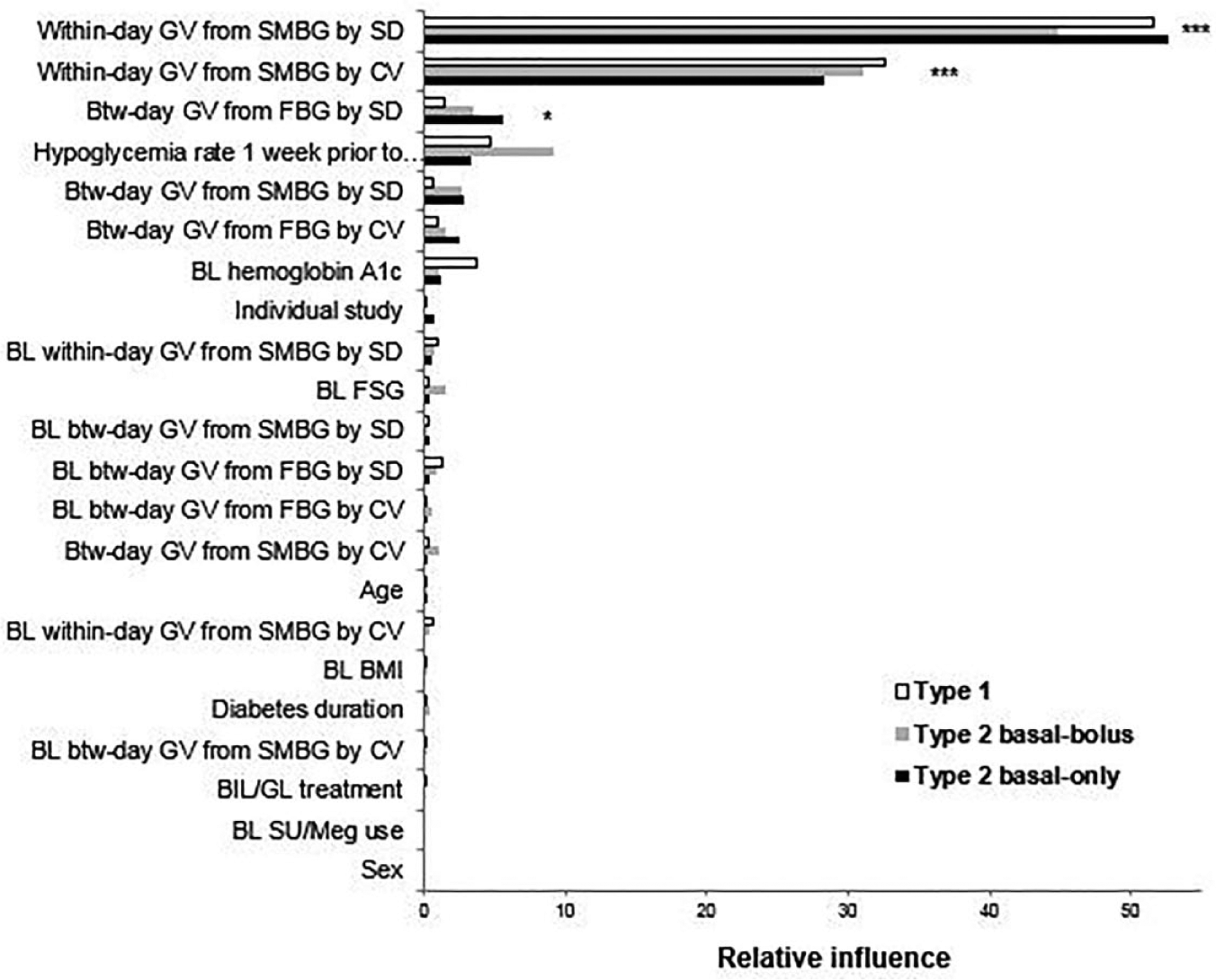
Order of relative influence of input variables on endpoint daily mean glucose.
Among the GV parameters evaluated in the week prior to endpoint, within-day GV by SD was identified as the top influencer in all the 3 populations. It accounted for >50% influence on DMG among all the input variables analyzed in the T2D basal-only and T1D populations and 44% influence in the T2D basal-bolus population (P < .001 for all 3 analysis populations). Between-day GV from FBG by SD was found to influence endpoint DMG in the T2D basal-only group.
None of the other input variables evaluated were found to have a significant influence on endpoint DMG.
We conducted a multiple regression analysis to evaluate the prediction effects of selected variables from the GBM model on endpoint DMG (Table 5). This analysis showed that a decrease in within-day GV by SD of 1 mg/dL would lower DMG by 0.8-1.0 mg/dL. Reduction in between-day GV from FBG by SD was also directly related to DMG reduction in all the 3 groups (all P < .001). Similarly, as observed with HbA1c, the hypoglycemia rate in the week prior to study endpoint was inversely related to DMG.
Discussion
Our analysis identified within-day GV (measured using SD in the week prior to study endpoint) as the most important influencer of endpoint HbA1c as well as DMG. Between-day GV from FBG by SD and hypoglycemia rate in the week prior to endpoint were also identified as potential influencers.
It is possible that the lower within-day GV may have been a consequence of reduction in HbA1c and DMG rather than a predictor of lower HbA1c and DMG, since a lower mean glucose and HbA1c may translate into decreased GV. However, it should be noted that the within-day GV by CV, which is adjusted for mean glucose, was also a significant factor associated with HbA1c. This observation supports the hypothesis that within-day GV could be a predictor of HbA1c and DMG at endpoint. Furthermore, in the phase 3 studies analyzed, FBG for BIL-treated patients was similar to GL-treated patients at treatment endpoint, but the daytime glucose excursion was lower with BIL than with GL. This also suggests that the lower within-day GV with BIL accounted for the lower HbA1c observed with BIL.11-15
A uniform reduction of the individual SMBG values of the diurnal profile would reduce the DMG and HbA1c values; however, this would not result in a decrease in within-day GV, which is the key observation of this analysis. For example, in the IMAGINE 5 study, the endpoint HbA1c and DMG for patients treated with GL was lower compared to baseline with the intensification of GL therapy, but the overall SMBG profile was shifted downward and GV was not decreased (LS mean change from baseline for within-day GV SD: –0.41 mg/dL, P = .74; LS mean change from baseline for within-day GV by CV: 1.9%, P = .015) (Data on file, Eli Lilly and Company).
Qu et al 9 evaluated the relationship of GV with hypoglycemia T2D patients. They found that both within-day and between-day GV by CV were significantly associated with the risk of hypoglycemia in T2D patients treated with insulin. However, within-day GV by CV was found to have the greatest relative influence on hypoglycemia rate. In addition, within-day GV by CV at baseline was also found to be associated with hypoglycemia rate at weeks 12 and 24. Kilpatrick et al 19 analyzed the Diabetes Control and Complications Trial database and found that within-day GV by SD was significantly associated with hypoglycemia in patients with T1D. The impact of within-day GV by CV and between-day GV was not assessed. The current analysis found that within-day GV by SD had the greatest influence on HbA1c and DMG. This finding as well as previous research suggests that within-day GV may play a more important role in glycemic control than between-day GV.
This hypothesis is further supported by the observations from the BEGIN trials in which insulin degludec did not show greater reduction in HbA1c compared to GL, in spite of significant improvement in between-day GV.20-22 Currently, there do not appear to be reports available regarding the impact of insulin degludec on within-day GV. However, in the 3 BEGIN trials, which compared insulin degludec with GL, the mean glucose values at individual time points were similar between insulin degludec and GL. This suggests that within-day GV may have been similar between the 2 treatments.20-22
In addition, it should be noted that within-day GV by CV was the most influential parameter on hypoglycemia in the analysis by Qu et al, 9 whereas within-day GV by SD was found to be the most influential parameter on endpoint HbA1c and DMG in this research. DMG is generally inversely related to hypoglycemia while GV by SD is positively correlated with hypoglycemia. Therefore, it is possible that within-day GV by CV could superimpose the effects of within-day GV by SD and DMG on hypoglycemia, as CV is mathematically calculated by dividing SD by DMG. This could explain why within-day GV by CV was more influential than within-day GV by SD on hypoglycemia. However, in the GBM model, as the influence of all variables is competitive in nature, within-day GV by CV had a much greater effect than within-day GV by SD on hypoglycemia. On the other hand, for HbA1c or DMG, the association with within-day GV by CV (which is calculated by dividing the SD by DMG) may be attenuated, compared to the association with within-day GV by SD.
Recently, GV has emerged as a target for treating diabetes. 23 This research as well as previous research on GV support the hypothesis that reducing GV may be beneficial in the treatment of diabetes. In addition, these findings may also be important considerations for clinical development of antidiabetes drugs with HbA1c and hypoglycemia as the targeted clinical outcomes.
It is generally believed that flat and consistent pharmacokinetic/pharmacodynamic (PK/PD) profiles result in less GV which may translate into better glycemic control and improved clinical outcomes (lower HbA1c and/or lower hypoglycemia). However, the quantitative relationships between these parameters are not yet clearly defined. Through this research and our previous research, 9 we have attempted to develop quantitative relationships between GV and glycemic control endpoints (HbA1c and hypoglycemia). As future research, it would be desirable to establish robust and reproducible quantitative relationships between preclinical and clinical PK/PD profiles, GV parameters, and glycemic control variables. This could enable prediction of the glycemic outcomes in late phase clinical development from preclinical and phase 1 clinical pharmacology studies where PK and PD are measured. This may help optimize the selection of drug candidates in the early development stage and potentially improve the efficiency of new insulin development.
There are several limitations to this research. First, this was based on a post hoc analysis; continuous glucose monitoring data was not collected in majority of patients in these trials and therefore was not included in this post hoc analysis. Hence, the results are only suggestive. Second, the association between GV and HbA1c was studied; however, a causal effect was not analyzed. Third, HbA1c is generally deemed to reflect the average glucose across 2-3 months, whereas the GV measurements were based on the SMBG data for the week prior to HbA1c measurements. Therefore, the analysis of DMG, which was based on the same days as the GV measurement, has an advantage compared to HbA1c. However, it should be noted that the variability in DMG is generally larger than HbA1c.
Conclusions
In conclusion, this post hoc analysis of 5 large phase 3 insulin studies showed that primarily lower within-day GV was significantly associated with improvement in DMG and HbA1c. This finding together with previous research suggests that GV could be a marker in the early phases of new therapy development for predicting clinical outcomes in terms of HbA1c, DMG, and hypoglycemia.
Footnotes
Acknowledgements
Medical writing support for this manuscript was provided by Sheetal Pradhan, MD, Eli Lilly and Company
Abbreviations
BIL, basal insulin peglispro; BMI, body mass index; CI, confidence interval; CV, coefficient of variation; DMG, daily mean glucose; FBG, fasting blood glucose; FSG, fasting serum glucose; GBM, generalized boosted model; GL, insulin glargine; GV, glucose variability; HbA1c, glycated hemoglobin; LS, least square; PD, pharmacodynamic; PK, pharmacokinetic; SD, standard deviation; SE, standard error; SMBG, self-monitored blood glucose; SU/Meg, sulfonylurea/meglitinide; T1D, type 1 diabetes; T2D, type 2 diabetes.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JL, YQ, QZ, AMC, and SJJ are employees and stockholders of Eli Lilly and Company.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Eli Lilly and Company.