
Abstract
The purpose of this study is to examine timing of meal insulin and further determine whether an association exists between timing of meal insulin and missed meal insulin doses. The cohort included 4768 T1D Exchange clinic registry participants <26 years with type 1 diabetes ≥1 year. Chi-square tests, t-tests, and regression were used to assess the relationship between participant characteristics and timing of meal insulin and missed meal doses, respectively. Timing of meal insulin and association with missed meal doses was analyzed using logistic regression. In all, 21% reported administering insulin several minutes before, 44% immediately before, 10% during, and 24% after meal. Participants who gave insulin prior to a meal had significantly lower HbA1c than those who gave insulin during or after meal (8.4% ± 1.5% vs 8.8% ± 1.6%, adjusted P < .001), but no significant association was observed regarding DKA events. Those who reported missing ≥1 insulin dose per week had higher HbA1c (9.8% ± 1.9% vs 8.3% ± 1.3%, adjusted P < .001) and were more likely to experience at least one DKA event (9% vs 5%, adjusted P = .001) compared with those who rarely missed a meal insulin dose. Participants who reported administering insulin during or after a meal were more likely to report missing ≥1 meal insulin dose per week compared with those who administered insulin before a meal (28% vs 14%, adjusted P < .001). Premeal insulin was associated with lower HbA1c and fewer missed meal insulin doses. Providers may use this information to discuss the benefits of premeal insulin on glycemic control and adherence to therapy.
Patients with type 1 diabetes must adhere to several daily tasks including blood glucose monitoring and insulin administration to achieve optimal glycemic control. Maximizing adherence to meal insulin is of substantial value given its effect on glycemic control1-3 since a pattern of missed meal insulin doses raises hemoglobin A1c (HbA1c) a clinically significant amount (0.8-1.5%).2,3 In a study by Burdick and colleagues, the most common reason for missing a meal insulin dose among adolescents and young adults with type 1 diabetes was forgetting to give the dose; 2 therefore, minimizing forgotten meal doses is crucial. This goal may be particularly important in adolescents and young adults with type 1 diabetes, as only 17% of participants 13-17 years old within the T1D Exchange clinic registry meet glycemic goals (HbA1c < 7.5% [58 mmol/mol]) set forth by the American Diabetes Association (ADA).1,4
One question not previously examined is whether giving insulin before a meal decreases the likelihood of missing a meal insulin dose. Although there are pharmacokinetic benefits to giving insulin before a meal (reduced post prandial glycemic excursion),5-7 it is unclear what percentage of patients give meal insulin before eating (patients may choose to give meal insulin before, during, or after a meal). Understanding how patients give their meal insulin, and whether premeal insulin administration is associated with improved adherence to therapy would allow providers to assess and improve adherence during routine office visits. Therefore, the purpose of this study is to examine the distribution of timing of meal insulin across T1D Exchange clinic registry participants and clinical centers, to determine factors associated with timing of meal insulin and missing meal insulin doses, and finally, to assess whether an association exists between timing of meal insulin and missed meal doses.
Methods
The T1D Exchange clinic registry (T1D Exchange) includes 74 endocrinology practices based in the United States, including 58 centers serving youth with type 1 diabetes. Details of the enrollment process, eligibility criteria, and baseline data collection have been previously reported. 8 Data were collected for the clinic registry central database from participants’ medical records in addition to comprehensive questionnaires completed by participants (or parents/guardians of participants <18 years). 8
The cohort includes 4768 participants younger than 26 years with a clinical diagnosis of type 1 diabetes for at least 1 year, who completed (or parent/guardian completed) an online questionnaire including information on timing of meal insulin administration and frequency of missed meal insulin doses. The majority of T1D Exchange participants were given the opportunity to complete this questionnaire. Demographic, socioeconomic, and diabetes management factors were obtained from the questionnaire. The most recent hemoglobin A1c (HbA1c) measurement within 6 months prior to questionnaire completion was obtained from the clinic medical record. HbA1c values were measured by point-of-care device or local laboratory. Participants or parents (henceforth referred to as participants) reported on method of insulin delivery (multiple daily injections or use of insulin pump) and occurrences of diabetic ketoacidosis (DKA) and severe hypoglycemia (SH) during the 3 months prior to questionnaire completion. DKA was defined by occurrence of ketoacidosis diagnosed by a doctor requiring a visit to hospital, emergency room, or other health care facility. SH was defined as severe hypoglycemia resulting in seizure or loss of consciousness.
Timing of Meal Insulin Administration and Frequency of Missed Meal Insulin Doses
Multiple choice responses regarding timing of meal insulin administration included several minutes before, immediately before, during, and after meal, in addition to an “I do not give a mealtime bolus” option. Separate analyses were performed categorizing timing of meal insulin as before (several minutes or immediately before) versus not before (during or after) a meal. Multiple choice responses for frequency of missed meal insulin doses included never, less than once a month, less than once a week, 1 to 2 days a week, 3 to 4 days a week, 5 or 6 days a week, and at least once a day. Responses were grouped into missing at least one meal insulin dose per week versus rarely missing a meal insulin dose (never, less than once a month, less than once a week) for the analyses. Participants/parents needed to provide responses to both timing of meal insulin administration and frequency of missed meal insulin doses to be included in the cohort. Those who reported not administering a meal insulin dose were excluded from the cohort.
Statistical Analyses
Timing of meal insulin administration was tabulated overall and according to demographic and clinical characteristics. The relationship between timing of meal insulin and categorical characteristics was assessed using a chi-square test, t-test, or Kruskal-Wallis test as appropriate. Linear regression was used to assess the relationship between timing of meal insulin and HbA1c, and logistic regression was used to assess the relationship between timing of meal insulin and occurrence of at least one SH event and DKA event. These models were adjusted for age, duration of diabetes, sex, race/ethnicity, and annual household income.
Similar analyses were conducted for assessing the relationship between frequency of missed meal insulin doses with participant characteristics and glycemic outcomes. Logistic regression was used to assess the effect of timing of meal insulin on missing at least one meal insulin dose per week to determine whether postmeal insulin dosing was associated with missed meal insulin after adjusting for potential confounders including age, diabetes duration, sex, race/ethnicity, and annual household income. This analysis was further stratified by frequency of self-monitoring of blood glucose (SMBG) (<4 times per day vs ≥4 times per day) (excluding continuous glucose monitor [CGM] users) to determine whether this relationship differs according to level of recommended diabetes management. All analyses were completed overall and stratified by age group (<6, 6-<13, 13-<18, 18-<26 years).
Data analyses were performed using SAS version 9.4 (2011 SAS Institute Inc, Cary, NC). All P values are two-sided, and due to multiple comparisons only P values <.01 were considered statistically significant.
Results
Among the 4768 adolescent and young adult participants, mean age was 13.6 ± 5.4 years (range 2-26 years) and mean duration of diabetes was 6.5 ± 4.6 years (range 1-25 years). Half of the cohort was female (50%) and the majority was non-Hispanic white (81%). Mean HbA1c was 8.6% ± 1.5% (70 ± 16.4 mmol/mol). Fewer than one-fourth (21%) identified themselves as current CGM users and more than half (62%) were using insulin pumps. Additional cohort characteristics are shown in Supplemental Table 1. The current sample was representative of the T1D Exchange Registry in regard to demographic and clinical variables.
Timing of Meal Insulin Administration
Of the cohort, 21% reported administering insulin several minutes before the meal, 44% immediately before meal, 10% during meal, and 24% after the meal (Figure 1). The average proportion of participants reporting giving insulin prior to meals at each clinical center with at least 50 participants ranged from 31% to 89% (Figure 2). Premeal dosing was reported by more than 70% of participants in only 12 of these 31 centers, highlighting differences in how participants report giving meal insulin in diabetes centers throughout the country. Of note, individual T1D Exchange centers were not asked how they teach patients to administer meal insulin. Different centers may have different teaching practices regarding timing of meal insulin.
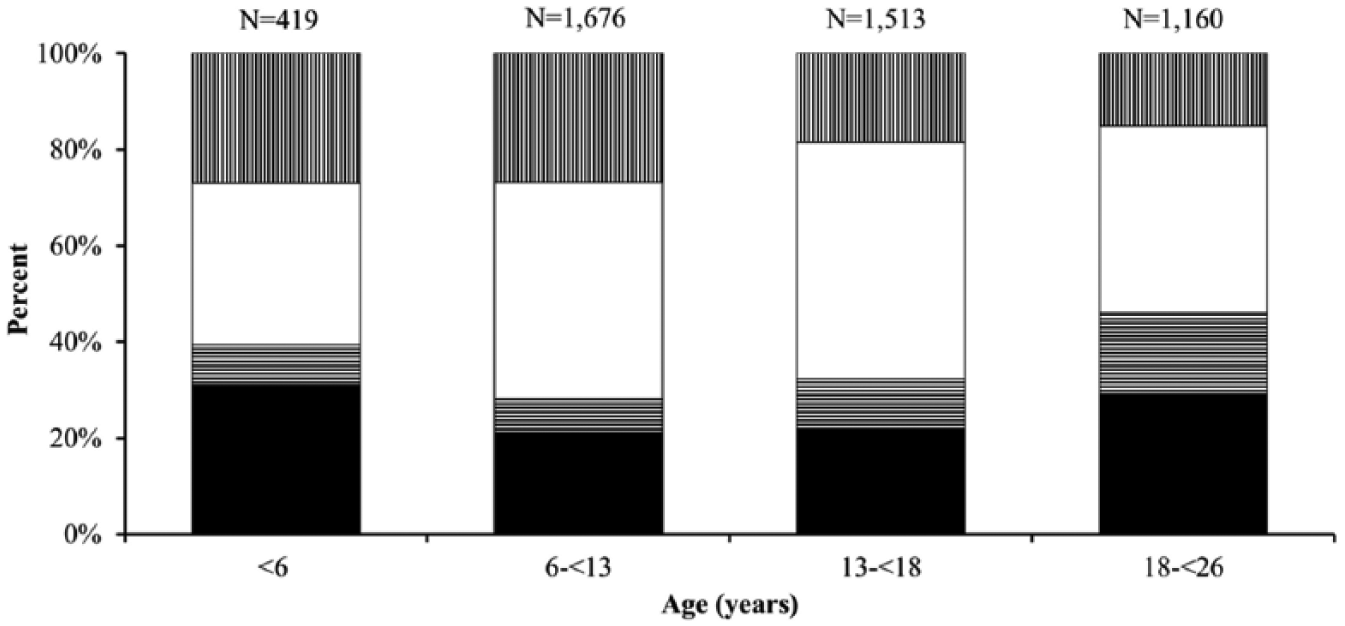
Distribution of timing of meal insulin within age group. Solid black represents after meal. Horizontal striped lines represent during meal. Solid white represents immediately before meal. Vertical striped lines represent several minutes before meal.
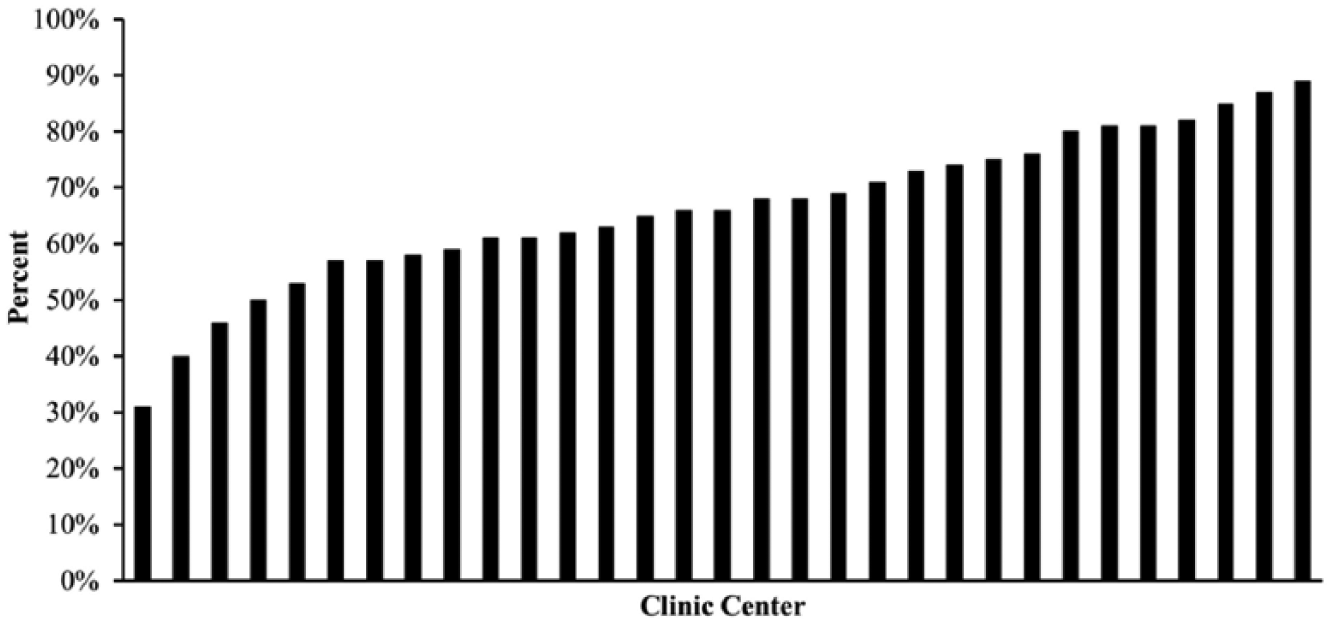
Premeal insulin administration across T1DX clinic centers. Premeal insulin administration defined as several minutes before meal and immediately before meal. Includes sites with ≥50 participants only.
Giving insulin before a meal (either several minutes or immediately before) was reported by 61% of participants/parents <6 years of age, 72% of those 6-<13 years, 68% of those 13-<18 years, and 54% of those 18-<26 years. Analysis of demographic and clinical differences between those who administered insulin before a meal (n = 3110, 65%) and those who administered insulin during or after a meal (n = 1658, 35%) indicated that those who gave meal insulin prior to a meal were younger (13.3 ± 5.3 years vs 14.0 ± 5.5 years, P < .001) were more likely to be of a minority race (21% vs 15%, P < .001), had shorter T1D duration (6.0 ± 4.2 years vs 7.5 ± 5.0 years, P < .001), were more likely to use pump therapy (63% vs 59%, P = .01) and CGM (24% vs 16%, P < .001), and monitored their blood glucose more frequently (6.2 ± 2.6 vs 5.4 ± 2.5 times per day, P < .001; Table 1). Results were similar when stratified by age.
Timing of Meal Insulin According to Participant Characteristics.
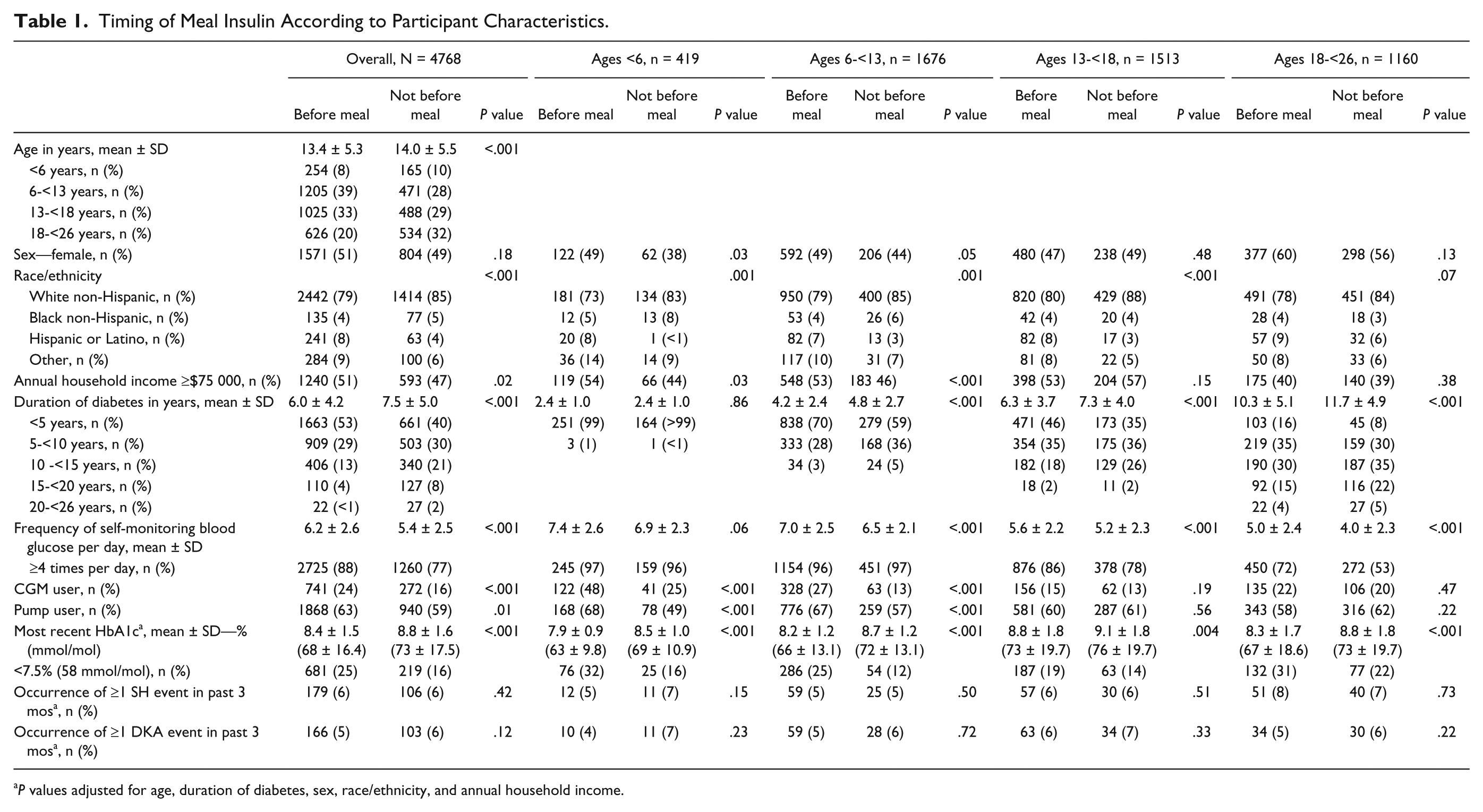
P values adjusted for age, duration of diabetes, sex, race/ethnicity, and annual household income.
HbA1c was significantly lower in those who reported insulin administration prior to a meal compared with those who reported insulin administration during or after meal (8.4% ± 1.5% [68 ± 16.4 mmol/mol] vs 8.8% ± 1.6% [73 ± 17.5 mmol/mol], P < .001; Table 1), though neither group achieves a mean HbA1c within the ADA guidelines. This relationship remained significant after adjustment for age, duration of diabetes, sex, race/ethnicity, and income (adjusted P < .001), and was observed across all age groups. A significant association was not observed between timing of meal insulin and occurrence of at least one SH event (6% of those who administer insulin before meal vs 6% during or after meal, P = .38) and DKA event (5% vs 6%, P = .21) in the past three months, even after adjusting for possible confounders (adjusted P = .42 and P = .12 for occurrence of ≥1 SH and DKA event, respectively; Table 1).
Frequency of Missed Meal Insulin Doses
The majority of participants (n = 3883, 81%) reported never or rarely missing a meal insulin dose (40% never, 26% less than once a month, 15% less than once a week). Among the 885 participants (19%) who missed a meal insulin dose at least once per week, 64% reported missing a meal insulin dose 1 to 2 days per week, 20% reported 3 to 4 days per week, 4% reported 5 to 6 days per week, and 12% reported at least once per day. The proportion of participants who reported missing at least one meal insulin dose per week was highest in adolescent and young adults (24% for 13-<18 years, 32% for 18-<26 years) compared with younger participants (5% for <6 years, 8% for 6-<13 years) (P < .001).
Participants who missed at least one meal insulin dose per week compared with those who rarely missed a meal insulin dose were older (14.5 ± 5.8 years vs 13.4 ± 5.3 years, P < .001), belonged to households earning less than $75 000 annually (58% vs 49%, P < .001), and had longer T1D duration (8.8 ± 5.0 years vs 6.0 ± 4.3 years, P < .001). Participants who rarely missed a meal insulin dose self-monitored blood glucose more intensively (6.2 ± 2.5 vs 4.4 ± 2.3 times per day, P < .001; Supplemental Table 2). Results were similar when stratified by age.
Though HbA1c was above ADA target for both groups, those who reported missing at least one meal insulin dose per week had worse glycemic control than those who rarely missed a meal insulin dose (HbA1c 9.8% ± 1.9% [84 ± 20.8 mmol/mol] vs 8.3% ± 1.3% [67 ± 14.2 mmol/mol], P < .001), even after adjusting for possible confounders (adjusted P < .001) (Supplemental Table 2). They also were more likely to experience at least one DKA event in the past 3 months than those who rarely missed a meal insulin dose (9% vs 5%, P < .001). This relationship between missed meal insulin doses and DKA remained significant after adjustment for confounders (adjusted P = .001), but only remained significant for the 13-<18 year group when analyses were stratified by age (adjusted P = .003). No significant relationship was seen between reporting missing at least one meal insulin dose per week and occurrence of at least one SH event (6% of those who miss ≥1 meal insulin dose vs 6% of those who rarely miss meal insulin dose, adjusted P = .9) (Supplemental Table 2).
Timing of Meal Insulin and Frequency of Missing Meal Insulin Doses
Participants who reported administering insulin during or after a meal were more likely to report missing at least one meal insulin dose per week compared with those who administered insulin before a meal (28% vs 14%, P < .001), even after adjusting for age, duration of diabetes, sex, race/ethnicity, and income (adjusted P < .001 and OR [99% CI] 2.10 [1.64, 2.60]). This relationship existed across all age groups, except among participants younger than 6 years (Figure 3). Missing at least one meal insulin dose per week was most common among those who reported administering insulin during a meal (31%), followed by those that administer insulin after (26%), immediately before (15%), and several minutes before meal (11%). Among participants who self-monitored their blood glucose <4 times per day (excluding CGM users), a trend was seen toward more missed meal insulin doses among those who administered insulin during or after meal compared to those administering insulin before meal (54% during or after meal vs 41% before meal, adjusted P = .01 and OR [99% CI] 1.72 [0.98, 3.02]). A similar relationship was observed among participants who self-monitor blood glucose ≥4 times per day, where those who administered insulin during or after meal were more likely to miss at least one meal insulin dose (19% during or after meal vs 11% before meal, adjusted P < .001 and OR [99% CI] 1.64 [1.20, 2.30]).
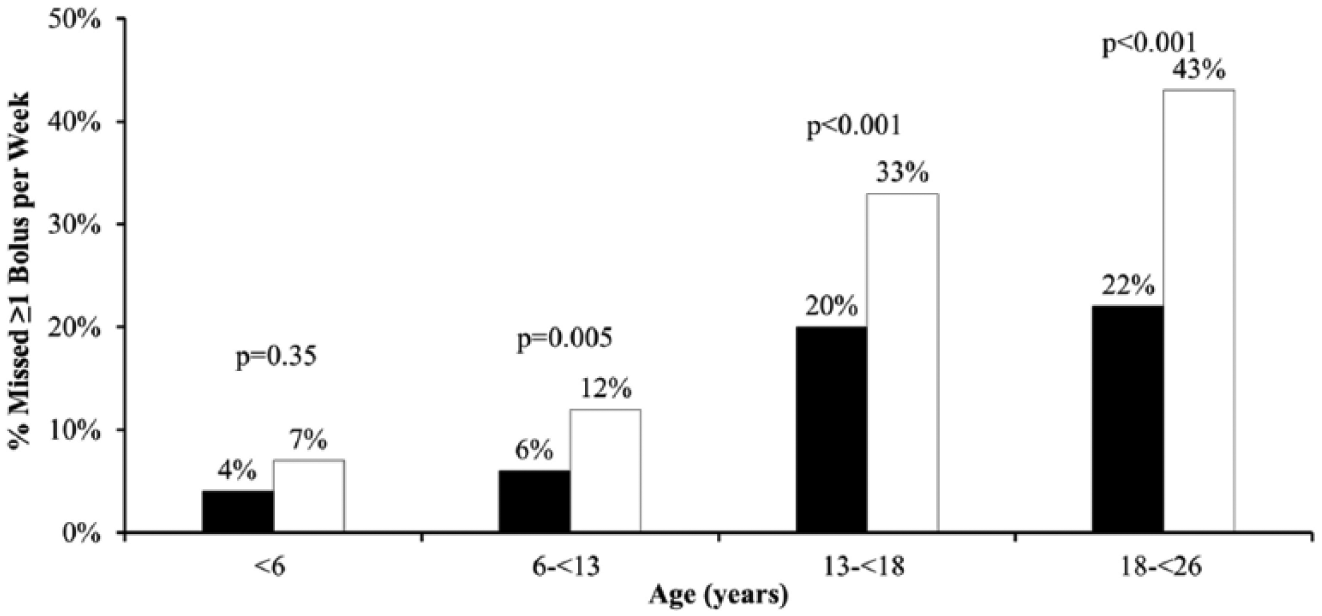
Timing of meal insulin and missing ≥1 meal insulin dose per week. Solid black bar represents before meal. Solid white bar represents during or after meal. P values adjusted for age, duration of diabetes, sex, race/ethnicity, and annual household income. Only 21 participants <6 years had parent report of missing ≥1 meal bolus per week; statistical tests were not performed for this group.
Discussion
Nearly 35% of youth participants in this cohort of the T1D Exchange clinic registry report not giving insulin before a meal. Premeal insulin administration is associated with decreased self-report of missed meal insulin doses (or increased adherence to meal insulin doses) and lower HbA1c. In addition, participants who missed at least one meal insulin dose per week had worse glycemic control, and were more likely to experience a DKA event. These findings are important not only because they demonstrate how patients give insulin, but also because they provide an opportunity for providers to assess and improve adherence to meal insulin therapy during routine office visits. Youth, particularly adolescents and young adults who are juggling school, work, and extracurricular activities, may be at higher risk of forgetting meal insulin. Therefore, emphasizing the importance of giving the meal insulin dose prior to eating may decrease forgotten meal doses, increase adherence to therapy, and improve glycemic control.
The T1D Exchange clinic registry has previously reported that participants with excellent glycemic control are more likely to report giving insulin before a meal.9,10 A logical question about this finding is whether participants’ adherence to therapy biased these results. Specifically, are participants who are adherent to therapy most likely to give insulin before a meal, and also most likely to have excellent glycemic control? To evaluate this question, we conducted a post hoc analysis to examine the relationship between the timing of the meal insulin dose and missed meal insulin doses in adherent and nonadherent patients with type 1 diabetes. A surrogate for adherence in type 1 diabetes is frequency of self-monitored blood glucose checks. 11 The ADA recommends that patients with type 1 diabetes check their blood sugar before meals/snacks, at bedtime, with concerns for low blood sugars, with exercise, and as needed at other times of day. This may necessitate blood glucose checks 6-10 times per day, but for the purposes of this paper, adherence to therapy was defined as checking blood sugars at least four times per day (ie, checking with meals, and at bedtime).1,11 While there are several metrics of adherence to therapy, parent/participant self-report of blood glucose checks was the only metric of adherence collected. Therefore, adherence was defined by self-report of checking blood sugars at least four times per day. Notably, an association between premeal insulin administration and fewer missed meal insulin doses was found in both adherent and nonadherent patients. This relationship suggests that, even among the most adherent patients, giving insulin before a meal could be associated with fewer missed meal insulin doses.
In pediatric patients in particular, a concern about giving insulin before a meal is the potential for hypoglycemia. Children may not reliably eat a meal or have the ability to detect and express hypoglycemia, making parents reluctant to give an insulin dose before a meal is consumed. However, T1D Exchange participants were asked to report episodes of SH, and no association between timing of meal insulin and reported hypoglycemia was found in any of the age groups examined. Previous studies that have examined timing of meal insulin have also not found a difference in hypoglycemia with respect to timing of insulin.5,6 While individual patient-specific decisions regarding timing of meal insulin should be left to the parents and provider, it is reassuring that the occurrence of a SH event was not associated with premeal insulin administration in this analysis.
While this study demonstrates an association between timing of the meal insulin and missed meal insulin doses, there are notable limitations. This analysis is cross-sectional, based on self-reported answers (from parents or participants) to an online questionnaire, and responders represented about 20% of the registry population as a whole, though the sample was representative of the registry population. It is also important to note that the majority of the current sample were non-Hispanic white and of relatively high socioeconomic status; thus, results may not generalize to other populations of children and young adults with T1D. The questions analyzed in this study were all multiple choice, with no option for additional questions or comments. For example, patients may opt to delay insulin injection if they are experiencing hypoglycemia before the meal, or if they have other problems affecting food absorption (for example, gastroparesis).
As this was a self-reported questionnaire, it is not possible to know how truthful participants were when they answered the questions. It is likely that all patients miss insulin doses periodically; however, it is unlikely that participants would overreport missed meal doses. It is more likely that missed doses may have been underreported, making the current findings particularly important. Another important limitation to note is the possibility that those who administer premeal insulin may differ from those who administer insulin during or after meal. Despite examining “adherent” and “nonadherent participants” and adjusting for potential confounders of age, duration of diabetes, sex, race/ethnicity, and income, other underlying factors may be influencing the association between premeal insulin administration and decreased likelihood of missed meal insulin doses. Furthermore, there may be some differences between parent-reported dosing and self-reported dosing (obtained from the older participants), which we were not able to capture in the current analysis. Finally, the relationship between premeal insulin administration and decreased self-report of missed meal insulin doses could not be properly concluded among participants aged <6 as only 21 participants had parent-report of missing at least one meal insulin dose per week.
This study has many practical implications for patients and their providers. Providers previously may not have been aware of how patients typically give meal insulin. Our data reveal that postmeal dosing is prevalent at all T1D Exchange clinical sites, even at sites that teach premeal blousing, and therefore should be a concern to all providers (Figure 2). Given that many of the T1D Exchange clinical sites are from academic medical centers with resources that may not be available at all practices, it is possible that the rates of premeal blousing are even lower in the general population. Our findings demonstrate an association between premeal insulin administration and improved adherence to therapy as reflected by fewer missed meal insulin doses. Furthermore, our analyses show that missing at least one meal insulin dose per week is associated with worse glycemic control and increased DKA events. Although this study is cross-sectional, it highlights several important findings that providers may discuss with their patients. While previous studies have shown that premeal insulin has pharmacokinetic benefits, our study also indicates an association between premeal insulin, fewer missed meal doses, and better glycemic control, offering further evidence for providers to emphasize the importance of premeal insulin to their patients.
Footnotes
Abbreviations
ADA, American Diabetes Association; CGM, continuous glucose monitor; DKA, diabetic ketoacidosis; SH, severe hypoglycemia; SMBG, self-monitoring of blood glucose; T1D Exchange, T1D Exchange clinic registry.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Leona M. and Harry B. Helmsley Charitable Trust.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.