
Abstract
To aid the burden of large dosing volumes, concentrated insulin products have been available in some form since the 1950s, albeit requiring significant and cumbersome detail in prescribing, converting doses from other products, and educating patients on how to administer. In 2015 and 2016, new concentrated products have been introduced that are available exclusively in pen devices that perform the conversion automatically, and thus, help to bypass the necessity for confusing calculations or administration. Providers and patients accustomed to traditional methods must recognize the differences and utility of these products to avoid dosing errors, as there are major differences in dosing procedures as well as their role in clinical practice. For example, the novel concentrated insulins (aside from U-500 products) are not solely indicated for severe insulin resistance. Use of novel agents may decrease the number of injections required, decrease complexity for patients and providers, reduce errors, and avoid conversion calculations. It is imperative that clinicians appreciate the nuances among the agents to choose an insulin product that is appropriate and fits a patient’s needs and preferences.
Keywords
Since the first patient was successfully treated with insulin in 1921, insulin products have been evolving. Developments over the past 3 to 4 decades have seen a transition from animal-derived insulin to synthetic human insulin, as well as the introduction of analog basal and rapid insulin products. Modern products continue to address and improve on concerns of their predecessors, such as the inconvenience or required dexterity when using a vial and syringe, excessive weight gain, risk of hypoglycemia, and the burdens of large dosing volumes. Insulin use is a mainstay in the management of patients with both type 1 and type 2 diabetes and is often an appropriate treatment option as either a first- or second-line agent, depending on the baseline A1c level or response to initial therapy.1,2 With the ever-growing prevalence of type 2 diabetes accompanied by obesity and significant insulin resistance, very high insulin doses are often needed and goals are often difficult to achieve. To aid the burden of large dosing volumes, concentrated insulin products have been available in some form since the 1950s.
Insulin is most commonly prescribed in the concentration of 100 units/mL (U-100). U-100 products include short-acting regular insulin, intermediate-acting neutral protamine Hagedorn (NPH), rapid-acting bolus insulin analogs lispro, aspart, and glulisine, and long-acting basal insulin analogs detemir, glargine U-100, and degludec U-100. Since it was approved in 1994, concentrated insulin has only been available in the form of regular insulin 500 units/mL vials (U-500 regular insulin) (Humulin R U-500; Lilly, Indianapolis, IN), which is 5 times as potent as its traditional regular U-100 counterpart at equal volumes. Patients are typically initiated on U-100 products, which are then titrated to therapeutic doses. Only when a severely insulin-resistant patient requires large doses in excess of 200 units/day is it appropriate to consider switching to U-500 regular concentrated insulin. 3 Converting from U-100 insulin to U-500 insulin, traditionally, has been very complicated and required confusing dose conversions. According to the manufacturer and based off of a study by Hood et al, a person with an A1c ≤8% should be started on a dose of U-500 insulin that is 80% of the final U-100 total daily dose; while those with an A1c >8% should be started on a dose equivalent to the final U-100 total daily dose.4,5 Once the U-100 insulin is discontinued, a U-500 regimen may be initiated in 2 daily doses divided 60% before breakfast and 40% before the evening meal, or in 3 daily doses divided 40% before breakfast, 30% before lunch, and 30% before the evening meal. Dose titrations are recommended for median 3-day premeal self-monitored blood glucose (SMBG) values and are similar for each dosing regimen. Dose adjustment recommendations should be applied to doses that affect the median SMBG values for particular points in the day. No change is recommended for SMBG 71-130 mg/dL. A 10% reduction is recommended for SMBG ≤ 70 mg/dL. The dose should be increased 5% for median SMBG values 131-180 mg/dL, by 10% for values 181-220 mg/dL, and by 15% for values > 220 mg/dL. Daily increases should not exceed 30% and daily decreases should not exceed 20%. Both regimens require similar dose titrations and both lead to significant and similar reductions in A1c. While the twice daily regimen has a higher rate of symptomatic hypoglycemia, severe hypoglycemia is very similar between regimens.4,5
While U-500 regular insulin has benefited many patients and has been used more frequently in recent years,6-8 it is not yet a commonplace agent, and many providers may not be familiar with the nuances of its use. Unfortunately, it has been the source of numerous dosing, prescribing, and dispensing errors. Until recently, it was only available in a vial and had to be administered with a U-100 insulin syringe or a tuberculin syringe, neither of which are designed for use with U-500 insulin. Clear communication is required to avoid dosing errors and prescriptions should read in actual units or volume rather than U-100 units. Every 1 unit of U-500 insulin is the same as 1 unit of U-100 insulin, but is delivered in one-fifth the volume. 9 For example, 5 units of U-500 insulin would be measured as 1 unit on a U-100 insulin syringe, but 0.01 mL volume in a tuberculin syringe; the communicated dose should be 5 units. 10 Unclear directions, communications, and product selections have contributed to dosing errors because of confusion over whether the intended dose is the number drawn to on a U-100 syringe, the volume injected, or the actual units injected, potentially resulting in an over/under dosing by 5 times. The “actual units” should always be communicated. In addition, the pharmacokinetics are different due to the increased concentration, 3 requiring nontraditional dosing frequencies and providing both mealtime and basal coverage. 6 Thus, U-500 regular insulin generally does not require a coadministered basal insulin.11,12 Use of U-500 insulin in addition to other insulin products should be cautioned. Despite these complexities, U-500 regular insulin demonstrated that it can provide the same or better glucose control compared to U-100 insulin while reducing the injected volume as well as the number of daily injections and this is appealing to patients and clinicians. 13 In 2015 and 2016, new concentrated products have been introduced that are available exclusively in pen devices that perform the conversion automatically, and thus, help to bypass the necessity for confusing calculations. Providers and patients accustomed to traditional methods must recognize the differences and utility of these products to avoid dosing errors, as there are major differences in dosing procedures as well as their role in clinical practice.
New U-500 Products
Two new products of 2016 have been specifically created to address the dosing issues of U-500 regular insulin. In July, the US Food and Drug Administration (FDA) approved a newly designed syringe purposed for use with U-500 regular insulin to directly measure proper doses without the need for a conversion. It is intended to be coprescribed with U-500 insulin vials and will be available by prescription only. The FDA reports that the Humulin R U-500 label will be updated to remove dose conversion tables for use with U-100 and tuberculin syringes since there will no longer be a need for them. The FDA advises that this new U-500 syringe should only be used with the U-500 insulin vial; that patients should not switch between types of syringes, because of the risk of dosing errors; and for patients to keep an adequate supply of U-500 syringes. 14
Earlier in the year, U-500 regular insulin became available as a prefilled pen device, the Humulin R U-500 KwikPen (Lilly, Indianapolis, IN), as an option to the vial. The new pen device requires no dosing calculations when converting from the U-500 vial. Patients need only dial to the prescribed number of units and administer the dose. Someone using 100 units of U-500 insulin will dial to 100 units on the new device. This would have been measured as 20 units (100 ÷ 5) on a U-100 insulin syringe or as 0.2 mL (100 ÷ 500) on a tuberculin syringe; but all along, this should have been communicated as a 100 unit dose. 15 Thus, it is important that patients understand their dose in actual units and not volume or U-100 equivalents, which is a change from methods many have used in the past. This 1:1 direct dose conversion from vial to pen should reduce the risk of over- or under-dosing compared to traditional dosing methods. Of note, the pen dials in increments of 5 units, instead of 1 unit like most U-100 pen devices, so dosing will, therefore, also be done in 5 unit increments. It can deliver up to 300 units of insulin per single injection, thus reducing the number of injections needed for some patients. The device holds 1500 units of insulin per pen, which is 5 times the number of units per pen of its U-100 counterparts, but in the same 3 mL volume. It delivers only 1/5 the volume of an equal dose from a U-100 device. In addition, it is a unique aqua color to prevent confusion with other insulin devices upon administration. 15
It is very important that patients and health care professionals alike have a thorough and accurate understanding of how to correctly use this insulin pen. Over dosage with an insulin pen can pose serious health risks, but this is especially true in the case of the U-500 regular insulin pen since it delivers 5 times the concentration of the standard U-100 insulin per volume.
Additional Novel Concentrated Insulin Products
In 2015, the first concentrated insulin products since U-500 regular insulin were introduced, but in differing concentrations and types of insulin. The new concentrated insulin products still provide large insulin doses in smaller volumes and availability in pen devices removes the need to convert doses when switching from traditional counterpart products. Furthermore, the novel concentrated insulins (aside from U-500 products) are not solely indicated for severe insulin resistance. A brief overview of the products is described in Table 1.
Product Information Regarding Concentration, Dosage Form Availability, and Conversion Ratios for Novel Concentrated Insulins.*
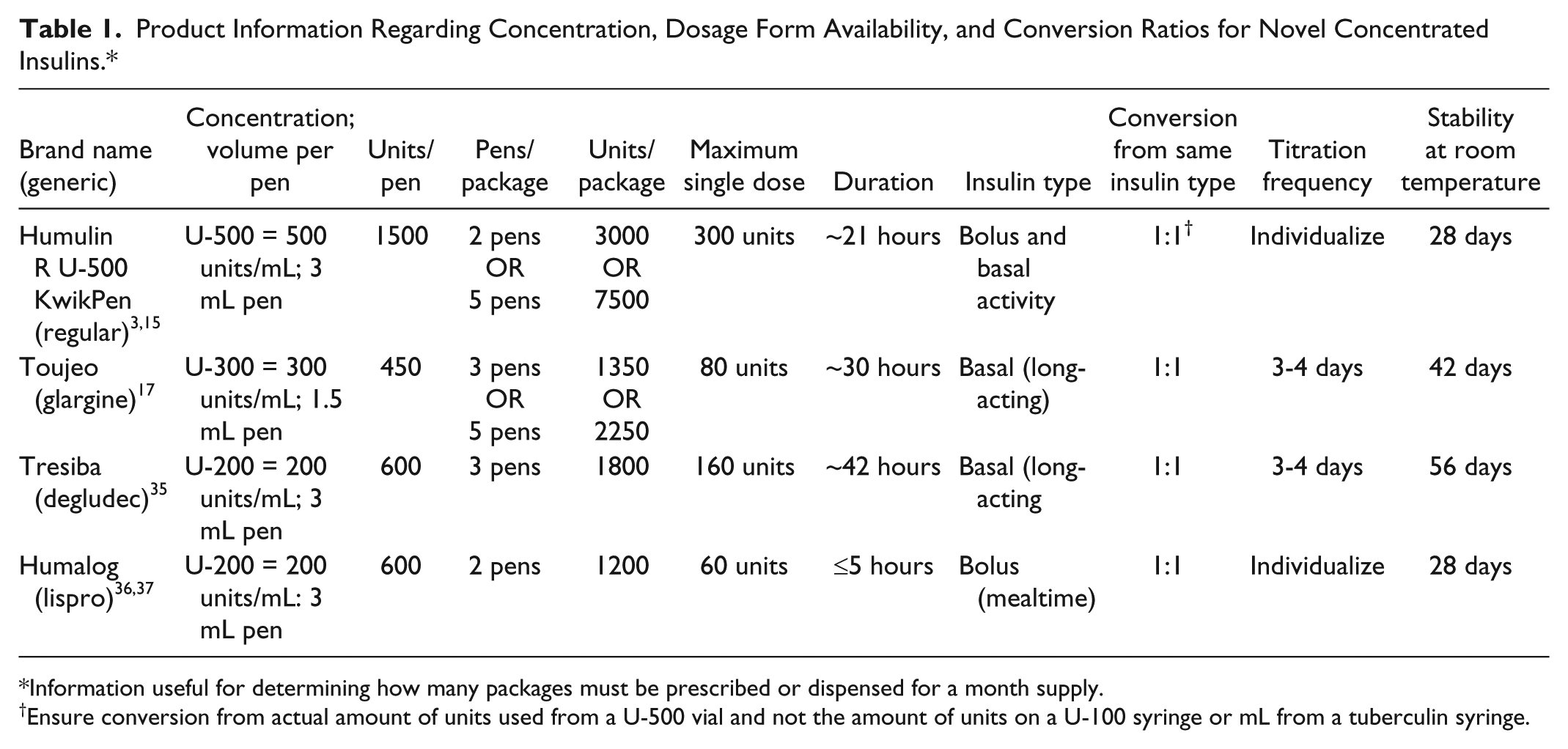
Information useful for determining how many packages must be prescribed or dispensed for a month supply.
Ensure conversion from actual amount of units used from a U-500 vial and not the amount of units on a U-100 syringe or mL from a tuberculin syringe.
Concentrated Basal Insulins
Insulin glargine 300 units/mL (U-300) (Toujeo; Sanofi-aventis LLC, Bridgewater, NJ) is a basal analog pen device that delivers insulin at one-third the volume of glargine U-100 (Lantus; Sanofi-aventis LLC, Bridgewater, NJ) in 1-unit increments. This removes the need to divide large-volume doses that are up to 80 units (pen delivers a maximum of 80 units/injection), and allows for once daily dosing of glargine U-300 for more patients than would have been possible with glargine U-100. The onset of action is slower (6 hours) compared to glargine U-100 (3-4 hours) and the duration of action is longer (average 30 hours) compared to glargine U-100 (24 hours).16,17 While not included in product labeling, the duration of glargine U-300 may allow for more flexibility in daily dosing times with intact safety and efficacy18,19 and may benefit more of those requiring twice-daily dosing of other basal insulins by simplifying to once daily dosing.18,20 Clinically, glargine U-300 is as efficacious for glycemic control as glargine U-100.18,21-30 Potential benefit lies with evidence supporting equal or less hypoglycemia and weight gain with glargine U-300 versus glargine U-100.18,21,25-27,29,31-34 The recommended starting dose for a patient with type 2 diabetes who is insulin naïve is 0.2 units/kg/day. Although a 1:1 conversion is recommended for switching to glargine U-300 from glargine U-100, detemir U-100 (Levemir; Novo Nordisk Inc, Plainsboro, NJ), or once-daily NPH, titration to higher doses may be needed for adequate glycemic control.6,17,18,21,23,34 Conversely, when switching from twice-daily NPH to once-daily glargine U-300, manufacturer labeling recommends starting glargine U-300 at 80% of the total daily dose of NPH, 17 just like the labeling for switching from twice-daily NPH to once-daily glargine U-100. In the same logic, when switching from glargine U-300 to gargine U-100, only 80% of the U-300 dose should be initiated. 16 Glargine U-300 should be titrated no more frequently than every 3 to 4 days. The glargine U-300 pen is stable at room temperature for 42 days after initial use compared to 28 days for the glargine U-100 insulin pen. 17
Insulin degludec (Tresiba; Novo Nordisk Inc, Plainsboro, NJ) is a new basal analog available as a pen device in both concentrations of degludec U-100 and degludec 200 units/mL (U-200). Both products are dosed once daily with a 42-hour duration of action. Similarly to glargine U-300, this may have a potential advantage for patients who do not consistently take their basal insulin at the same time every day by providing some efficacy beyond 24 hours. A delayed or missed dose may be made up later in the day as long as the next dose is at least 8 hours away. 35 The degludec U-200 product is targeted for those requiring larger doses of insulin. It can deliver up to 160 units in a single injection and is dosed in 2 unit increments. The U-100 product delivers a maximum of 80 units in a single dose and is dosed in 1 unit increments. There is no pharmacokinetic difference between degludec U-100 and U-200 preparations. The recommended starting dose in type 2 diabetes for someone who is insulin naïve is 10 units/day and should be titrated every 3-4 days. 35 When converting from other intermediate or long acting insulins, a 1:1 unit conversion is recommended. This approach is also utilized when converting between degludec U-100 and U-200. 35 Another potential advantage of degludec U-200 is the stability at room temperature for 8 weeks once opened, allowing for potential decreased waste of unused insulin in those who take relatively low doses.
Concentrated Bolus Insulin
The insulin lispro U-200 pen device (Humalog U-200 KwikPen; Lilly, Indianapolis, IN) is a rapid-acting insulin providing the advantage of having a single insulin pen last twice as long as the lispro U-100 pen device. This may benefit patients who require over 45 units per day of meal-time insulin, by requiring fewer pen changes per month, and therefore, less potential for running out of insulin from an individual device. 36 Doses are delivered in 1 unit increments up to a maximum of 60 units per dose. There is a 1:1 conversion from any rapid-acting insulin to either lispro U-100 or U-200 concentrations or between the 2 concentrations. There are no pharmacokinetic differences between the U-100 and U-200 preparations. 37 Insulin lispro U-200 should not be used in a subcutaneous infusion pump and it should not be mixed with other insulins (ie, NPH preparations). 37 Similar to the lispro U-100 pen, the U-200 pen is also stable at room temperature for 28 days after initial use.
Conclusion
These new products are practical additions to the arsenal against uncontrolled diabetes and give providers more options to better customize to individual patient needs. However, with more products to choose from, patients, providers, and pharmacists must be more cautious to avoid confusion between products. Providers need to be careful to select the properly intended product when e-prescribing through an electronic medical record. Many of these systems list all relevant products from an initial search for the desired drug. Concentrations may be listed at the end of the line and not always immediately visible without scrolling right. When a product is available in more than 1 concentration, but under the same brand name, it can be easy to select the incorrect product, sending a prescription with the wrong concentration to the pharmacy. Pharmacists must also be cautious to interpret concentrations properly on prescriptions and, then physically obtain the proper product from storage for dispensing. These products often have a very similar appearance and diligence is necessary to avoid a dispensing error. Patients as well as all health care providers must communicate product concentrations and doses very clearly to avoid errors. These interactions could include phone calls requesting refills, visits in person without the presence of the actual medication, or in any transition-of-care setting. And finally, conversion from the regular U-500 vial to the new U-500 pen will require very clear communication to determine the proper new dose. Providers and patients must confirm the actual number of units being used (not the number of units listed on the U-100 syringe or number of mL volume on a tuberculin syringe) to use a 1:1 conversion dose.
Switching to a concentrated insulin is now much simpler, as long as communication is clear between providers, patients, and pharmacists. Use of novel agents may decrease the number of injections required, decrease complexity for patients and providers, reduce errors, and avoid conversion calculations. It is imperative that clinicians appreciate the nuances among the agents to choose an insulin product that is appropriate and fits a patient’s needs and preferences.
Footnotes
Abbreviations
FDA, US Food and Drug Administration; NPH, Neutral Protamine Hagedorn; SMBG, self-monitored blood glucose; U-100, 100 units/mL; U-200, 200 units/mL; U-300, 300 units/mL; U-500, 500 units/mL.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.