
Abstract
Continuous glucose monitoring (CGM) systems provide people with diabetes with valuable real-time information on glucose trajectories and trends, thus offering opportunities for improving diabetes self-management. Ample evidence from clinical trials underscores CGM effectiveness for biomedical outcomes including HbA1C and hypoglycemia. However, interindividual variability in CGM uptake seems to be substantial: Neither do all individuals with diabetes adopt CGM readily in their diabetes self-management, nor do all of them benefit from CGM. In this article, we focus on CGM effects on quality of life and the potential role of psychosocial patient characteristics for determining the uptake and outcomes of CGM. After providing a brief overview on existing evidence on psychosocial factors in CGM use, gaps in existing research are identified and directions for future research are proposed that could answer key research questions and offer guidance for clinical diabetes care.
Keywords
The availability of patient systems for continuous glucose monitoring (CGM) has been a major technological innovation in the treatment of diabetes: Real-time CGM allows individuals with diabetes to track their glucose levels in real-time and to obtain information on glucose trends and trajectories, thus, offering new opportunities for people with diabetes for their diabetes self-management: Real-time CGM provides warning functions to signal imminent hypoglycemia or hyperglycemia. CGM technology may facilitate diabetes self-management by helping people with diabetes to adequately react to changes in glucose (trends) to achieve glycemic targets in a timely manner (lowering of HbA1c, less glucose fluctuations, less hypoglycemic events). Recent years saw rapid developments in CGM technology in terms of measurement accuracy, reliability and ease-of-use, rendering the systems more accessible for a broader range of people with diabetes. 1 Outside the field of diabetes care and research, CGM has also been gaining attention as a technological innovation, 2 for example in behavioral medicine research 3 , where glucose monitoring provides a new biosignal for the study of subclinical metabolic anomalies in conditions like depression or chronic stress. In addition to stand-alone CGM systems, integrated systems that combine insulin pumps for insulin delivery with CGM and allow for an automatic suspension of insulin delivery in case of impeding hypoglycemia, offer new therapeutic options and were shown to be effective in terms of avoiding or reducing nocturnal hypoglycemia.4,5
As a landmark clinical trial, the Juvenile Diabetes Research Foundation (JDRF) Study, which examined the effectiveness of CGM in children, adolescents, and adults in a prospective randomized trial, provided evidence for real-time CGM to lower HbA1C levels while avoiding an increase in hypoglycemia, which has been corroborated in several clinical trials by now, as was also shown in recent meta-analyses.6-9
With this article, we pursue two goals: First, existing CGM research in type 1 diabetes will be briefly summarized adopting the framework proposed by Hisore et al 10 , that stresses the relevance on predictors and outcomes in the psychosocial domain. Key domains of interest are the patient’s perceptions of (dis)advantages and barriers as predictors of CGM use and success, as well as quality of life as a patient-reported outcome (PRO). We will extend the perspective of this recent review article, that summarized research in children and adolescents, 10 and focus on research in adults with diabetes. Second, we will identify gaps in existing research in terms of psychosocial determinants and outcomes of CGM, outlining a research agenda designed to answer key research questions in the field.
CGM and Quality of Life
The US Food and Drug Administration’s (FDA) Guidance emphasizes the PROs 11 that are considered to be of comparable importance as biomedical outcomes when it comes to evaluating interventions in clinical trials. In diabetes research, PROs include generic (quality of life, anxiety, depression) as well as diabetes-specific domains (eg, fear of hypoglycemia, problems in self-management and care). Quality of life, in turn, is a multifaceted concept that—following a biopsychosocial model—covers the physical domain, well-being, and mental health as well as the social perspective (eg, social integration) and, hence, quality of life has to captured in a multidimensional fashion.
Previous clinical studies on CGM systems do not provide any a clear picture in terms of quality of life benefits of CGM (Table 1). While large-scale trials like the JDRF Study failed to consistently demonstrate quality of life effects of CGM, 12 several smaller-scale clinical studies provide mixed findings that may provide information on which domains of quality of life are afflicted by CGM: One study referred to positive effects of CGM use on the quality of life that was limited to the physical domain of quality of life only 13 , whereas other research even found a negative association of CGM with quality of life and psychosocial outcomes 14 or an increase in family conflicts of adolescents with diabetes who used CGM. 15 A current larger-scale survey in CGM users in the United States, however, revealed that over 80% of respondents believed that CGM facilitated their diabetes self-management, including benefits in terms of hypoglycemia avoidance and safety. 16
Quality of Life Effects of CGM.
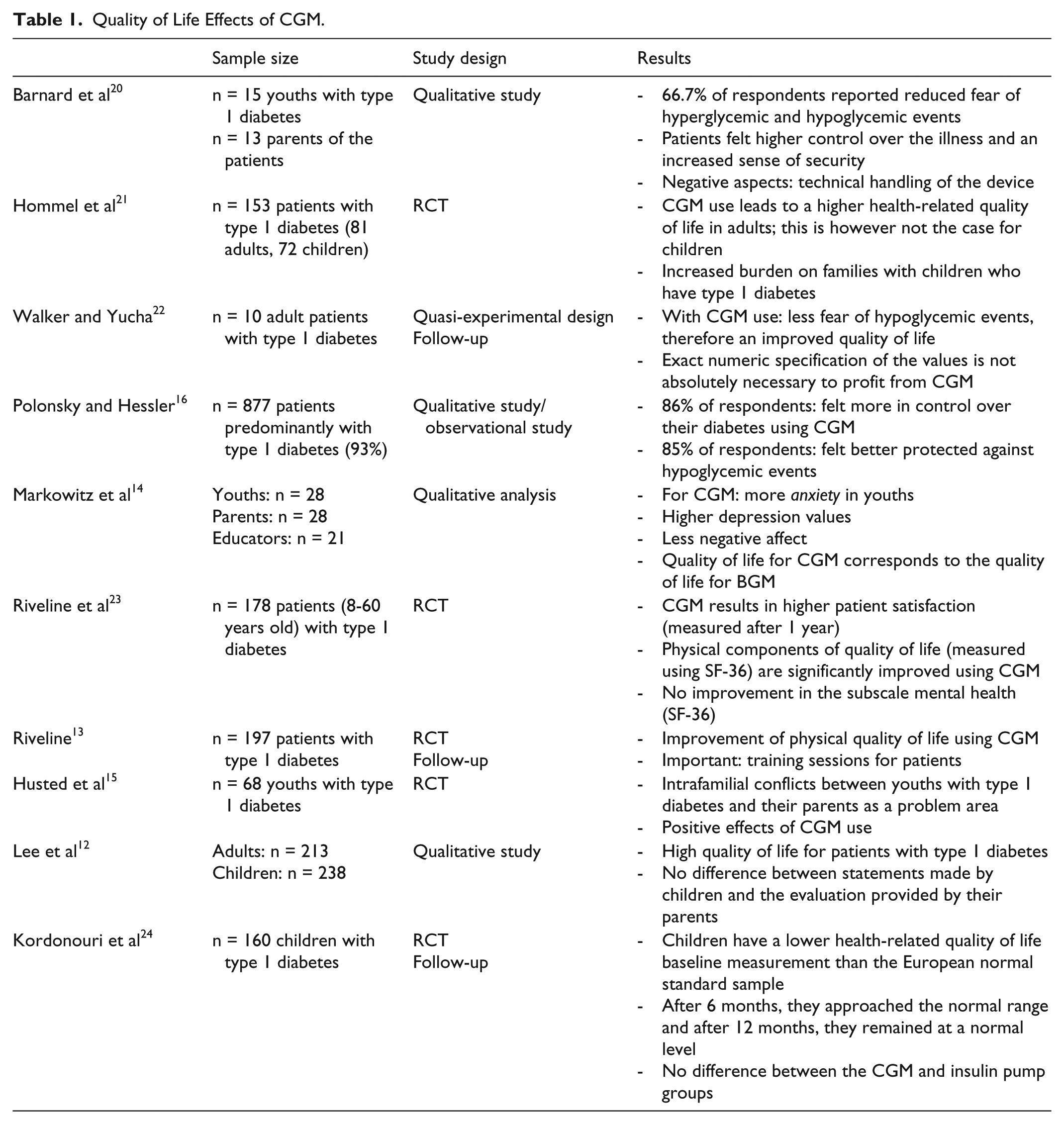
The heterogeneity of evidence on quality of life effects in clinical studies may partly be rooted in study methodology: With quality of life not being included as a primary outcome criterion, studies may be underpowered to demonstrate any effects in this domain. Moreover, quality of life effects may be obscured by the composition of study samples. This may lead to a skewed distribution of quality of life at baseline, possibly resulting in ceiling effects. Furthermore, sensitivity of change or lack thereof may be an issue as generic quality of life measures such as the SF 36 may fail to capture diabetes-specific effects such as an increase in perceived safety. Studies which capture quality of life in everyday life using change-sensitive procedures are missing (eg, ecological momentary assessment with electronic diaries). 17
Psychosocial Factors Influencing CGM Effectiveness
In terms of biomedical outcomes, CGM was found to be effective only when people with diabetes used CGM intensively, in a continuous manner and in a day-to-day fashion.8,9 Surprisingly, even in when study participants were supplied with CGM devices for free and without additional costs for the patients (like in the JDRF study), cross-participant variability of CGM uptake and use was substantial. CGM uptake, and hence effectiveness, varied across age groups, with adults benefitting the most and a mixed picture in children and adolescent. These differences are mediated by the amount of days the CGM system was used. Furthermore, in line with the notion of “past behavior predicts future behavior”, diabetes self-management behaviors prior to the initiation of CGM, such as frequency of blood glucose self-monitoring, was significantly predicting CGM uptake.
While the latter finding offers some insights in terms of determinants of CGM success, one key question remains unanswered: Why do some people with diabetes use their CGM continuously, while others do not? Human factors research shows that psychosocial variables are likely to play an important role when it comes to CGM uptake. In support of this notion, the previously mentioned survey in CGM users identified numerous human factor predictors of CGM uptake and effectiveness, including variables such as perceived system reliability and ease-of-use. Unfortunately, the existing evidence on psychosocial predictors of CGM uptake is scarce, as is dedicated research on this theme. Most evidence stems from smaller cross-sectional studies or is built on post hoc analyses of (sub)samples in large-scale trials (see Table 2 for an overview). One of the first studies builds on qualitative interviews in a subsample of the JDRF study 18 to identify psychosocial characteristics that distinguish between CGM users who benefitted from nonresponders. Three domains were identified that could hamper successful CGM use as perceived by the study participants:
- Frustration felt by the patient, primarily when expectations of CGM use are not met
- Feelings of being overwhelmed by the sheer amount of information provided by real-time CGM and the constant availability of glucose readings
- Negative reactions from the social environment, possibly resulting in a perceived need to justify oneself as to why a(nother) technical device is worn constantly on the body
Psychosocial Determinants of CGM Uptake.

In addition to patients’ perceptions rooted in the experience with CGM and social environmental factors, human factors research suggests that patients’ expectations prior to CGM use may influence uptake of the technology and its sustained use. 19 Unrealistic expectations may lead to disappointment and, eventually, discontinuation of CGM: These may include the unfounded belief that with CGM, conventional blood glucose measurements with finger pricks will not be mandatory anymore. General “tech savviness” can also play a role in the adoption of CGM technology. Finally, time and effort may be underestimated that need to be invested in building CGM-related skills that range from technical handling to integrating CGM-provided information into one’s diabetes self-management.
Summary and Prospects: The Need for a Psychosocial Research Agenda
In this article, we summarized evidence on psychosocial determinants and impact of CGM. Evidence on the effects of CGM on quality of life as a key psychosocial outcome is heterogeneous, which may be a result of larger-scale clinical trials focusing on metabolic outcomes as primary outcome criteria. This may in turn lead to insufficient statistical power to capture quality of life effects. We want to argue that—in line with the FDA guidance—future clinical trials should (1) emphasize quality of life outcomes to a similar extent as it is done with metabolic outcomes. In addition to power considerations, the (2) careful selection of measures is of paramount importance: Quality of life measures should cover both generic as well as a range of diabetes-specific instruments (including treatment/CGM satisfaction and fear of hypoglycemia), with particular attention being paid to sensitivity of change of these measures. Possible ceiling effects that may result from a skewed distribution of quality of life at baseline (ie, many study participants already reporting relatively high levels of quality of life) could be dealt with statistically in the data-analytical approach, and with careful considerations regarding sample composition and inclusion criteria (e.g., stratified sampling based on baseline quality of life).
In terms of predictors of CGM uptake, self-management behaviors determine the success of CGM to a large extent—particularly the regular and continuous use of the systems. While emerging evidence on psychosocial factors provides valuable insights in determinants and themes that may impact CGM uptake and use, more research is needed that should draw from human factors models and research: To ensure the integration of CGM into diabetes self-management in an optimal manner and to increase the outreach of the technology requires to connect to patients’ experiences and perceptions. A dedicated psychosocial research agenda is needed to generate more comprehensive evidence and to provide practitioners and patients with evidence-based guidance.
Footnotes
Acknowledgements
We would like to thank many of our colleagues for the discussions on this topic. This article is an expanded version of an article in German that has been previously published in the journal Diabetologie und Stoffwechsel 2015;10:29-35.
Abbreviations
CGM, continuous glucose monitoring; FDA, Food and Drug Administration; JDRF, Juvenile Diabetes Research Foundation; PRO, patient-reported outcome.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.