
Abstract
Background:
Technology provides adjuvant and/or alternative approaches to care and may promote self-care, communication, and engagement with health care services. Common recent technologies for diabetes include continuous subcutaneous insulin infusions (insulin pumps), continuous glucose monitoring systems, smartphone and tablet applications, and telehealth (video conferencing). This study reports Australian diabetes educators’ intentions and reported professional use of these technologies for people with type 1 diabetes, and factors predictive of this.
Methods:
An anonymous, web-based questionnaire based on the technology acceptance model was distributed to members of the Australian Diabetes Educators Association through their electronic newsletter. Exploratory factor analysis revealed a 5-factor solution comprising confidence and competence, improving clinical practice, preparation (intentions and training), ease of use, and subjective norms. Logistic regression analyses identified factors predicting intention and use of technology.
Results:
Respondents (n = 228) had high intentions to use technology. The majority reported using continuous subcutaneous insulin infusions, continuous glucose monitoring systems, and applications with patients, but usage was occasional. Confidence and competence independently predicted both intentions and use of all 4 technologies. Preparation (intentions and training) independently predicted use of each technology also.
Conclusions:
Discrepancies and dissonance appear between diabetes educators’ intentions and behavior (intentions to use and reported technology use). Intentions were higher than current use, which was relatively low and not likely to provide significant support to people with type 1 diabetes for disease management, communication, and engagement with health care services. Continuing education and experiential learning may be key in supporting diabetes educators to align their intentions with their practice.
Keywords
Globally, type 1 diabetes (T1D) incidence is increasing, which is challenging many health systems. Overall incidence is increasing by around 3% each year, 1 estimated in Australia at 11 cases per 100 000 population. 2 Numbers are rising particularly in the 0-14 years age group,3,4 a concern because onset at a young age means early potential health impact and consequent high disease burden.5-7
Decreasing the impact of T1D on health requires optimizing glycemic control, 8 which is not widely achieved. Better glycemic control is seen in young adults who maintain rather than lack regular contact with routine preventive care services. 9 However, many adult diabetes services are focused on older people with type 2 diabetes,10,11 and those with T1D may struggle to access disease or age specific care; many young adults become disengaged from diabetes services.12-14 This results in reduced diabetes self-management and well-being, and inadequate complication screening.6,7 Innovative health care approaches are needed for young people with T1D to support their disease management and maintain and improve communication and engagement with health care services.
Technology provides potential alternative and/or adjuvant opportunities. Current common diabetes technologies include continuous subcutaneous insulin infusion (CSII) therapy, continuous glucose monitoring (CGM) systems, applications, and video conferencing (VC). Compared to injections, CSII may achieve better clinical outcomes, including reduced mortality and improved quality of life, due to increased meal-time and carbohydrate flexibility and greater convenience and discretion of insulin delivery.15-19 Unsurprisingly, CSII use is increasing. In Australia, commencement rates have consistently increased by an average of 107 to 140 new users each month from 2004-2010. By 2011 around 10% of the T1D population were using this technology and one-third of users were aged under 20 years. 20 With glycemic control and insulin dosages reliant on blood glucose monitoring, this technology is often used in combination with CGM. More often used sporadically than continuously due to its cost, 21 CGM overcomes limitations of intermittent monitoring and has been associated with reduction in HbA1c without increased hypoglycemia risk.19,22
Specialized program applications (“apps”) downloaded on smart phones and tablets are used to transfer blood glucose measurements electronically to health care providers. 23 They also provide timely information on, for example, carbohydrate content of foods to support self-care,23-25 and with an estimated 74% of younger adults using smartphones, 26 this may achieve significant impact. VC is another form of internet based communication, allowing simultaneous audio and visual communication between 2 or more locations. Personal communication software such as Skype™ and FaceTime® can be used as well as commercial systems managed by health care organizations. VC can be used for continuing education as well as clinical care, and has been the means through which young people with T1D have reengaged with specialist diabetes services. 27
However, technology use requires specialist expertise. Diabetes educators (DEs), health care professionals from disciplines such as nursing and dietetics, are key to the treatment and support of people with T1D and ideally placed to promote and support appropriate technology use. Few studies have examined health care professionals’ use of diabetes-related technologies for patients with T1D. 28
This study aimed to determine DEs’ intended and reported professional use of common diabetes-related technologies for patients with T1D, and predictive factors.
The main theoretical framework underpinning the study was the technology acceptance model (TAM), an information systems theory that models how users come to accept and use a technology.29-33 Originally developed to examine responses to computer technology, the model has been revised for translation to the health care context and used to examine, first, telemedicine technology acceptance by physicians 34 and then evaluation of home telemonitoring for patients with heart failure and/or chronic obstructive pulmonary disease. 35 Factors were added from relevant theories, mapping influences on behavioral intention from individual, technological, and organizational contexts, structured as 7 theoretical constructs.
Methods
Design and data collection
A survey design was used, and data were collected with an anonymous, web-based questionnaire. The most recent TAM model used in health care included habit, facilitating conditions, and subjective norms and omitted peer influence and perceived technology control (ability or competence). 35 No rationale was supplied for these omissions, yet perceived technology control may be important as shortages of health care professional expertise have been cited as a reason why health care professionals do not engage with CSII-related care. This 33-item version of the questionnaire 35 had 4 questions on attitude (perceived positive or negative consequences of adopting the technology) and compatibility (the degree of correspondence between a new technology and existing values, past experiences and needs of potential adopters) in the individual context. Within the technological context, 6 questions sought perceived ease-of-use and usefulness, and 3 focused on habit (behavior that has become automatic). Within the organizational context 4 questions related to subjective norms (the extent to which an individual believes that people who are important to them will approve of their behavior adoption), and 3 to facilitating conditions (the degree to which individuals believe that organizational and technical infrastructures support usage). Three questions on intention were included. Responses were measured on a 7-point Likert-type scale from −3 = totally disagree to 3 = totally agree, with scores summed for each of the 8 factors. Validity was supported by a panel of experts in technology, and Cronbach’s alpha values greater than or equal to .7 were reported for all but 1 factor (habit = .56). This version of the model had never been formally tested.
Modifications to the questionnaire for this study included wording changes to relate to T1D, and removal of negative values from the Likert-type scale for more intuitive scaling (from 1 = strongly disagree to 7 = strongly agree). Seven questions were added: 1 question determined technology use and frequency measured on a 5-point Likert-type scale (1 = never, 2 = daily, 3 = weekly, 4 = monthly, and 5 = occasionally); 6 questions related to competence in provision of information and advice, data interpretation, operation, problem solving, and overall competence for these technologies (measured using the original scale of 1 = strongly disagree to 7 = strongly agree). Finally, an extra response choice of “already know,” “already use,” or “intend to continue” was added to 6 questions, to distinguish existing knowledge and technology usage. The questionnaire was formatted to ask participants to consider the 4 technologies separately, and data were collected to characterize participants’ age, sex, health care qualifications, and experience. The modified questionnaire was reviewed for face and content validity by 2 subject matter experts, both physicians with extensive research and diabetes experience, and piloted by 8 Canadian-based DEs; minor changes were made for ease of moving through the survey.
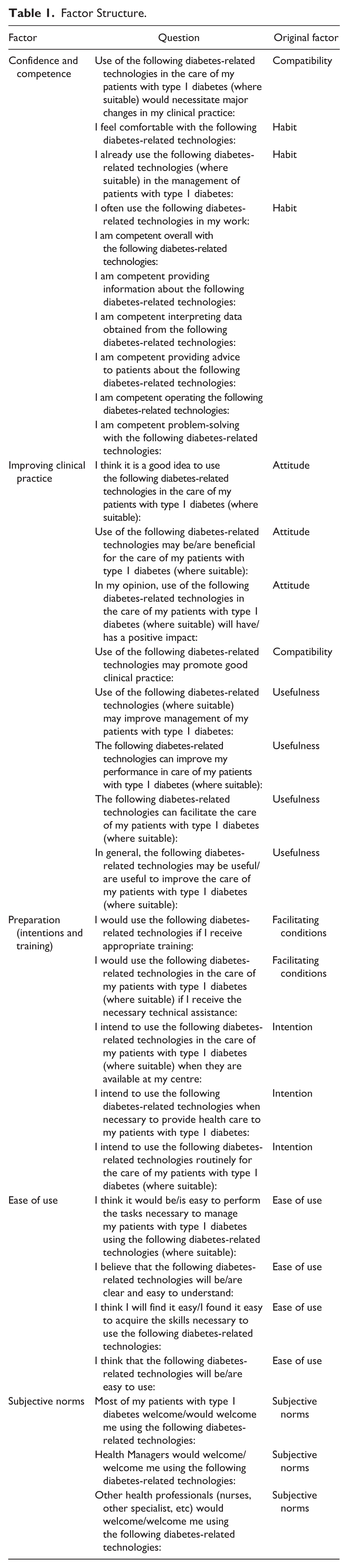
Exploratory factor analyses using an iterated principal axis analysis with promax rotation examined the factor structure for each of the 4 technologies separately. Discriminant validity was evaluated by inspecting the construct loadings of each factor, applying criteria of a primary factor loading of 0.4 or above and no cross-loading of 0.6 or more. 36 Initial factor analyses identified that 9 questions did not consistently load on identified factors for 3 or more of the technologies. Their exclusion resulted in a replicating 5-factor solution and improved fit across the 4 technologies. These 5 factors were confidence and competence, improving clinical practice, preparation (intentions and training), ease of use, and subjective norms. These factors explained 71.17% of the variance for the questions related to CSII, 70.13% for CGM, 71.09% for apps, and 67.95% for VC. The Kaiser-Meyer-Olkin measure of sampling adequacy was .934 or above; Bartlett’s tests of sphericity were significant (CSII: χ2 = 6798, P < .001; CGM: χ2 = 6485, P < .001; apps: χ2 = 6500, P < .001; and VC: χ2 = 5813, P < .001); the diagonals of the anti-image correlation matrix were all 0.860 or above; and, excluding 1 question relating to CSII, CGM, and apps, communalities were all 0.4 or above. Finally, Cronbach’s alpha values were acceptable for all factors for all technologies; for the confidence and competence factor, values ranged from .950 to .974; for improving clinical practice, from .914 to .935; and the other domains ranged from .756 to .927. Items pertaining to competence in the confidence and competence factor were highly correlated (CSII = .614-.953; CGM = .646-.944; apps = .662-.929; and VC = .481-.915); however, the explanatory power of the factor was not improved by removal of any combination of these items (Table 1).
Factor Structure.
Sample
A convenience sample was collected from members of the Australian Diabetes Educators Association (ADEA), the leading Australian organization for multidisciplinary health care professionals who provide diabetes education and care. This organization had 1747 members on June 30, 2013. 37 To be eligible, participants were required to have experience as a DE in Australia, current membership with the ADEA, and be registered to receive the ADEA’s electronic newsletter; numbers of eligible members were not known. Approval for the study was obtained from the University of Technology Sydney Human Research Ethics Committee.
Procedure
The web based survey was undertaken June-August 2014. Potential participants were advised of the study and could access it through a link in the ADEA weekly electronic newsletter, operational for 12 weeks to allow for response patterns previously experienced in this population. 38 Reminders were posted in the newsletter at 2, 4, 6, 8, and 10 weeks following the first advice of the survey. Through the use of the skip logic feature in SurveyMonkey®, respondents were only asked relevant questions based on their previous responses. A total of 247 questionnaires were partially or fully completed; 19 provided only demographic data and were omitted from data analyses.
Data analyses
Data were entered into SPSS© version 23 software. Area of employment was categorised, 39 and for each of the 4 technologies, responses for reported technology use were categorized (no/yes) and compared with socio-demographic data using the chi-square test, where theoretical or clinical reasons identified these characteristics as potential influences.40,41 Questions were otherwise analyzed as ordinal measures and summed for each of the 5 factors, and for the 3 questions relating to intentions; 2 questions required reverse coding. Frequencies and medians (25, 75 quartile) scores, where appropriate, were used descriptively.
Logistic regression analyses were undertaken to identify independent predictors of DEs’ intentions and reported use of the 4 technologies. Dependent variables were intention to use each technology summary scores dichotomized at median scores into low and high intention (due to nonnormal distribution), and reported use (no/yes). Potential predictor variables comprised summary scores of the 5 factors identified through the factor analyses (though the single-item factor preparation [intentions and training] was not considered for analyses as a potential predictor of technology intention) and sociodemographic data. The backward entry method was selected to create the most parsimonious model and adjusted odds ratios and 95% confidence intervals reported. All assumptions of the models were tested and met. A P value < .05 was considered significant.
Results
The majority of respondents (n = 228) were female nurses, although multiple disciplines were represented (Table 2). Respondents had many years of experience in both their professions and in diabetes education, and were well educated. Most were presently credentialed with the ADEA and had experience working with pediatric and/or young adult patients with T1D; of those with experience working with pediatric patients with T1D, almost all (n = 125, 99.2%) also had experience with young adults with T1D. Most (91.7%) were currently working in Australia and in cities, with all states and territories of Australia represented.
Respondent Characteristics.
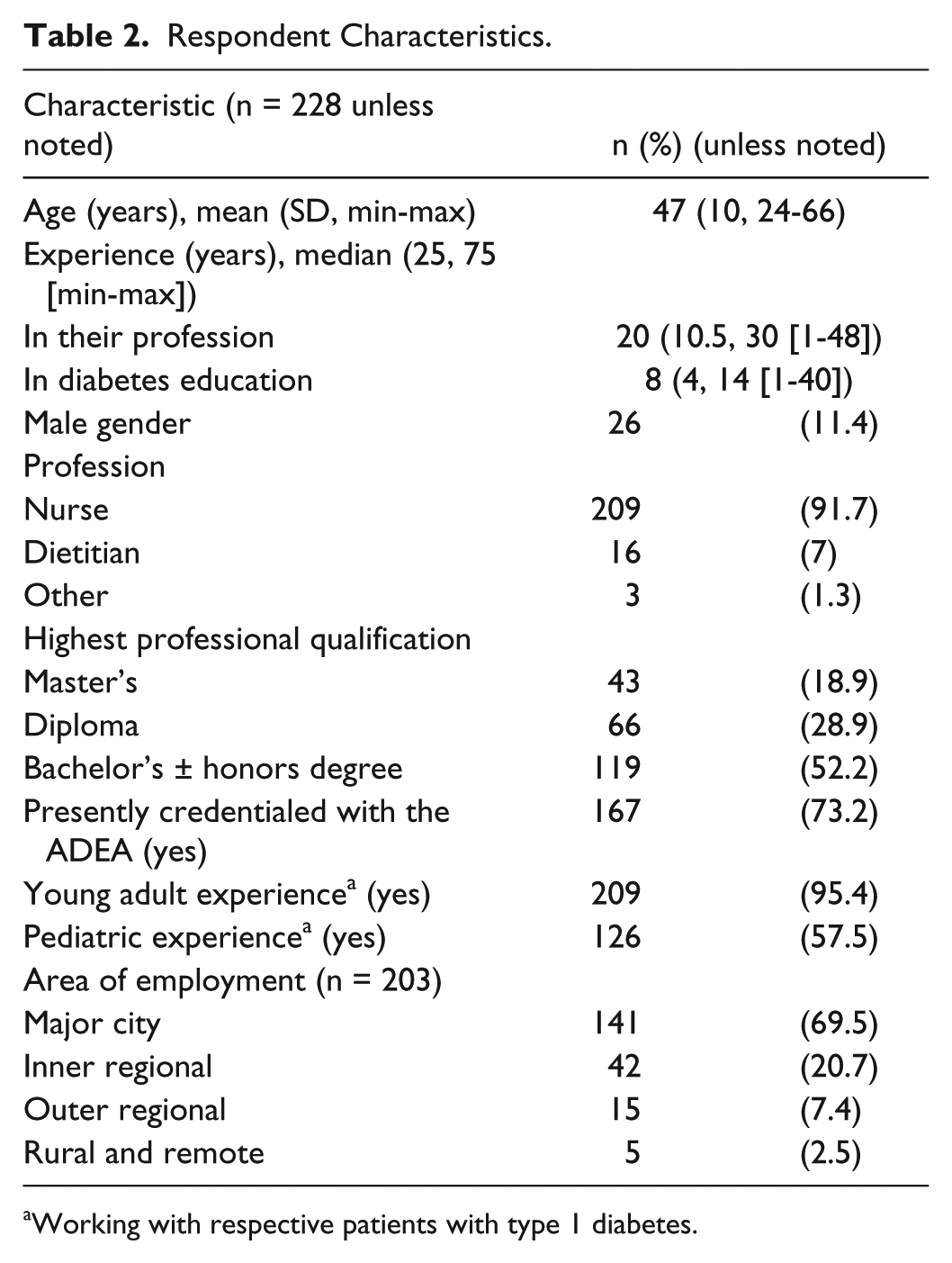
Working with respective patients with type 1 diabetes.
Summary scores of the 5 factors identified from the questionnaire as potentially influential for technology adoption were relatively consistent across the 4 technologies (Figure 1). Highest scores indicated that respondents strongly perceived positive consequences for patient care of adopting the 4 technologies; the lowest scores were for respondents’ reported confidence and competence. With maximum possible scores of 7 (1 = strongly disagree to 7 = strongly agree), overall respondents reported they felt competent with CSII (median [25, 75 quartile] score 6 [3, 7]), and somewhat competent with CGM (5 [3, 7]) and apps (5 [3, 6]). However, they neither agreed nor disagreed they were competent with VC (4 [2, 5]). They reported at least some degree of competence with each facet identified (Figure 2).
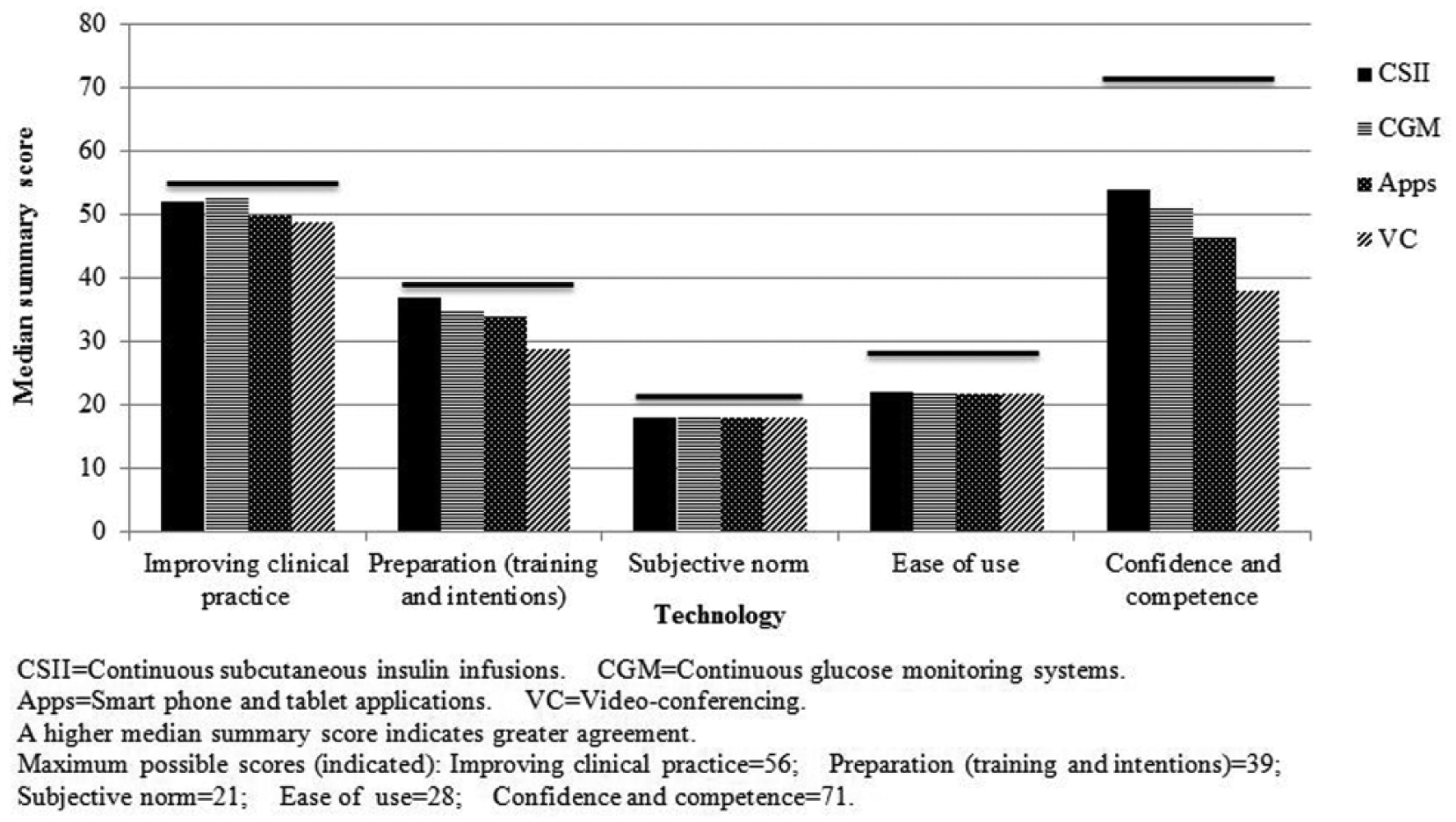
Factors Influencing Diabetes Educators’ Reported Use of Common Diabetes-Related Technologies for Patients with Type 1 Diabetes.
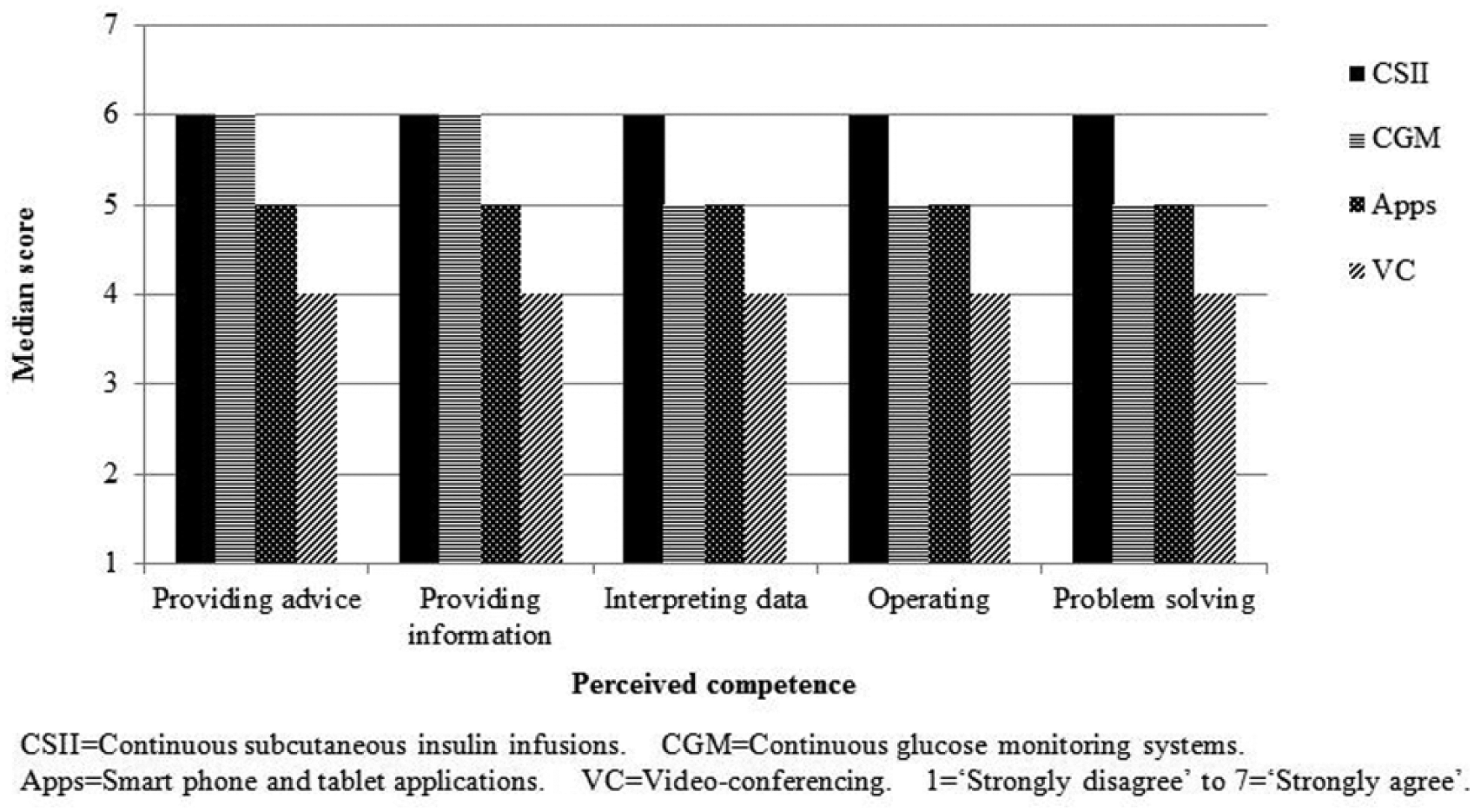
Diabetes Educators’ Reported Competence in Use of Common Diabetes-Related Technologies for Patients with Type 1 Diabetes.
Respondents had strongly positive intentions to use common diabetes-related technologies for patients with T1D, particularly CSII and CGM; somewhat less so for apps and VC (Figure 3). The majority of respondents also reported using CSII, CGM and apps for patients with T1D. Around 4 of every 5 respondents reported using CSII (80.3%), around 2 in 3 used CGM (65.4%) or apps (69.7%), but only around 1 in 3 used VC (36.4%). Significantly greater proportions of those with, rather than lacking, experience working with pediatric patients with T1D reported using CGM, apps, or VC. A greater proportion of DEs employed outside of major cities reported using VC. Overall, where these technologies were used; this was on an “occasional” basis.
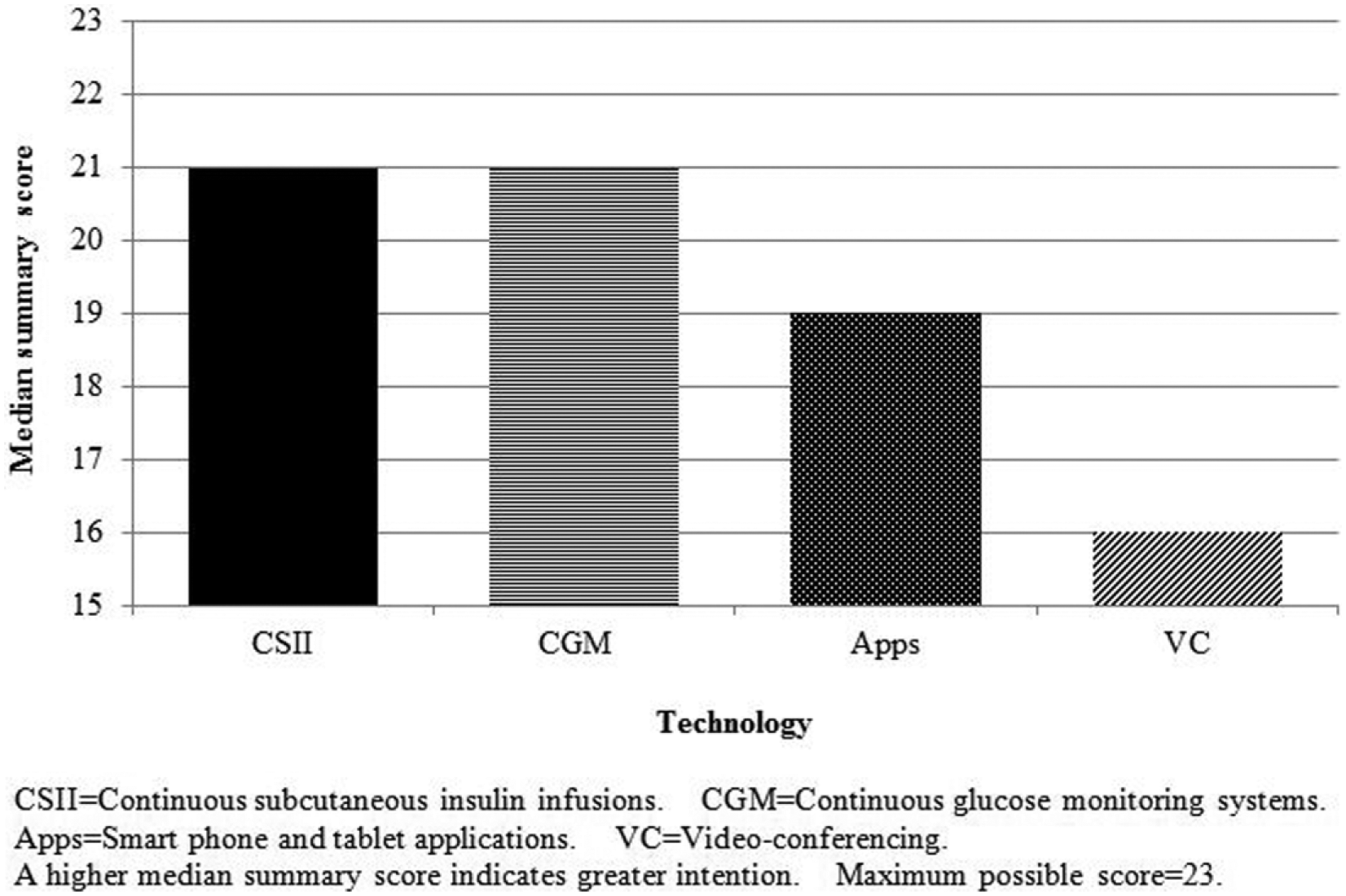
Diabetes Educators’ Intentions to Use of Common Diabetes-Related Technologies for Patients with Type 1 Diabetes.
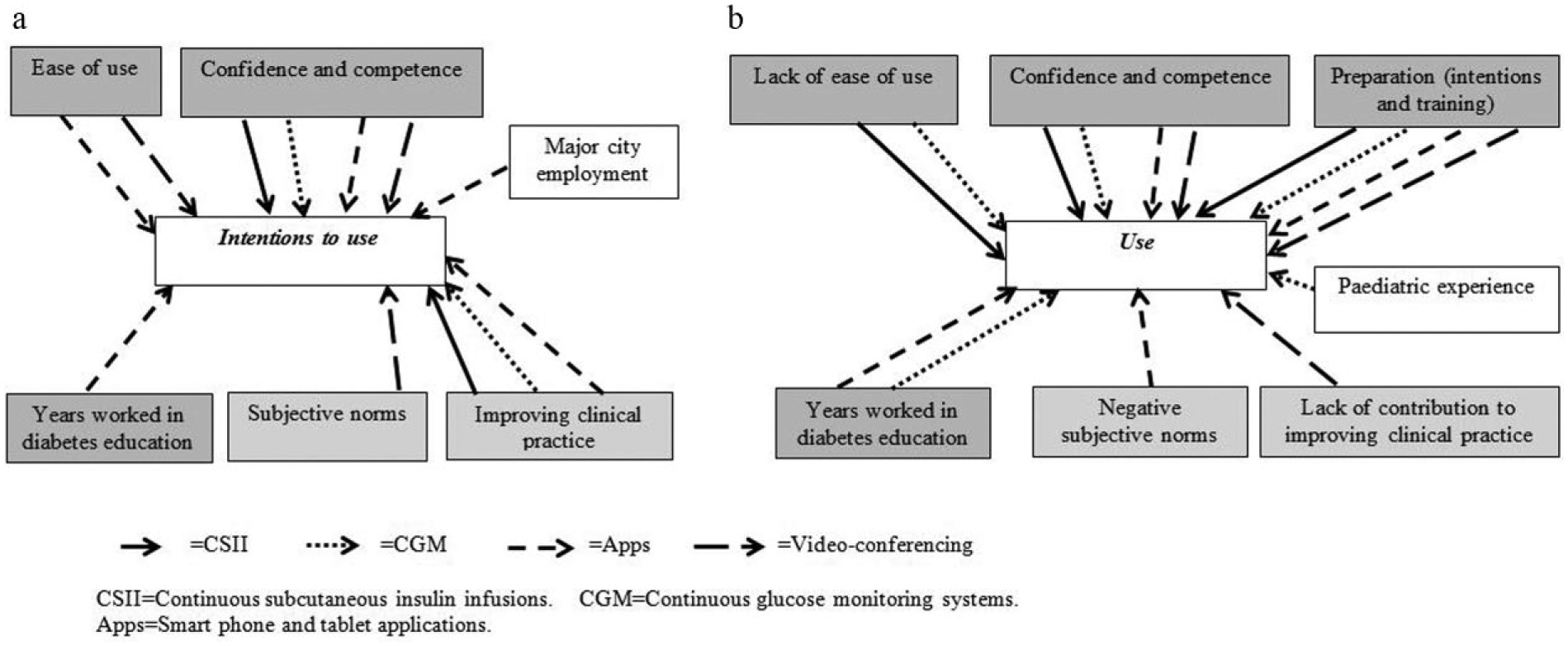
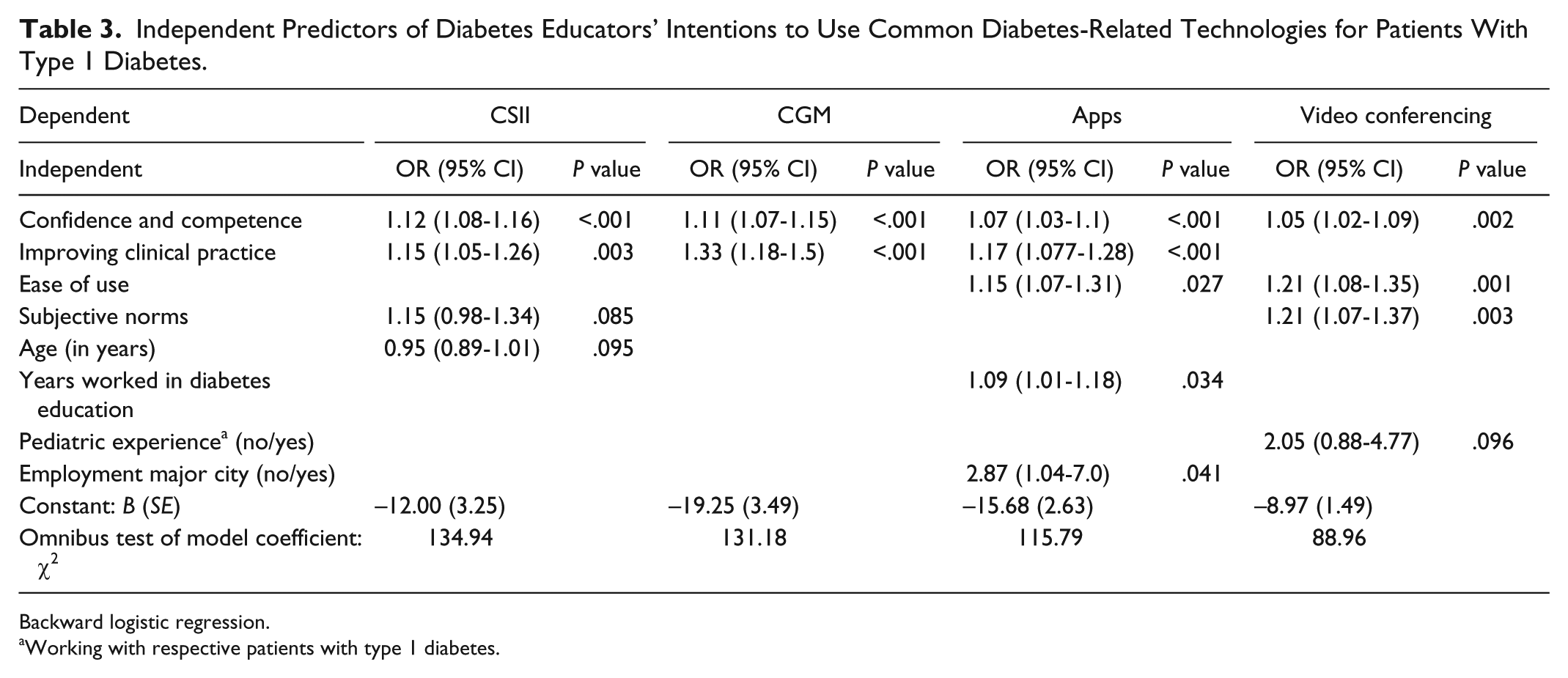
Many predictors of both intended and reported actual use of common diabetes-related technologies exhibited substantial effects across the technologies. Confidence and competence consistently positively predicted DEs’ intentions to use each of the 4 technologies; ease of use was also predictive of intention to use apps and VC; years worked in diabetes education positively predicted intention to use apps (Figure 4a; Table 3). Subjective norms were also important, positively predicting DEs’ intentions to use VC; perceived improvement to clinical practice consistently and positively predicted DEs’ intention to use all technology except VC. Employment in a major city was predictive of DEs’ intentions to use apps.
Common Diabetes-Related Technologies-Influences on Diabetes Educators’ Intentions and Reported Use.
Independent Predictors of Diabetes Educators’ Intentions to Use Common Diabetes-Related Technologies for Patients With Type 1 Diabetes.
Backward logistic regression.
Working with respective patients with type 1 diabetes.
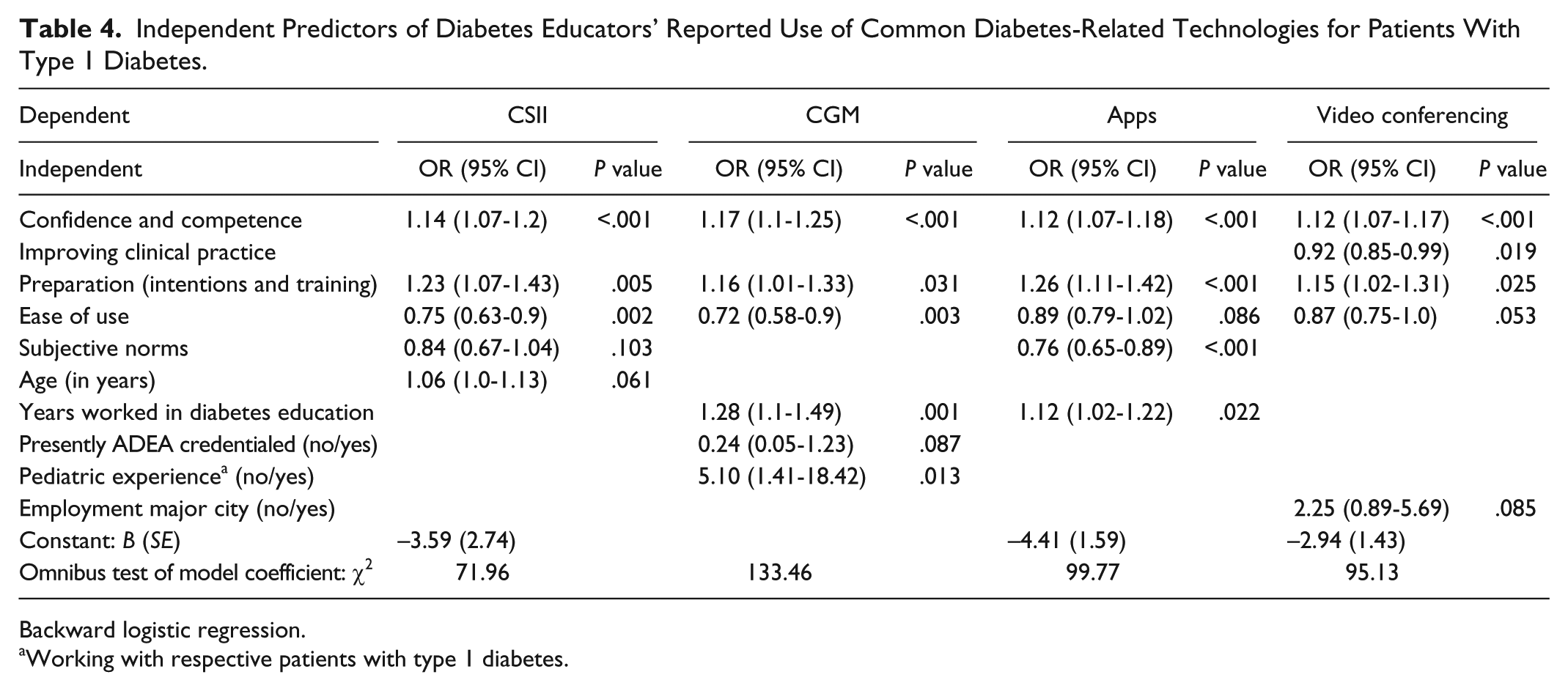
Predictive factors were shown to relate both positively and negatively to reported technology use (Figure 4b; Table 4). As for intention to use, DEs’ confidence and competence consistently positively predicted actual usage of all 4 technologies, as did preparation (intentions and training). Years worked in diabetes education positively predicted DEs’ reported use of both CGM and apps; experience working with pediatric patients with T1D positively predicted CGM use. However, lack of ease of use was a negative predictor, or deterrent, of CSII and CGM usage. Subjective norms were again of importance, negatively predictive of use of apps, with perceived negative effects for clinical practice linked to lower use of VC.
Independent Predictors of Diabetes Educators’ Reported Use of Common Diabetes-Related Technologies for Patients With Type 1 Diabetes.
Backward logistic regression.
Working with respective patients with type 1 diabetes.
Discussion
Our research indicates discrepancies and dissonance between DEs’ strongly positive intentions to use common diabetes-related technology for patients with T1D and their reported actual usage, which is occasional and not likely to be adequate to support effective disease management or patients’ communication and engagement with health care services. It also highlights key factors that can be targeted to address this gap.
To increase technology adoption, DEs’ confidence and competence, their preparation (intentions and training), and their perceptions of the ease of use of the technologies are all important. Education has been widely reported as crucial to support change in these areas,42-46 and may be targeted to help address these predictive factors. With technology use in T1D management increasing this should feature as part of routine continuing professional development for those who care for people with diabetes. The form in which this is delivered is likely to influence its uptake and effectiveness. The principles of adult learning 47 mesh with these findings to suggest such education should support DEs as autonomous and self-directed learners, should be goal and relevancy focused, and contain elements of experiential learning. There is potential for the ADEA to expand their role by initiating, promoting and/or developing and making available relevant educational programs.
Other influences were subjective norms and technologies’ perceived contribution to improving clinical practice; both could be addressed locally through, for example, experiential evidence- based workshops led by respected opinion leaders. Broadening DEs’ clinical experience by rotating local placements might also be helpful. Young adults’ experiences of pediatric diabetes care have been reported as significant influences on their expectations of care as they transition to adult-based diabetes care, with unmet expectations linked to care disengagement.48-50 Clinical placements across pediatric and adult diabetes care settings may be one means to increase DEs’ exposure to a range of care models as well as technologies, and better align the norms of practice in different settings for greater consistency of experience for young people.
Findings relating to VC were notably different to those of these other technologies. This was not surprising because this technology is used for rather different purposes; a means of conversing with patients rather than routine day to day clinical care. There are obvious differences in need for this technology, and hence exposure, for those in cities compared to regional and rural areas. However, participants may also have interpreted these questions differently. Some may have responded based on experiences with VC in the form of personal communication software such as Skype and FaceTime, whereas others may have been thinking of commercial systems managed by health care organizations; these differing systems, contexts, security concerns and technology performance may have influenced DEs’ reported attitudes and intentions. For the future, personal use of these and other diabetes-related technologies should be investigated, and how this may influence professional attitudes and behaviors, and other barriers and supports to technology use in a clinical setting.
Study limitations include the potential for responder bias and use of self-report data, intrinsic to survey design. Use of an online survey may have also preselected technology-oriented clinicians. Strengths derive from the history and rigor of the development of the model and the ensuing questionnaire instrument. Recruitment was successful across a wide and diverse geographical and sociological area, and may well have achieved a sample representative of eligible ADEA membership.
Conclusions
This research is important because it explores previously little-examined attitudes and behaviors of an essential professional group supporting people with T1D. Findings indicate discrepancies and dissonance between DEs’ strongly positive intentions toward use of common diabetes-related technology for patients with T1D and their reported actual usage, which is only occasional and probably inadequate for patient support. Continuing education using the principles of adult learning may be key in supporting DEs to align their intentions with their practice. Embedding engagement with technologies within DE practice may help maintain and improve patients’ communication and engagement with diabetes services and with this their self-management of their diabetes. While this may necessitate some resource reconfiguration, findings suggest how this may be approached to maximize realization of the potential benefits of these new but now common diabetes technologies.
Footnotes
Acknowledgements
The authors offer thanks to the survey respondents, the Australian Diabetes Educators Association (in particular Dr Joanne Ramadge, Aneesa Khan, and Vy Le) and Associate Professor Yeuping Alex Wang (clinical epidemiologist and statistician), University of Technology Sydney.
Abbreviations
ADEA, Australian Diabetes Educators Association; App, application; CGM, continuous glucose monitoring; CI, confidence interval; CSII, continuous subcutaneous insulin infusion; DE, diabetes educator; OR, odds ratio; TAM, technology acceptance model; T1D, type 1 diabetes; VC, video conferencing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.