
Abstract
Widespread and successful implementation of any glucose measurement system in a hospital point-of-care (POC) program requires a number of features in addition to accurate and reliable analytical performance. Such features include, but are not limited to, a system’s glucose-hematocrit dependence, durability, information technology capabilities, and battery capacity and battery life. While the study of Ottiger et al in this issue supports the analytical accuracy and reliability of Bayer’s CONTOUR XT® blood glucose monitoring system, the suitability of other features of this system for a hospital POC program remains to be established.
In this issue of Journal of Diabetes Science and Technology, Ottiger et al 1 evaluate the analytical performance of the CONTOUR XT® (Bayer HealthCare LLC, Tarrytown, NY) blood glucose monitoring system in a hospital point-of-care (POC) setting. Bayer markets the CONTOUR XT for patient self-testing and for use by health care professionals. The system accurately measures glucose in venous or capillary whole blood from 11 mg/dL to 600 mg/dL (0.6 mmol/L to 33.3 mmol/L). The system is not intended for diagnosis of, or screening for diabetes mellitus and Bayer warns against its use in the neonatal population. Results from the system can be transferred to and analyzed on a computer with the help of Bayer’s diabetes management software, GLUCOFACTS® Delux. GLUCOFACTS allows downloading of data onto a computer and generates various reports including a summary, logbook, and blood sugar trends.
In their article titled “Performance of a Blood Glucose Monitoring System in a Point-of-Care Setting,” Ottiger et al use control solutions and leftover venous blood samples from adults to show that the CONTOUR XT meets analytical performance specifications set forth by German (RiliBÄK), Swiss (QUALAB), and international (ISO) guidelines (Table 1). This is certainly a promising beginning for worldwide implementation of this system. It’s important to note, however, that some regions use performance criteria issued by other entities (Table 1), and it remains to be established that the CONTOUR XT satisfies these other criteria.
Performance Specifications for Blood Glucose Issued by National and International Entities.
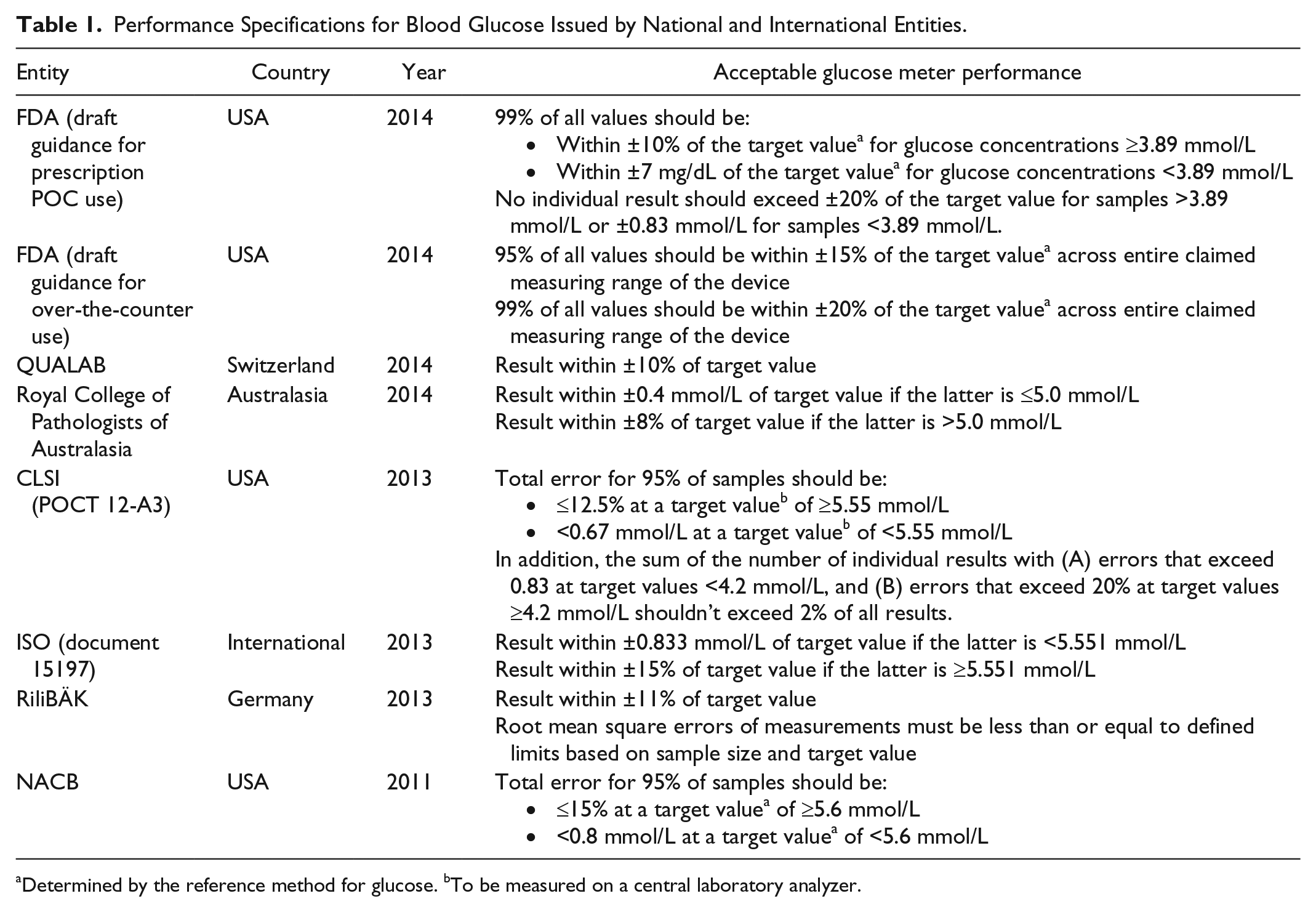
Determined by the reference method for glucose. bTo be measured on a central laboratory analyzer.
Besides precision and accuracy, the influence of hematocrit on meter performance continues to be an important analytical consideration. Before 2008, glucose meters showed significant positive bias at low hematocrits and negative bias at high hematocrits.2-5 For example, a 1993 study 2 of Accu-Chek II (Boehringer Mannheim Diagnostics, Indianapolis, IN), One Touch (Lifescan Inc, Milpitas, CA), and Stat Profile 4 (Nova Biomedical Corp, Waltham, MA) demonstrated that glucose values obtained on specimens with low (< 20%) or high hematocrits (>55%) were either falsely elevated or decreased, respectively, regardless of which meter was used. Such findings are concerning as hospitalized individuals often are anemic. POC glucose measurements in non-neonatal patients would often show factious hyperglycemia, which when treated would result in iatrogenic hypoglycemia. Newborns might exhibit factious hypoglycemia as their hematocrits may run as high as 60 to 65%. 6 Studies over the next decade continued to demonstrate this faulty glucose-hematocrit dependence. Around 2008, glucose meters began to feature hematocrit correction4,5 and since then, increasing numbers of manufacturers have embraced this technology. While the CONTOUR XT User Guide does not present hematocrit performance claims, a 2013 study showed < 10 mg/dL (< 0.6 mmol/L) bias at plasma glucose of 50 mg/dL (2.8 mmol/L) and < 10% bias at 121 mg/dL and 450 mg/dL (6.7 mmol/L and 25.0 mmol/L, respectively) for hematocrits up to 70%. 7 CONTOUR XT is thus able to compensate over a wide range of clinically relevant hematocrit levels.
In our experience, robust analytical performance is the minimum requirement for adoption of a glucose meter into a hospital POC program. With the epidemic of antibiotic resistant organisms, today’s meters must be able to endure chemical (caustic peroxide and bleach cleaning) as well as physical trauma. An additional indispensable feature is the POC glucose system’s extensive information technology (IT) capabilities. Manual recording of glucose meter results into patient charts is error-prone and can lead to incorrect clinical decisions. An audit of POC glucose results in an Italian hospital revealed that 3% of results were transcribed incorrectly and 12% of results were never transcribed. 8 To minimize the occurrence of such mistakes, it is highly desirable to have glucose meters that electronically transmit results to a data management software and subsequently into the laboratory information system, hospital information system, and/or patient medical chart. Most manufacturers of glucose measurement systems for hospital use also offer a data management software for their product (eg, Cobas IT 1000 from Roche) or permit compatibility with an independent data management software (eg, Telcor QML). In addition to enabling seamless patient data transfer, such software enhances the quality of a POC program via online user training, remote user management, QC and operator lockout, and positive patient identification. Information privacy and security is also becoming a prominent focus as more and more data is being stored on distant system servers (ie, in the “cloud”). The Diabetes Technology Society, for example, is hosting the first international conference on medical data security and privacy in May of this year. 9 While GLUCOFACTS Delux reinforces Bayer’s support of diabetes management IT, the software’s functionality lacks many features that are important for facile implementation of glucose POC within a health care system. These limitations create a significant barrier to system adoption and are likely to restrict its use to patients as well as small medical offices.
We are discovering that battery capacity and battery life are highly critical, often overlooked requirements for successful adoption of a glucose measurement system into a POC program. Glucose meters tend to be used continuously throughout the day for patient and quality control testing as well as for result transmission to/from the data management module. This continuous use makes it difficult to “dock” the meter into a charging station even for a few hours. As end-users tend to have many, diverse responsibilities there is little opportunity to monitor the charge status of a meter to expeditiously redock the meter. Glucose meter batteries must be able to recharge rapidly and must provide power for an optimal period. Discussions that we’ve had with other hospital-based POC programs suggest that currently marketed glucose meters are able to hold a charge anywhere from 6-8 hours to 3-4 days. Newer meters tend to be at the shorter end of this range because of constant Wi-Fi communication with data management software and power drainage secondary to the running of complex monitoring programs. Technical specifications for the CONTOUR XT indicate a battery life of approximately 1000 tests or 1 year average use. Definition of “average use” is not stated but instructions for the meter suggest that average use encompasses active use of the meter for glucose measurement 3-4 times per day with each use requiring several minutes. Data transfer is expected to be minimal with 1 or 2 transfers per week. While the claimed battery life is aligned with the intended use of the system, battery performance would be unclear under the more demanding conditions of a hospital POC program. In addition, various users are discovering that the frequent battery recharging seems to be damaging the battery and reducing battery life.
In summary, the study of Ottiger et al 1 in this issue of Journal of Diabetes Science and Technology supports the results of several previous reports7,10-13 on the accuracy and reliability of Bayer’s CONTOUR XT blood glucose monitoring system. However, it remains to be seen whether other features of this system, including durability, IT capabilities, and battery life, are conducive to its widespread implementation in hospital POC programs.
Footnotes
Abbreviations
CLSI,Clinical & Laboratory Standards Institute; FDA, US Food and Drug Administration; ISO, International Organization for Standardization; IT, information technology; NACB, National Academy of Clinical Biochemistry; POC, point of care; QUALAB, Richtlinie der Schweizerischen Kommission für Qualitätssicherung im medizinischen Labor; RiliBÄK, Richtlinien der Bundesärztekammer zur Qualitätssicherung laboratoriumsmedizinischer Untersuchungen.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.