
Abstract
Virtual reality (VR) technology can provide a safe environment for observing, learning, and practicing use of behavioral weight management skills, which could be particularly useful in enhancing minimal contact online weight management programs. The Experience Success (ES) project developed a system for creating and deploying VR scenarios for online weight management skills training. Virtual environments populated with virtual actors allow users to experiment with implementing behavioral skills via a PC-based point and click interface. A culturally sensitive virtual coach guides the experience, including planning for real-world skill use. Thirty-seven overweight/obese women provided feedback on a test scenario focused on social eating situations. They reported that the scenario gave them greater skills, confidence, and commitment for controlling eating in social situations.
Training in empirically validated behavioral weight management skills such as goal-setting, self-monitoring, and stimulus control (eg, changing and coping with cues for overeating and inactivity) is the foundation of behavioral weight loss treatment (BWL), which produces clinically significant weight losses of 5-10% of initial body weight and lowers risk of type 2 diabetes. 1 BWL skills training is typically delivered in face-to-face group sessions. 2 Online delivery of skills training increases reach and reduces costs, 3 but is often associated with suboptimal weight losses. 4 According to social learning theory, the methods typically used for online skills training (static text, audio, and/or video lessons), which lack interactivity and the opportunity to observe and practice skills use, may be inadequate and therefore lead to lower weight loss compared to face-to-face treatment. 5
This journal published a special issue 6 describing how virtual reality (VR) technology could improve adherence to BWL skills, 7 and ultimately improve weight losses, by providing a safe environment in which to observe, learn, and practice skills use.7,8 A few early studies showed that VR could be used for these purposes, but most relied on a human counselor to guide the experience, thus limiting their reach and increasing cost.9-11
The goal of the Experience Success (ES) project was to develop a system for creating and deploying automated VR scenarios for online training in BWL skills, and collect feedback from test users with an initial social eating scenario.
Design and Development of the VR Delivery System & Social Eating Scenario
The ES system was programmed by Virtually Better, Inc (Decatur, GA) using Unity (Unity Technologies, San Francisco, CA) and 3D Studio Max (Autodesk, Inc, San Rafael, CA) software. All 3D models were optimized for real-time rendering performance, with the final executable published for Windows and Mac operating systems.
The ES social eating scenario targeted (1) knowledge of barriers that interfere with eating control, (2) behavioral skills to cope with these barriers, (3) confidence for using these skills, and (4) commitment to using these skills in real-world situations. Participants began by choosing a coach from 8 virtual characters of varying gender and race/ethnicity, who was shown standing outside a suburban home. The coach explained that the participant would face challenges to their weight control efforts while visiting a party. The coach also explained that there are no correct or incorrect answers to the challenges; rather the goals are to (1) experience using a variety of skills, (2) observe the outcomes, and (3) plan for real-world situations.
Participants then entered the house and were met by the VR hostess and partygoers. Users faced 2 types of challenges: interpersonal and practical. Interpersonal challenges included (1) whether to disclose weight loss efforts to the other partygoers, (2) how to cope with peer pressure to overeat, and (3) how to respond to intrusive/negative comments about weight loss efforts. At predefined moments participants engaged in conversation with partygoers by using the mouse to select from 2 to 5 dialogue choices at a time (Figure 1).

Example interaction during a conversation with partygoers.
Practical challenges involved whether to “consume” a healthy snack before entering the party, and how to build a plate of food that is consistent with weight loss goals from a party buffet. At the buffet, the user was instructed to build a plate of food (13 choices) and choose a beverage (5 choices) (Figure 2), ranging in healthfulness (eg, fruit salad, lasagna, meatballs; water, wine, margaritas). Participants first chose a plate, large or small, holding a maximum of 8 or 4 portions of food, respectively. Participants clicked foods to add portions to their plate (from 0 to maximum portions) and then chose a beverage. The coach then gave feedback on the total calorie content and individual choices related to the amount and composition of the food and drink selected. The user could then proceed to the next interaction or build another plate.

View of virtual foods in the plate-building challenge.
Choices made at each step in the scenario affected partygoers’ preprogrammed behavior and response options available during subsequent challenges. For example, disclosing efforts to lose weight to the other partygoers resulted in (1) some partygoers became more supportive, (2) “unlocked” response options for coping with peer pressure (eg, “The cake looks delicious, but I’m going to stick with the fruit salad since I’m working on my weight.”), and (3) more intrusive comments from a partygoer critical of weight loss efforts. Thus, the scenario was not aimed at promoting a narrow range of “correct” behaviors, but rather gave participants an experience of trying various skills and experiencing both positive and negative outcomes in a realistic way.
The final step of the scenario involved a debriefing with the coach outside the home. The coach reviewed the participant’s choices and experiences at the party, highlighted some suggestions for real-world behavior change, and guided development of a contract for making specific real-world changes at social events.
Test User Feedback
Thirty-seven overweight/obese women (mean ± SD age = 55.0 ± 8.2 years, BMI = 34.6 ± 5.4 kg/m2; 97.3% non-Hispanic white) in week 8 of an 18-month BWL trial (RCT; Live SMART 12 ) participated in a feedback session involving pretest questionnaires, access to the ES social eating scenario, and posttest questionnaires. They received a $25 honorarium. Questionnaires assessed demographic characteristics (pretest only); difficulties, barriers, skill level, confidence, and commitment related to controlling eating in social situations; and acceptability/feasibility of the scenario (posttest only). Paired t tests were used to evaluate change in measures pre/post the ES scenario. Verbal feedback was also solicited.
All participants completed the ES scenario in about 15 minutes without assistance. Knowledge of barriers to controlling eating in social situations was unchanged, but level of skills, confidence, and commitment to controlling eating in social situations were all significantly improved (Table 1) at posttest. The mean ± SD for the acceptability/feasibility items combined was 6.5 ± 0.6 on a 7-point Likert-type scale. The most common feedback described the scenario as highly realistic, but some dialogue reportedly “did not seem like something I would say” (n = 15), and some of the buffet foods reportedly lacked detail and/or did not appear fully realistic (n = 12).
Results of Test User Feedback.
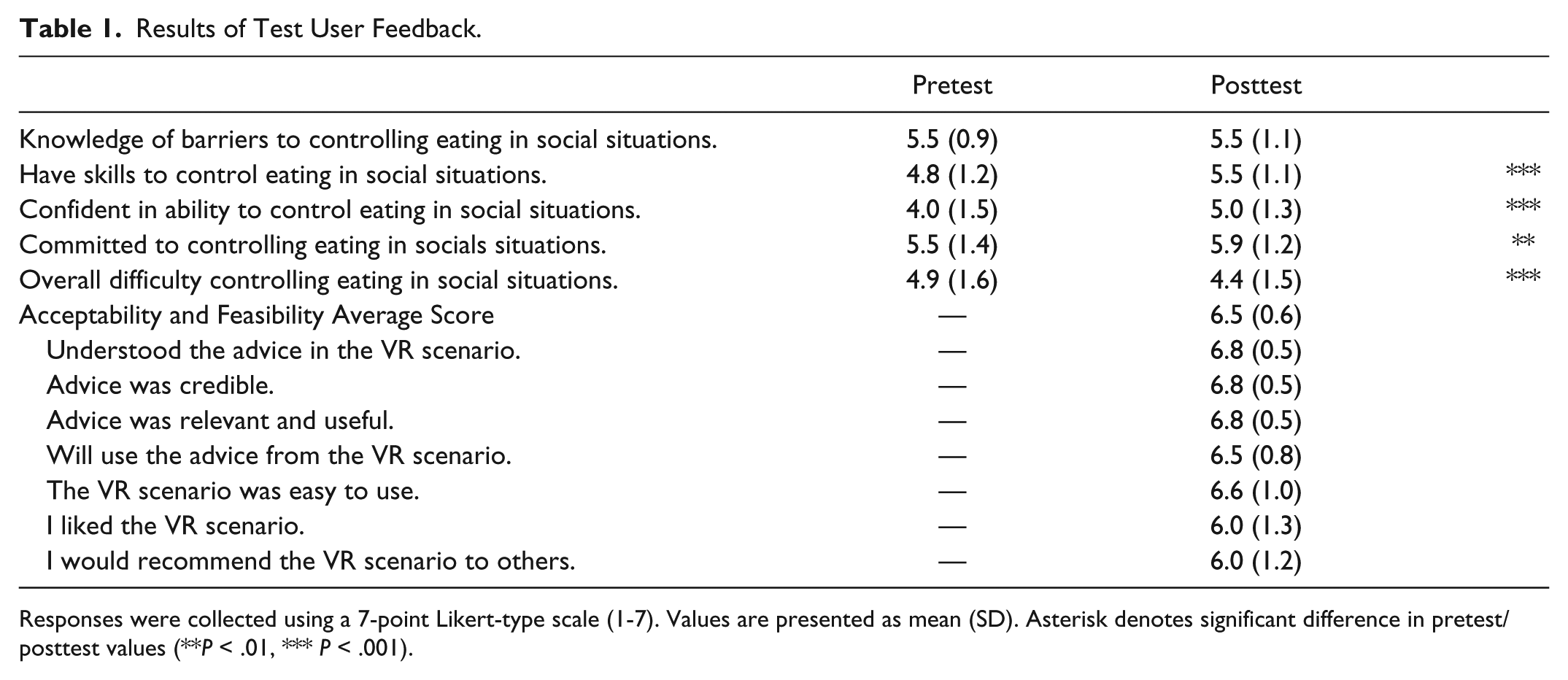
Responses were collected using a 7-point Likert-type scale (1-7). Values are presented as mean (SD). Asterisk denotes significant difference in pretest/posttest values (**P < .01, *** P < .001).
Discussion and Conclusions
The ES system demonstrates VR technology’s potential to deliver training in weight management skills. The fully automated nature of the intervention differentiates it from the few other VR interventions targeting weight manage-ment skills training. Previously, VR interventions primarily involved delivery of traditional face-to-face treatment in a virtual environment with group leaders and patients attending and participating in avatar form.10,11 The avatars were customized with a patient’s appearance to demonstrate basic weight management behaviors (eg, walking on a treadmill at medium intensity), 9 or using VR as an adjunct to face-to-face treatment to reinforce skills training and change weight-related cognitions. 13 Because the ES system is automated, requires no special equipment (eg, goggles), and is designed for web-based delivery, it may someday be possible to provide experiential training in weight management skills to large numbers of patients at low cost via technology they already own (eg, PCs, tablets, smartphones).
The initial ES scenario was rated as acceptable, feasible, and helpful in a preliminary feedback session. However, the feedback highlights the difficulty in crafting a VR experience that is uniform for participants, but is perceived as realistic; the most common criticisms pertained to the response options available in conversation and the appearance of foods, which can be difficult to model realistically in VR and may be expected to appear differently depending on each patient’s life experience. This may be particularly true for the typical older adult seeking weight loss, who may have little prior experience with virtual worlds. 14 Planned research will determine whether these challenges can be overcome, and whether a full complement of ES scenarios targeting environments such as the home, workplace, and gym can improve weight losses produced by online BWL (R42 DK103537).
Footnotes
Abbreviations
BWL, behavioral weight loss treatment; ES, Experience Success; RCT, randomized controlled trial; SD, standard deviation; VR, virtual reality.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JSS was a full-time employee of Virtually Better, Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the National Heart, Lung, and Blood Institute (R41 HL114046).