
Abstract
Background:
Telehealth-supported clinical interventions may improve diabetes self-management. We explored the feasibility of stepwise self-titration of oral glucose-lowering medication guided by a mobile telephone-based telehealth platform for improving glycemic control in type 2 diabetes.
Methods:
We recruited 14 type 2 diabetes patients to a one-year feasibility study with 1:1 randomization. Intervention group patients followed a stepwise treatment plan for titration of oral glucose-lowering medication with self-monitoring of glycemia using real-time graphical feedback on a mobile telephone and remote nurse monitoring using a Web-based tool. We carried out an interim analysis at 6 months.
Results:
We screened 3476 type 2 diabetes patients; 94% of the ineligible did not meet the eligibility criteria for hemoglobin A1c (HbA1c) or current treatment. Mean (standard deviation) patient age at baseline was 58 (11) years, HbA1c was 65 (12) mmol/mol (8.1% [1.1%]), body mass index was 32.9 (6.4) kg/m2, median [interquartile range (IQR)] diabetes duration was 2.6 (0.6 to 4.7) years, and 10 (71%) were men. The median (IQR) change in HbA1c from baseline to six months was −10 (−21 to 3) mmol/mol (−0.9% [-1.9% to 0%]) in the intervention group and −5 (−13 to 6) mmol/mol (−0.5% [-1.2% to 0.6%]) in the control group. Six out of seven intervention group patients and four out of seven control group patients changed their oral glucose-lowering medication (p = .24).
Conclusions:
Self-titration of oral glucose-lowering medication in type 2 diabetes with self-monitoring and remote monitoring of glycemia is feasible, and further studies using adapted recruitment strategies are required to evaluate whether it improves clinical outcomes.
Keywords
Introduction
Diabetes is one of the most prevalent chronic medical conditions worldwide, 1 and its complications are well documented.2–5 In clinical trials, tight glycemic control reduces the risk of complications in patients with type 2 diabetes;6–9 however, it is difficult to achieve and maintain in clinical practice. 10 Improvements in population glycemic control have been modest,11,12 indicating the need to explore new, potentially more effective approaches to supporting patients in improving their individual glycemic control.
Currently recommended treatment regimens require active dose titration with both first- and second-line oral glucose-lowering medications.13,14 Dose adjustments are typically initiated by clinicians in response to elevated hemoglobin A1c (HbA1c) measurements or, where used, self-monitored blood glucose (SMBG) measurements. The rate of titration to an adequate dose is limited by the frequency of patient contact with their health care providers and, where used, the time intervals between routine HbA1c measurements. Although the extent of clinical benefit from routine SMBG is controversial,15,16 short-term self-monitoring may be a feasible approach for promoting more rapid attainment of optimal treatment intensity while reducing the risk of hypoglycemia.
Previous studies showed that patients with type 2 diabetes can effectively self-titrate insulin based on conventional SMBG17,18 or telehealth support and monitoring.19,20 These studies suggest that self-titration of treatment is acceptable to patients with type 2 diabetes. The approach may, therefore, potentially be applied to oral glucose-lowering medication. As with self-titration of insulin, 18 defining specific titration increments would be necessary for self-titration of oral glucose-lowering medication. We hypothesized that this may be achieved by suggesting that patients and clinicians follow a stepwise treatment plan similar to those used in the care of asthma patients. 21
A mobile telephone-based telehealth platform, with real-time graphical feedback to patients and remote clinician monitoring of blood glucose levels, was feasible and acceptable in studies of patients with type 1 and type 2 diabetes receiving insulin treatment.19,22 Such an approach might provide the additional support required to implement patient self-titration of oral glucose-lowering medication.
The aim of this article is to present the protocol, the interim feasibility results, and the experience, to date, of studying the stepwise self-titration of oral glucose-lowering medication facilitated by a previously assessed mobile telephone-based telehealth platform in patients with type 2 diabetes.
Methods
Design
Medication adjustment for type 2 diabetes using SMBG with telehealth support (MATS) is a small-scale, open parallel group randomized controlled feasibility study carried out in primary care. In this article, we describe the design of this feasibility study and report the results of the study to date.
Patients and Settings
Patients were recruited from seven general practices in Oxfordshire and Buckinghamshire, United Kingdom. Those eligible were ≥35 years old with type 2 diabetes of at least 3 months' duration and were taking oral glucose-lowering medication. We recruited patients who had last routinely measured HbA1c ≥64 mmol/mol (8.0%) and <97 mmol/mol (11.0%) with no subsequent records of increase in oral glucose-lowering medication. Patients were excluded if they were unable to follow the trial protocol due to physical, cognitive, or social limitations; were prescribed insulin; or required addition of insulin to treatment regimen. Other exclusion criteria were visual impairment, pregnancy or breast feeding, and limited life expectancy or other comorbid conditions making tight blood glucose control inappropriate.
Intervention
The telehealth intervention included regular SMBG to guide self-titration of oral glucose-lowering medication under the supervision of the research nursing staff whose primary tasks were to ensure patient safety and correct use of the telehealth system. The self-titration followed an individualized stepwise treatment plan (available from the corresponding author) approved at the baseline visit by the patient's general practitioner. The treatment plan included a number of discrete successive medication doses (steps) based on the recommendations of the National Institute for Health and Clinical Excellence (NICE). 13
The intervention group patients received a mobile telephone (Nokia 7230, Nokia Corporation, Espoo, Finland) and a blood glucose meter (OneTouch Ultra 2™, LifeScan, Milpitas, CA) with a Bluetooth™ cradle (t+ Medical, Abingdon, UK) and were asked to perform at least six blood glucose tests per week, of which at least three were required to be fasting. Blood glucose readings were transmitted by Bluetooth from the glucose meter to the mobile telephone and then uploaded to a central server through the mobile 3G network. The telehealth system used in this study (t+ Diabetes, t+ Medical, Abingdon, UK) included a mobile telephone diary application for patients, with real-time graphical feedback on glucose levels. Patients also received graphical user guides to the telephone application and example screens to aid decisions on self-titration. The blood glucose readings were also monitored by the research nursing staff twice a week via a Web-based monitoring system
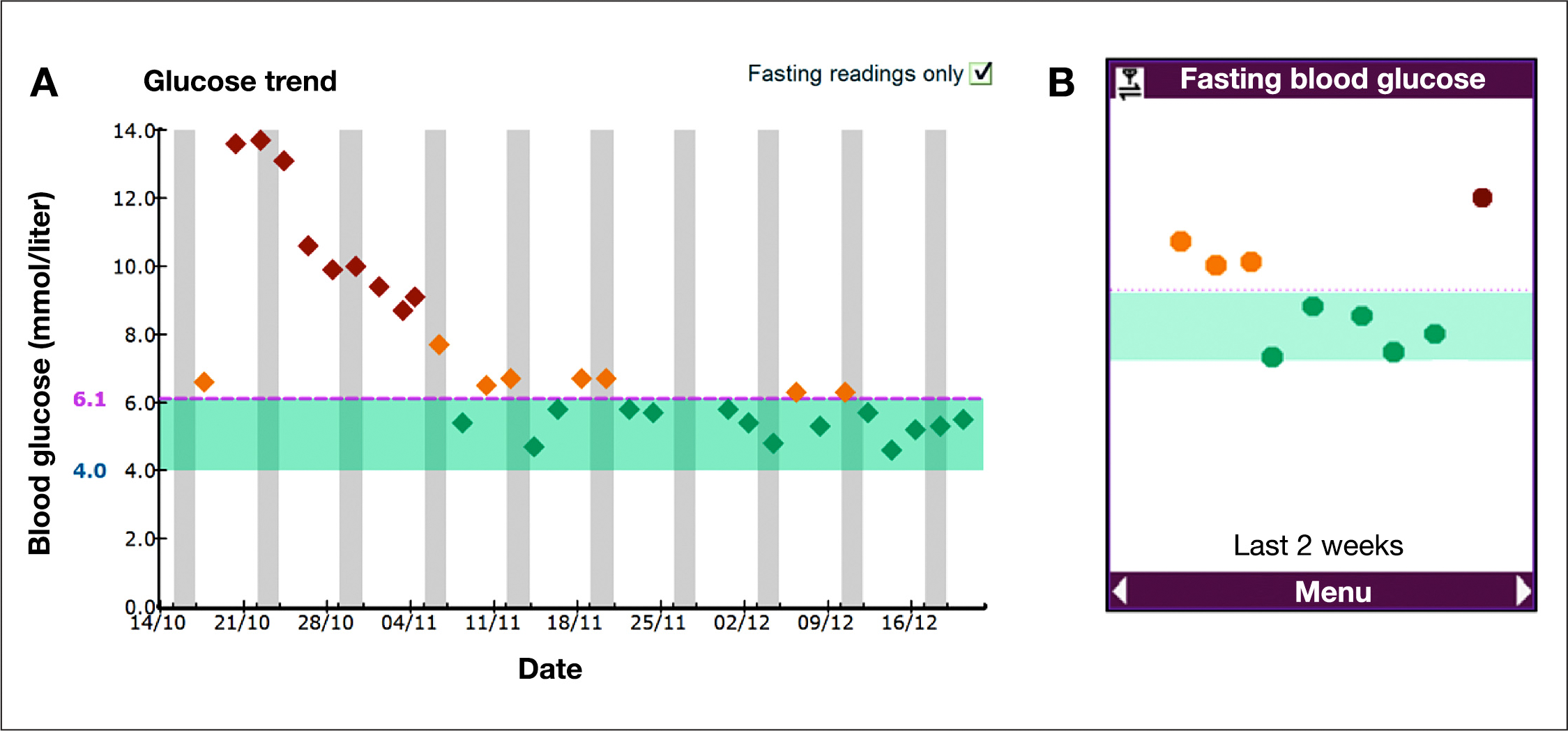
Remote blood glucose monitoring and self-monitoring components of the telehealth intervention.
Patients used the phone application to review their glucose levels every 3 weeks and, if necessary, titrate their oral glucose-lowering medication to achieve a target fasting blood glucose of ≤110 mg/dl, or ≤126 mg/dl if 65 years or older, or the highest tolerated dose. If blood glucose control remained suboptimal at a maximum dose of the first oral glucose-lowering medication, a second medication was added. The dose of oral glucose-lowering medication was down-titrated in the event of symptomatic hypoglycemia, or at least four blood glucose readings <72 mg/dl over a 2 week period. Patients stopped self-monitoring when target blood glucose levels were achieved and resumed self-monitoring prior to quarterly visits and if 3-monthly HbA1c was >53 mmol/mol (7.0%). In both intervention and control groups, oral glucose-lowering medication dose was increased at the clinician's discretion if 3-monthly HbA1c values were outside of the target range recommended by the NICE [≤48 mmol/mol (6.5%) with none or one oral glucose-lowering medication, ≤58 mmol/mol (7.5%) with two oral glucose-lowering medications]. The detailed titration protocol is provided in
Both intervention and control group patients received a supportive lifestyle-focused intervention consisting of monthly telephone calls, during which diet, physical activity, and recent changes in medication were discussed. In the control group, medication titration followed the procedures of routine care of patients with diabetes. We did not instruct the control group patients to use SMBG.
Outcomes
We report here the demographic, health, and treatment-related characteristics of recruited patients. We also report the 6-month data on changes of HbA1c and changes of oral glucose-lowering medication defined as changes in dose or quantity of medications.
Procedures
Practice staff identified eligible patients using computerized patient records and sent them brief study descriptions with invitations to contact the coordinating center for further details on joining the study. Those who responded and agreed to participate had their eligibility confirmed during an initial telephone assessment and were then individually randomized to intervention or control groups. Randomization was carried out independently of the research nursing staff by the study coordinator using a computerized minimization algorithm balancing for age, gender, and duration of diabetes.
Patients agreed to attend their practice at baseline and at 1 year to discuss their treatment. In addition, three extra visits were scheduled for blood sample collection. During the baseline visit, all patients had the opportunity to ask further questions and clarify their involvement and then provided written consent. Those patients allocated to the intervention group received training (30–45 min) on SMBG and the use of the telehealth system. At both baseline and final (month 12) visits, the research nursing staff obtained blood samples for HbA1c and recorded blood pressure, weight, and treatment regimen. Height was only recorded at baseline visit. During the three interim practice visits, blood samples for HbA1c were obtained by the practice nurse. Prior to the baseline, 6-month, and final visits, patients were sent a study questionnaire.
The research nursing staff received a formal training session and a printed manual to promote fidelity to intervention delivery. The baseline visit and monthly telephone calls followed a standardized algorithm. The research nursing staff were instructed not to initiate any discussions about the treatment regimen during telephone contacts with the control group patients except when identifying recent changes in medication. Any requests for specific medication advice were directed to the patient's practice nurse or physician.
Measurements
Patient age; gender; duration of diabetes; last total and high-density lipoprotein cholesterol values; current glucose-lowering, lipid-lowering, and antihypertensive treatments were obtained from practice records. Ethnicity, total number of prescribed medications, and prior SMBG were reported by the patient at the baseline visit. Blood pressure was recorded using an electronic sphygmomanometer conforming to the recommendations of the European Society of Hypertension. 23 Systolic and diastolic blood pressure, height, and weight were measured by the research nurse. Hemoglobin A1c concentration was measured in a Diabetes Control and Complications Trial-aligned 24 central laboratory (Clinical Biochemistry Laboratory, Oxford University Hospitals Trust, Oxford, UK).
Data on changes in oral glucose-lowering medications were obtained by the research nurses during monthly telephone calls. Hypoglycemia was defined as hypoglycemic symptoms or blood glucose <56 mg/dl or both. We recorded a narrative account of the feedback provided and problems encountered by patients and clinical staff while using the telehealth platform.
Ethics and Governance
The study protocol was approved with a reference number 10/H0502/18 on April 16, 2010, by the Southampton and South West Hampshire Research Ethics Committee, National Research Ethics Service (Southampton, UK).
Statistical Analyses
We performed an unblinded analysis of data obtained prior to and including 6 months in this analysis. We analyzed data from patients who met the inclusion criteria and attended the study baseline visit. Missing HbA1c values were substituted with closest routinely available HbA1c measurements obtained from the practice records. We assumed no change in oral glucose-lowering medication if no contact was made with the patient at the monthly telephone call, but the oral glucose-lowering medication recorded immediately prior to and immediately after the unsuccessful contact attempt were the same.
We present normally distributed continuous data as mean and standard deviation (SD) and non-normally distributed variables as median and interquartile range (IQR). The uncertainty in measurements was reported as 95% confidence intervals (CIs). Mean values of HbA1c were compared using a two-tailed t-test. We used linear logistic regression analysis to determine between-group differences in HbA1c with adjustment for baseline values. We compared the numbers of patients who changed their oral glucose-lowering medication using a χ 2 test. Statistical analyses were performed using STATA 11.1 SE (StataCorp LP, College Station, TX), and the line chart of mean HbA1c over time was constructed using R version 2.14 (R Foundation for Statistical Computing, Vienna, Austria).
Results
From October 2010 to June 2011, 17 patients were recruited into the MATS study, and a detailed flow diagram is shown in
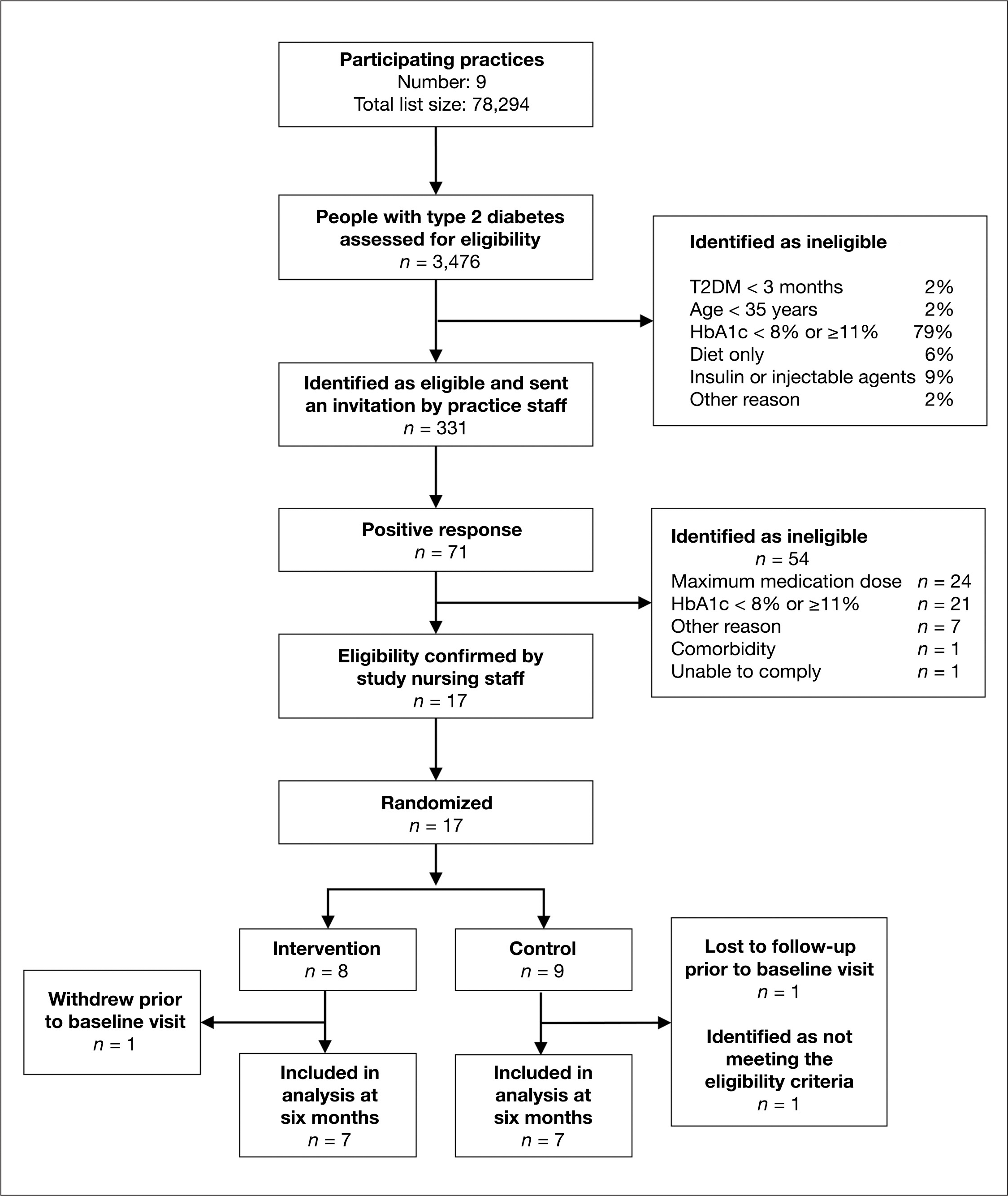
Study flow diagram. T2DM, type 2 diabetes mellitus.
Baseline Population Characteristics of Patients Included in the Study a
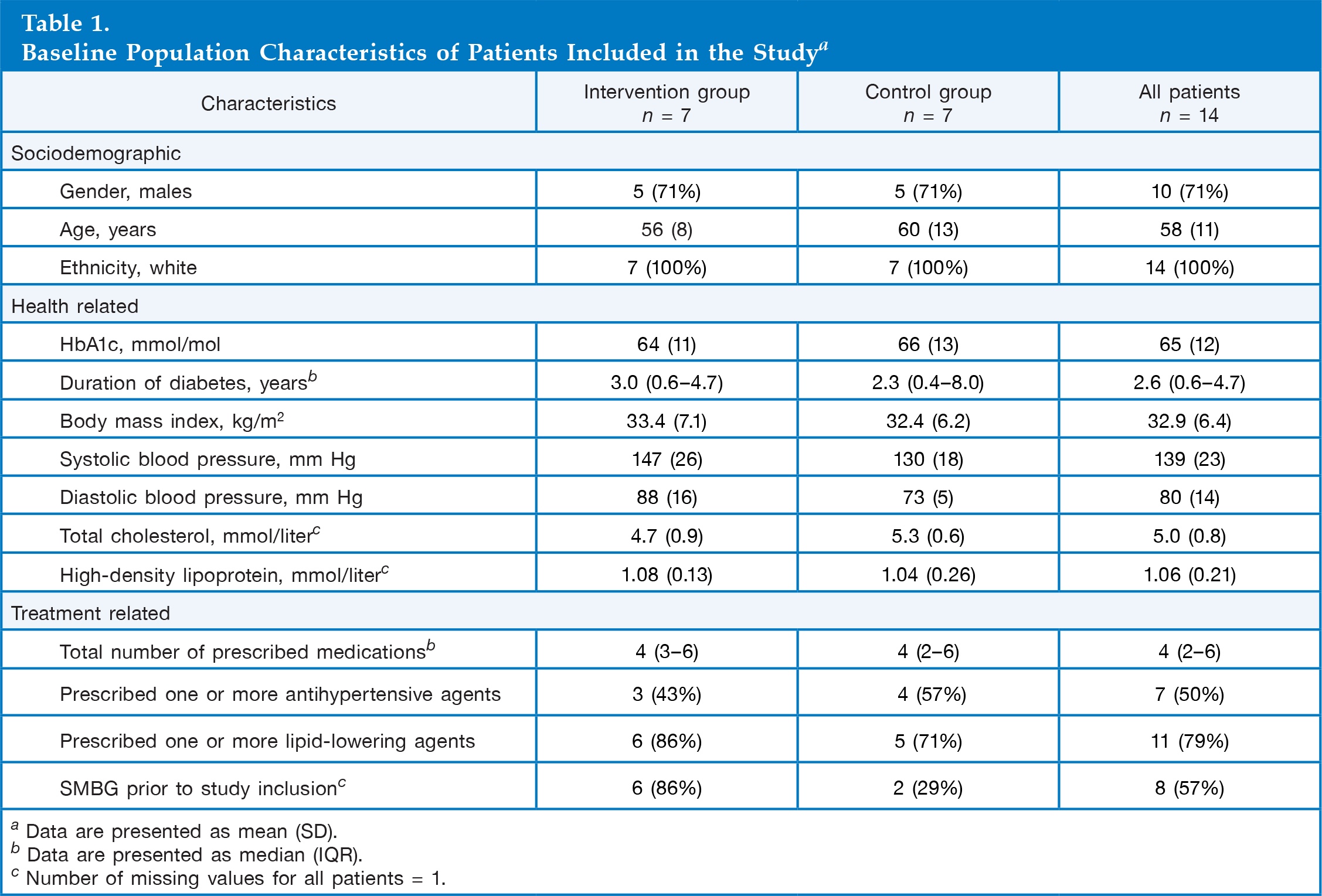
Data are presented as mean (SD).
Data are presented as median (IQR).
Number of missing values for all patients = 1.
Change in Hemoglobin A1c
Complete per-protocol series of HbA1c measurements up to and including the month 6 visit were available in 10 patients. Two patients missed one of the three study visits, and 2 other patients missed two visits.
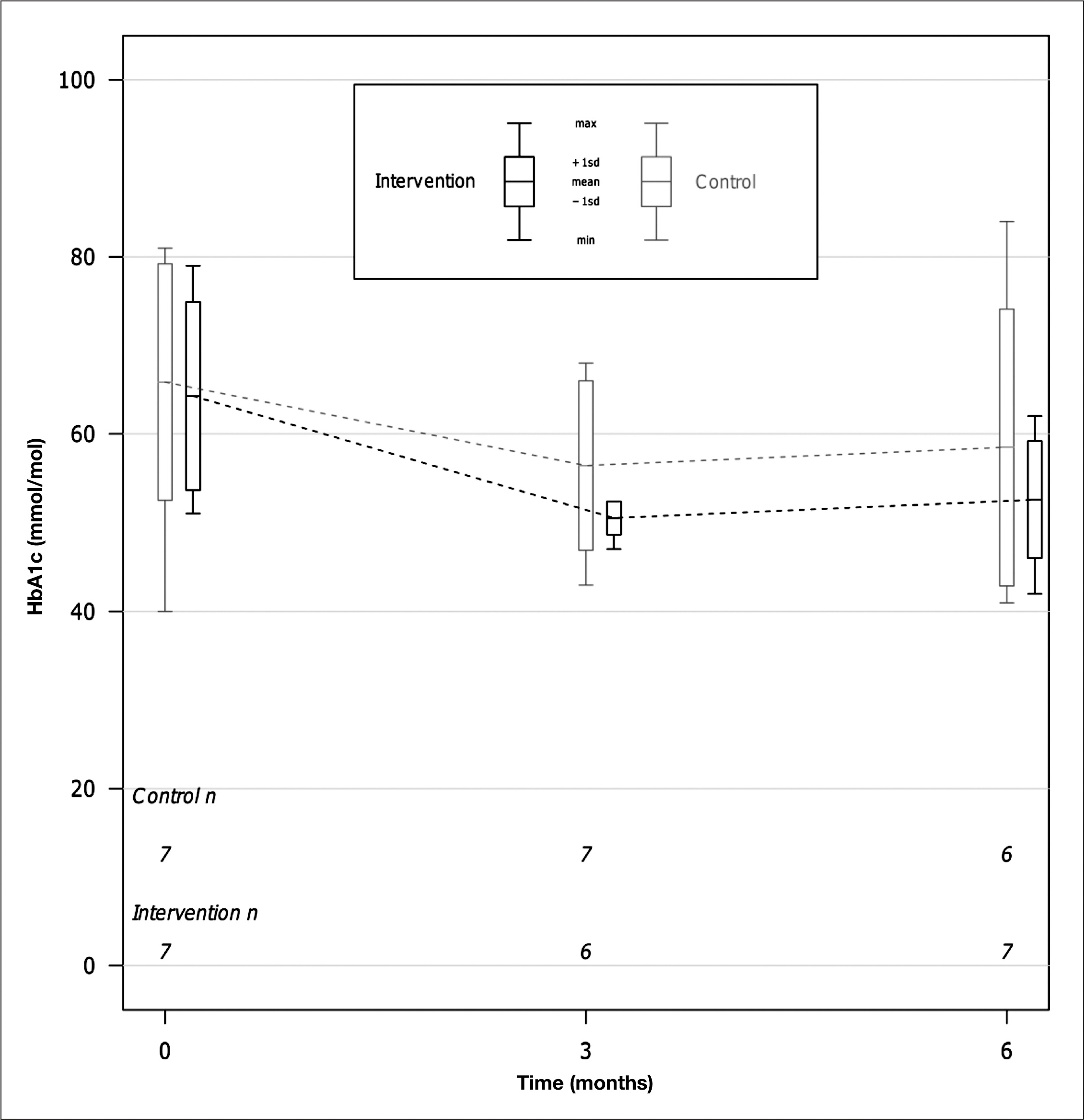
Changes of HbA1c level in the telehealth intervention and control groups from baseline to 3 and 6 months.
The mean (SD) HbA1c at 6 months in this study sample was 55 (12) mmol/mol [7.2% (1.0%)], which was 9 (CI 0 to 17; p = .04) mmol/mol (0.8% [CI 0.1% to 1.5%]) lower compared with baseline. The median (IQR) change in HbA1c from baseline to 6 months was −10 (−21 to 3) mmol/mol (−0.9 [-1.9 to 0%]) in the intervention group and −5 (−13 to 6) mmol/mol [-0.5% (−1.2% to 0.6%)] in the control group. When adjusted for baseline, the mean HbA1c at 6 months was 6 (CI −20 to 8; p = .35) mmol/mol [0.6% (CI −1.9% to 0.7%)] lower in the intervention group compared with the control group, although this difference was not significant.
Individual Hemoglobin A1c Measurements
Hemoglobin A1c measurements both at baseline and at 6 months were available in six patients from the control group and in seven patients from the telehealth intervention group. Among these patients, three in the control group and five in the telehealth intervention group had a decrease in HbA1c from baseline to 6 months; three patients from the control group and two patients from the telehealth intervention group had an increase in HbA1c.
Oral Glucose-Lowering Medication
Complete per-protocol series of telephone calls, during which data on the treatment regimen were collected, were made in nine patients; three patients could not be contacted for one monthly telephone call, and two patients could not be contacted during two or more subsequent monthly call attempts.
Over the first 6 months of the study, four out of seven patients in the control group and six out of seven patients in the intervention group had a change in their oral glucose-lowering medication (p = .24). Out of 15 changes in medication recorded to date, 12 (8 in the intervention group and 4 in the control group) took place during the first 3 months of the study.
Safety
One patient in the intervention group reported hypoglycemia. This report was not confirmed by objective blood glucose measurements. Using the remote monitoring system, a research nurse also detected that another intervention group patient had two fasting blood glucose readings <56 mg/dl. Both the patient and their general practitioner were notified. We recorded no other serious intervention-related adverse events.
Feasibility
The Clinicians' Perspective
Both practice nurses and research nurses were interested in the telehealth platform and optimistic about its potential role in routine health care, although they had no previous experience with telehealth. The practice nurses agreed that the telehealth support would complement the care provided at their practices.
The study-coordinating group held a series of meetings in three practices to present the technology and discuss its use. In all the three practices, the staff saw self-titration using the telehealth platform as potentially useful in providing care to patients who were reluctant to increase the intensity of their treatment regimen or found it difficult to visit their health care provider regularly.
The Patients' Experience
Overall, based on the feedback from the research nurses, the patients were enthusiastic about using the telehealth platform. The concept of adjusting their glucose-lowering medication based on the results of SMBG was new to the patients. The research nurses reported that, overall, the patients understood how to adjust their medication based on the blood glucose graphs available via the mobile telephone application.
Patients were initially uncertain about making the decision themselves to change the dose of their blood glucose-lowering medication. The episodes of such uncertainty, including indication of readiness to adjust the medication without actually adjusting, mostly occurred at early stages of using the platform. In such cases, the patients typically followed the intervention protocol correctly after a reminder of the criteria for adjusting their medication. One patient was concerned about uptitrating because of a period of traveling.
The technical difficulties typically required minor interventions such as battery replacement or removing a blood glucose testing strip from the glucose meter to proceed with data transmission.
Discussion
Interim reports from patients and clinical staff involved in the study suggest that the use of a telehealth platform may be feasible in primary care. Self-titration of oral glucose-lowering medication with telehealth support may have potential to improve clinical outcomes. The average HbA1c measurement at 6 months was 6 mmol/mol (0.6%) lower (p = .35) in the intervention group compared with the control group. Although this difference was not statistically significant, a clinical effect of this size, if sustained in further studies, would be important in controlling diabetes.
To our knowledge, this is the first study to assess the feasibility and clinical efficacy of stepwise self-titration of oral glucose-lowering medication based on a telehealth platform including SMBG and remote telehealth support by a clinician. Self-titration of insulin with or without telehealth support has been studied previously,17–19 and self-titration with telemonitoring has been successfully used in the treatment of hypertension. 25 However, the feasibility of self-titration of oral glucose-lowering medication remained unexplored although self-monitoring had been proposed as a way to support patients in making treatment-related decisions. 26
In combination, self-titration and remote monitoring using the assessed telehealth platform may promote achievement of appropriate oral glucose-lowering medication levels while minimizing the risk of hypoglycemia—an important factor that may limit treatment intensity. 27 The initial uncertainty of some patients in self-titration of their medication may potentially be addressed by modifications in the telehealth platform.
In this study, the telehealth platform played an important role, as it not only enabled data collection and remote monitoring, as demonstrated using other telehealth systems, 28 but also supported patients in making independent medication titration decisions. Remote monitoring by a research nurse in such a scenario is auxiliary, as the telehealth user could, potentially, manage his treatment independently. The study patients, research nursing staff, and practice clinicians had no previous experience in telehealth, although there was an imbalance in previous use of SMBG between intervention and control groups. This study allowed us to explore the feasibility of the study intervention in general patient population and primary care clinicians with usual level of expertise.
The sample size used was appropriate for a feasibility study but limited the power of the quantitative comparisons in detecting differences between the study groups. We experienced difficulty with recruitment because we targeted patients with suboptimal glycemic control in the context of an incentive scheme for physicians to improve care in this group. 29 Identification of potential study participants using a wide scale strategy rather than contacting individual general practices may be more appropriate in implementing and evaluating this intervention. We developed the intervention as a theoretically coherent package building on the engineering concept of a “closed-loop” system. Therefore, we did not explore the effects of individual components of the intervention.
Although, in this analysis, we did not assess whether the use of the platform and potential clinical benefits would persist beyond 6 months, the duration of follow-up was similar to many comparable randomized controlled trials reported to date.30,31 Recruitment of patients from only a single ethnic group may limit the generalizability of our findings. The use of informal feedback from research and primary care nurses to assess the feasibility of the telehealth platform reflects the pilot nature of this study.
Conclusions
This study demonstrated that self-titration of oral glucose-lowering medication in type 2 diabetes with self-monitoring and remote monitoring of blood glucose levels by clinical staff was feasible in primary care and may improve clinical outcomes. Further studies are needed to assess the costs and confirm or disprove the potential clinical efficacy of self-titration of oral glucose-lowering medication based on a telehealth platform.
Footnotes
Abbreviations:
This study was funded by the National Institute for Health Research School for Primary Care Research and the National Institute for Health Research Biomedical Research Centre Programme, Oxford, United Kingdom.
Acknowledgments:
We are grateful to Jason Oke for providing a figure for the article.