
Abstract
Background:
Our motivation for this study was to develop a noninvasive glucose sensor for low birth weight neonates. We hypothesized that the underdeveloped skin of neonates will allow for the diffusion of glucose to the surface where it can be sampled noninvasively. On further study, we found that measurable amounts of glucose can also be collected on the skin of adults.
Method:
Cellulose acetate dialysis membrane was used as surrogate for preterm neonatal skin. Glucose on the surface was collected by saline-moistened swabs and analyzed with glucose-binding protein (GBP). The saline-moistened swab was also tested in the neonatal intensive care unit. Saline was directly applied on adult skin and collected for analysis with two methods: GBP and high-performance anion-exchange chromatography (HPAEC).
Results:
The amount of glucose on the membrane surface was found (1) to accumulate with time but gradually level off, (2) to be proportional to the swab dwell time, and (3) the concentration of the glucose solution on the opposite side of the membrane. The swab, however, failed to absorb glucose on neonatal skin. On direct application of saline onto adult skin, we were able to measure by HPAEC and GBP the amount of glucose collected on the surface. Blood glucose appears to track transdermal glucose levels.
Conclusions:
We were able to measure trace amounts of glucose on the skin surface that appear to follow blood glucose levels. The present results show modest correlation with blood glucose. Nonetheless, this method may present a noninvasive alternative to tracking glucose trends.
Introduction
This article describes our initial efforts to develop a noninvasive method to determine glucose levels in low birth weight and preterm neonates. The primary objective was to develop a glucose sensor that is noninvasive/painless, is more accurate and sensitive than current sensors, is easy to use by staff, and produces rapid results. The method of sampling takes advantage of the high permeability of the underdeveloped cutaneous layer of neonatal skin. We hypothesized that this permeability will allow small molecules like glucose to diffuse passively to the surface of the skin and be available for sampling, albeit in small amounts. The glucose biosensor for this method is a recombinant fluorescent glucose-binding protein (GBP), which, in nature, is responsible for chemotaxis in gramnegative bacteria and, therefore, has undergone natural selection to be sensitive to very low (μm) levels of glucose and be highly glucose selective, even in complex media. Our group has labeled the GBP with fluorescent dye(s) and has previously demonstrated optical sensing of glucose using this biosensor.1–8
The primary motivation for noninvasive glucose sensing is that current blood glucose monitors require intermittent blood collection through a skin-penetrating prick on the finger or the heel of neonates. This procedure is painful, messy, and not conducive to good patient compliance. The same point-of-care devices for glucose testing in adults are currently used for neonates. Thus they present added issues specific to neonates, such as threat of infection, long-term effects of pain, and potential anemia from frequent blood draws. A true noninvasive, painless, and accurate glucose sensor is a “holy grail” not only in neonatal glucose monitoring, but in adults as well. Several spectroscopic methods 9–13 have been in development for years, including near-infrared, mid-infrared, Raman, 14 photo acoustic, 15 and terahertz spectroscopy. 16 The methods generally involve exposing the skin to radiation and teasing out the minute signal from the blood and tissue glucose. These noninvasive methods suffer from large background interferences (generally from water but also molecules with glucose-like structures), requiring multiple corrections on the hardware and software. None have resulted in a commercial device. Previous attempts to collect and measure transdermal glucose (TG) were based on diaphoretics or external forces to enhance the excretion of glucose through the skin. The closest success among these, reaching Food and Drug Administration approval, is the Cygnus Glucowatch™.17,18 This device extracted glucose across skin by iontophoresis, but the device never made it to market. Another TG monitor developed by Echo Therapeutics Inc. uses a “skin preparer” to abrade the stratum corneum (SC) for access by a glucose oxidase sensor. 19 This is clearly not applicable to neonates or very young children. Other workers have looked at ultrasound20,21 and chemical skin disrupters as well as application of adhesive tape to peel off the SC 22 to increase the amount of glucose extracted through the skin. In contrast, the method for noninvasive TG monitoring described in this article is simply based on collecting the glucose that passively diffuses through skin by gently washing the skin with water.
Our earliest design for collecting passively diffusing TG is a buffer-moistened swab. To test whether glucose on the skin's surface will be absorbed by this swab, cellulose acetate dialysis membrane was used as preterm neonatal skin surrogate. Additionally, this simple model is meant to show that varying the glucose concentrations inside the membrane is reflected in the glucose levels collected on the surface of the membrane. Initial testing of the swab on patients in the neonatal intensive care unit (NICU) proved to be disappointing, probably due to the drying of the outer layer of the swab, which created a barrier to glucose diffusion. This led us to try a more efficient direct sampling procedure based on washing the skin for a set time period and allowing glucose to diffuse. We unexpectedly found that we can pick up traces of glucose even on adult skin. These findings suggest that this method is applicable not only to neonates but also to a broader population of patients.
Methods
The Acrylodan-Labeled Glucose-Binding Protein
The fluorescently labeled GBP used in this study was prepared as described previously.1–4 Before analyzing the samples, the GBP was calibrated using standard glucose solutions. Standard solutions were prepared by dissolving D-glucose (>99.5% purity) obtained from Sigma-Aldrich (St. Louis, MO) in phosphate-buffered saline (PBS). Volumetric flasks were used to make the stock solution (100 mM) and the following dilutions: 0.5, 1.0, 2.0, 4.0, and 8.0 mM.
The fluorescently labeled GBP has micromolar sensitivity to glucose, and its accuracy has been previously validated by high-performance anion-exchange chromatography (HPAEC) with pulsed electrochemical detection (PED) for sugar analysis. 3 For micromolar glucose analysis, GBP has a similar accuracy with a much faster response (less than a few seconds versus ∼20 min).
The Test Vessel and Sampling Swabs
To test the feasibility of collecting glucose on the external surface of a semipermeable membrane, we designed an appropriate test vessel as shown in
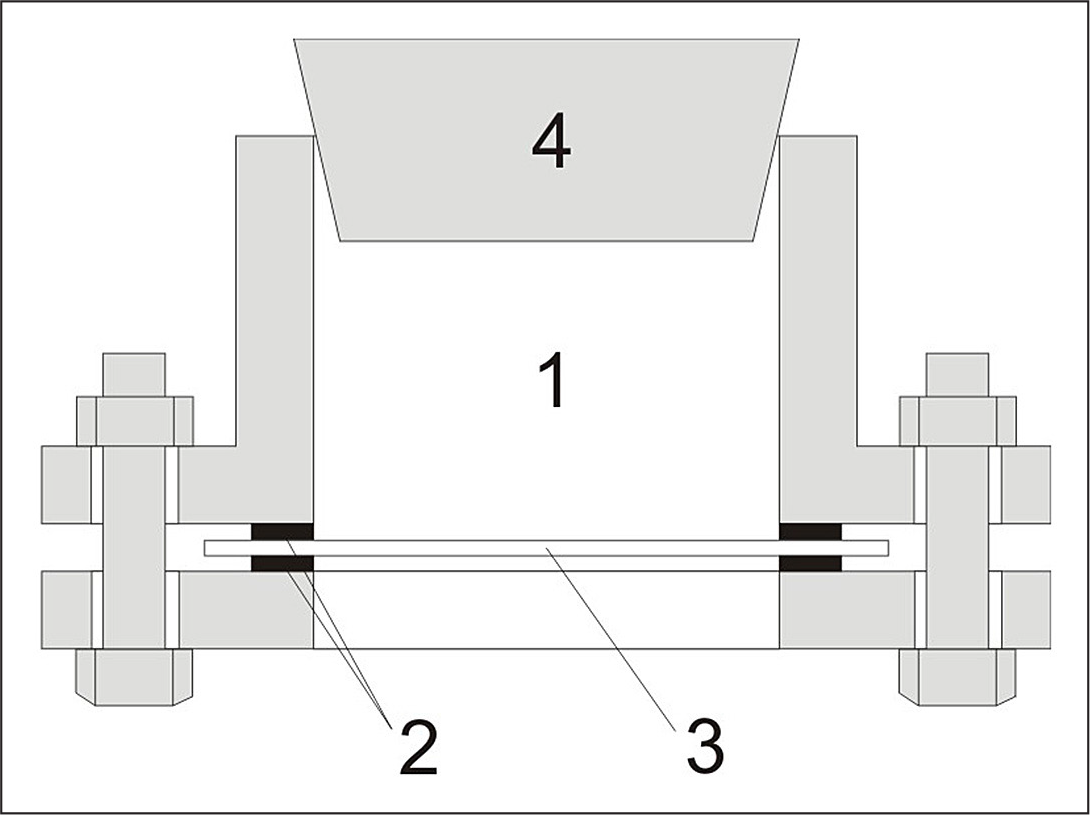
The structure of the test vessel: (1) chamber, (2) O ring, (3) dialysis membrane, and (4) rubber stopper.
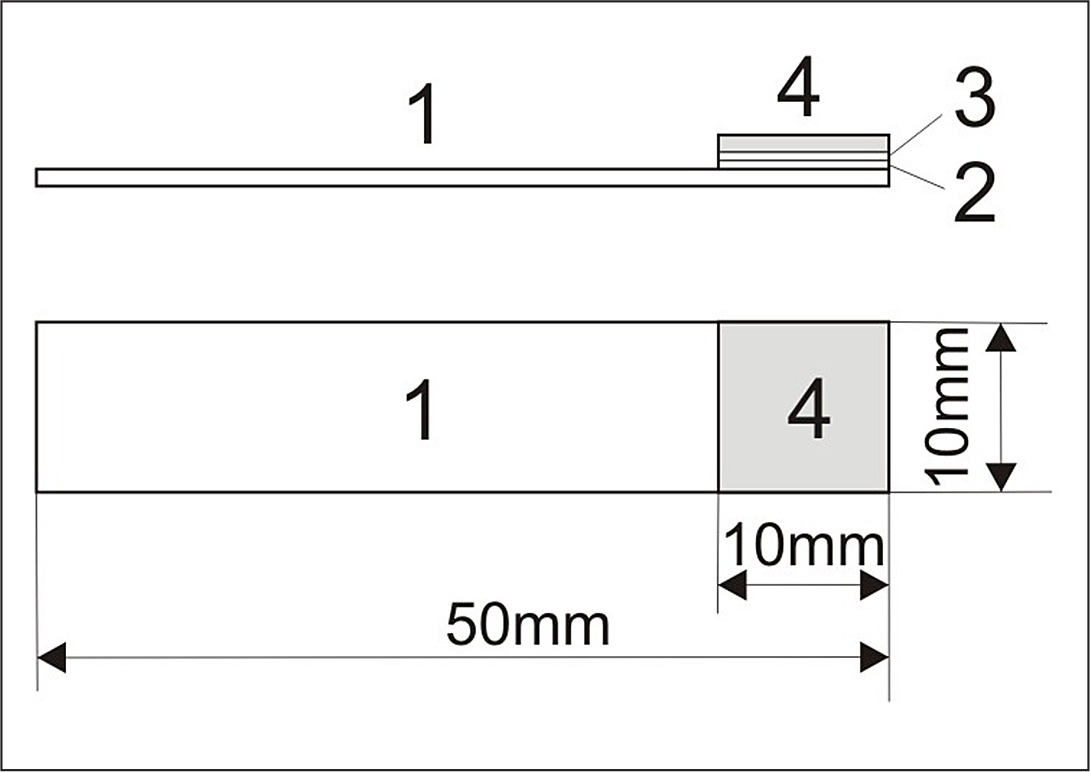
The structure of the sampling swab: (1) polyester transparency film, (2) adhesive, (3) polyethylene, and (4) Whatman chromatography paper.
Swab Sampling Procedure
The surface of the membrane in
Direct Sampling Procedure
The skin surface was first washed with soap and thoroughly rinsed with deionized water. The water on the surface was removed with glucose-free absorbent material, and the surface was allowed to dry at room temperature. To delineate the sampling area, a 1 cm2 plastic ring was placed onto the skin surface and held in place by a finger. We introduced 125 μl of PBS buffer on the skin surface, being careful to keep it within the area of the ring. The buffer was pipetted up and down for 5 min to thoroughly wet and “wash” the surface. The buffer was then withdrawn and transferred to a 1.5 ml plastic vial.
Transepidermal Water Loss Measurement
The TEWL values were measured by a Delfin Vapometer (Delfin Technologies, Finland) as instructed.
Fluorescence Measurement Procedure
Fluorescence intensities were measured on a Varian Cary Eclipse Fluorescence Spectrophotometer (Varian Instruments, Walnut Creek, CA). A total of 250 μl of GBP solution (∼1.5 μM) was added to a 1.5 ml quartz cuvette, and the fluorescence was measured 20 times consecutively. Then 50.0 μl of glucose solution was added. After the mixture was gently vortexed for 10 s, the cuvette was then placed on the spectrophotometer and the fluorescence was again measured 20 times. The average fluorescence intensity before and after adding the glucose sample was calculated, and the signal change was obtained. The assay was performed in triplicate for each solution. All measurements were made at the same instrumental conditions: excitation wavelength 380 nm, emission wavelength 510 nm, excitation slit width 5 nm, emission slit width 5 nm, photomultiplier-tube detector voltage 900 V, and average time 0.1 s.
High-Performance Anion-Exchange Chromatography and Pulsed Electrochemical Detection
A DX-500 microbore liquid chromatography system (Dionex Corporation, Sunnyvale, CA) with a Dionex Model ED40 electrochemical cell and pulsed electrochemical detector was used to measure glucose in the sample solutions. The electrochemical detector was equipped with an gold electrode, a combination pH and Ag/AgCl reference electrode, and a titanium auxiliary electrode. Separation was achieved using a DionexCarboPac PA10 guard and PA10 2 × 250 mm2 analytical column. The mobile phase was 0.150 M NaOH, which was obtained by mixing 0.200 M NaOH (75%) and deionized water (25%), and delivered isocratically. All solvents were degassed and kept under pressure (N2, approximately 10 psi). Samples were introduced by an AS3500 autosampler (Spectra-Physics, Mountain View, CA) onto an injection valve (Model 9010, Rheodyne Inc., Cotati, CA) fitted with a 25 μl injection loop. Glucose was analyzed using a pulsed potential waveform controlled by Peaknet software (Dionex, version 5.21). Under the experimental conditions, glucose elutes in 4.1 min. Samples were run in triplicate, and the glucose concentration in the solution was quantified by using peak area data from the chromatogram.
Results and Discussions
The GBP used in this study has a single cysteine mutation at 255 where the polarity-sensitive probe acrylodan is covalently attached. The labeled acrylodan emits strong green fluorescence (510 nm) when excited with violet light (380 nm). In the presence of glucose, the fluorescence intensity of acrylodan decreases with glucose concentration. The signal change is defined as (F0 – F)/F0, where F0 and F are the fluorescence intensity of GBP in the absence and presence of glucose, respectively. A typical calibration curve of the glucose biosensor is shown in
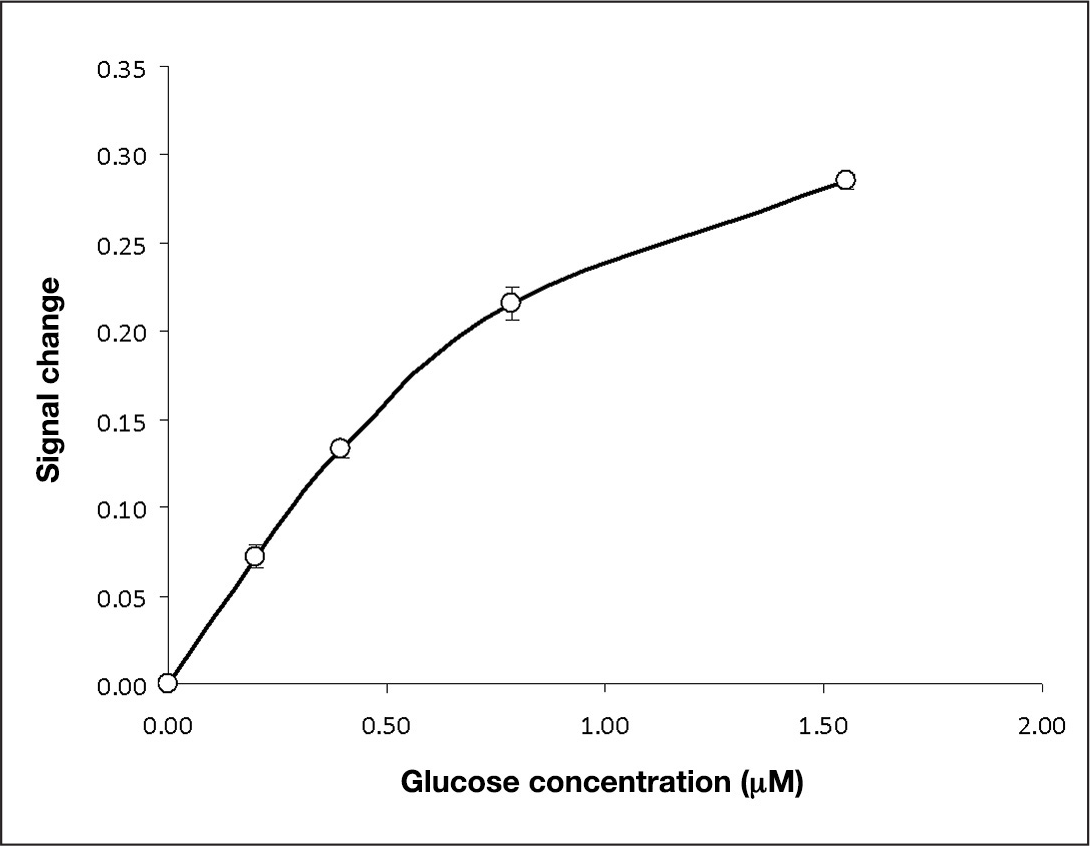
The calibration curve for the acrylodan-labeled GBP. The error bars are the standard deviation of three repeated assays.
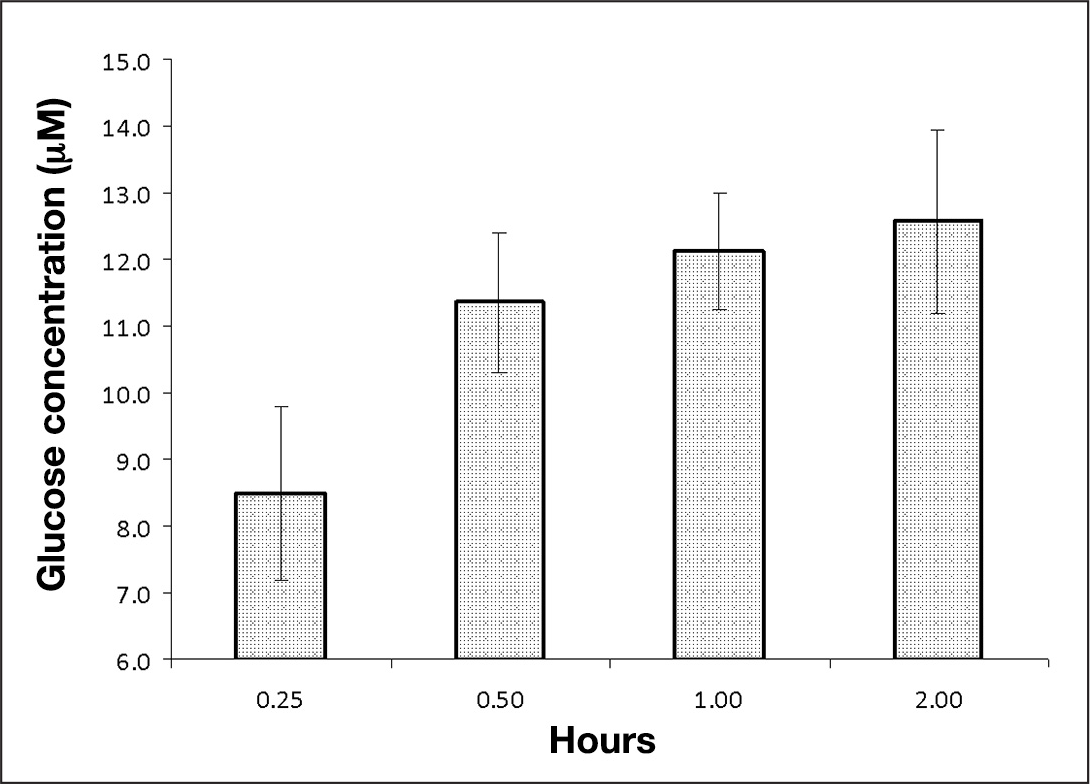
Effect of lapse time after surface rinsing on the glucose concentration in the collected sample. The error bars are the standard deviation of three different samples. The glucose concentration in the chamber is 5.0 mM, and the sampling time is 60 s.
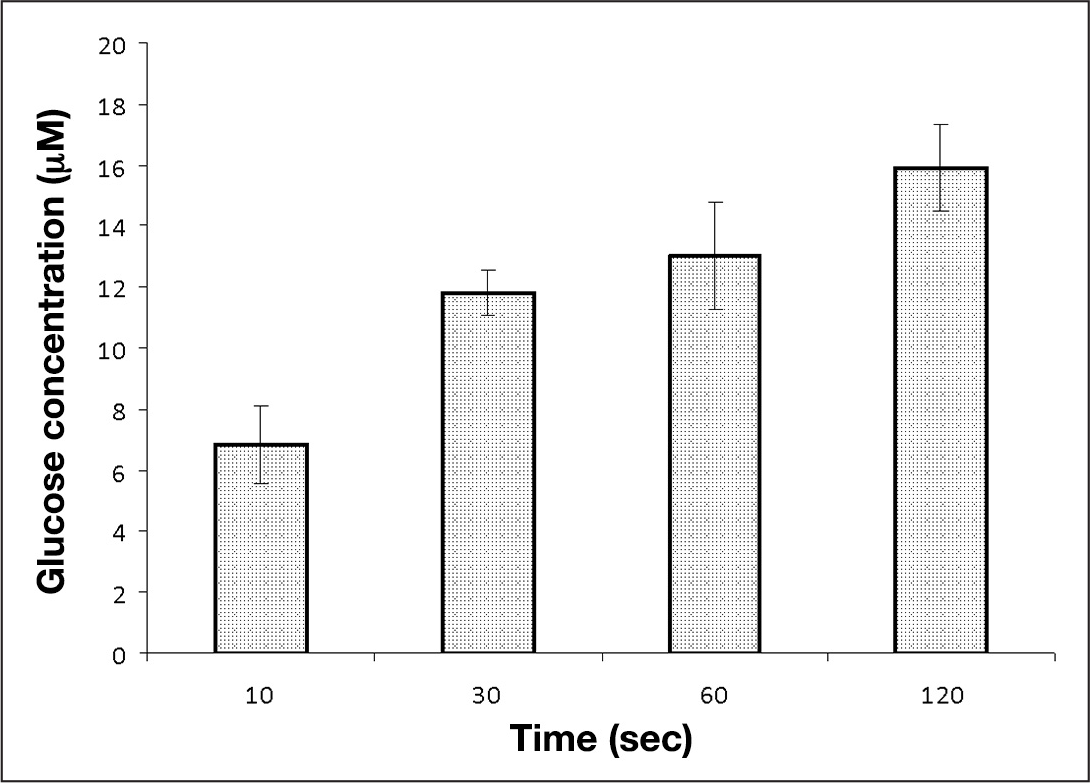
Effect of swab dwell time on the glucose concentration in the collected samples. The error bars are the standard deviation of three different samples. The glucose concentration in the chamber is 5.0 mM, and the samples are collected 30 min after surface rinsing.
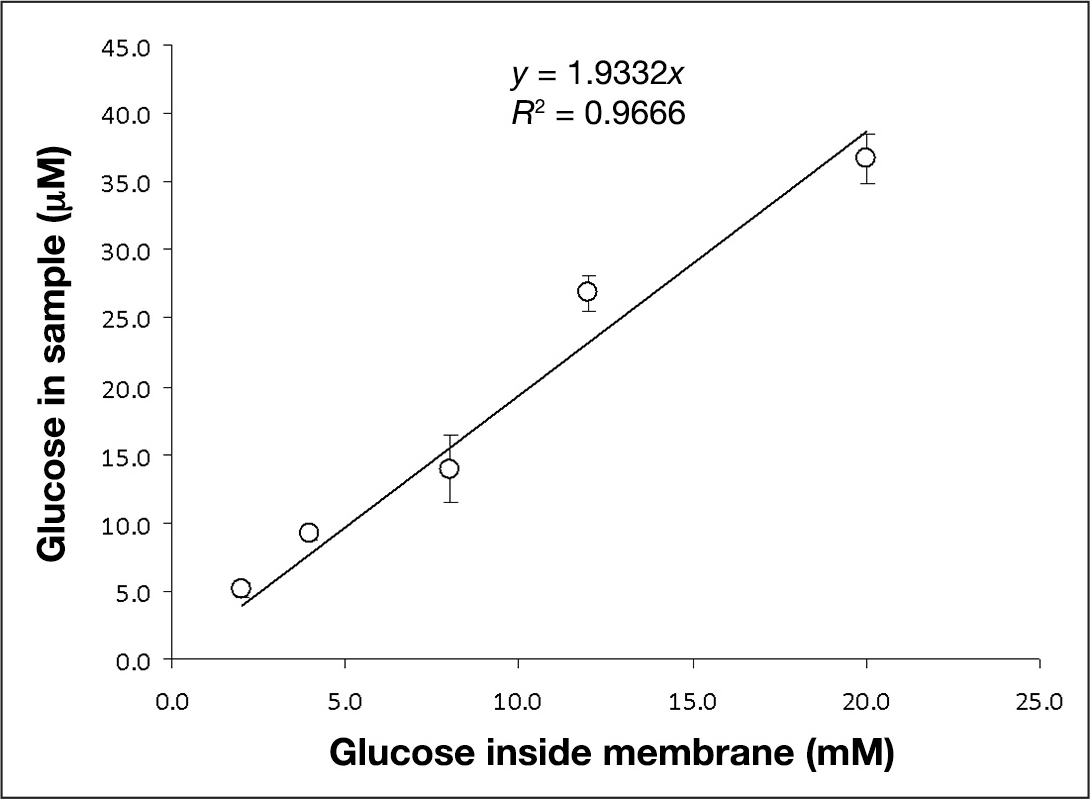
Relationship between the glucose concentration in the sample and the glucose concentration in the test vessel. The error bars are the standard deviation of three different samples. The samples are collected 30 min after surface rinsing, and the sampling time is 30 s.
We hypothesized that the underdeveloped skin of the neonate should behave like the semipermeable membrane, which we chose based on the same rate of water loss of 59 g/m2/h. To test this hypothesis, we collected some samples from the skin surface of neonates in the NICU using the swab sampling procedure. It was found that the glucose concentrations in the samples collected by the swab were too low to be detectable. It is possible that, from the time the buffered saline was added to the filter paper to the time the swab was applied on the baby, the outer layer of paper dries and becomes a barrier to glucose diffusion. Indeed, we found that the swab could collect only part of the glucose on the surface. Conversely, only a fraction of the glucose that manages to diffuse to the filter paper is released to the wash buffer prior to analysis. We observed this when serum of known glucose concentration was directly applied to the swab. Approximately 50% of the glucose remains in the swab, and approximately 50% is available for analysis. Thus the swab turned out to be a poor vehicle for collection of skin glucose. Consequently, the swab was completely eliminated for sampling. Instead, buffered saline was directly applied on the skin, circulated for a period of time, collected, and analyzed.
Up to this point, the results on the cellulose acetate semipermeable membrane support the idea that the glucose that diffused on the surface of the membrane is directly proportional to glucose inside the membrane. However, human skin is of a more heterogeneous composition than a simple inanimate membrane. Human epidermis is composed of the basal layer, keratinocytes, and an outer SC. The prevailing notion is that the SC consists of hornified cells with no interstitial fluid and, thus, is presumed to be of little value to TG sensor development. 24 In reality, the SC is involved in dynamic processes. 25 It is also assumed that the highly hydrophilic glucose molecule present in the interstitial fluid cannot penetrate through the dermis and the adipose tissues beneath the epidermis. Without some kind of chemical or physical enhancement, the general belief was that sufficient surface collection of glucose is not possible. 26 With all these caveats, we nevertheless decided to test direct sampling of the skin on an adult, primarily because neonates are not as accessible for immediate testing.
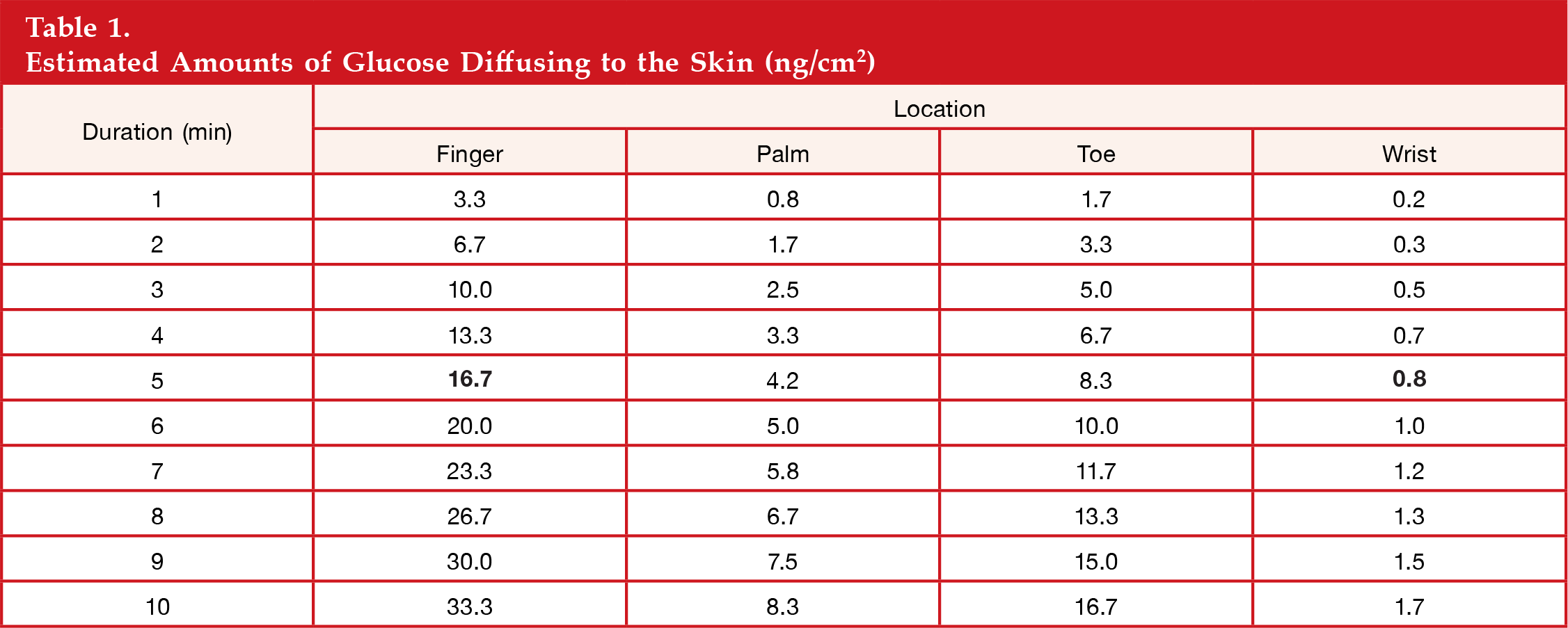
First we measured the total TEWL at different sites on the body. The highest TEWL was at the tip of the fingers (∼200) and lowest on the belly (∼10). Based on the TEWL rates, we estimated the glucose concentrations in samples for 125 μl water to wash 1 cm2 skin. The calculated results are shown in
Estimated Amounts of Glucose Diffusing to the Skin (ng/cm2)
Measured Amounts of Glucose on the Skin (ng/cm2) a

The duration of the collection is 5 min.
The ratio of the amount of glucose collected at site 1 to that collected at site 2.
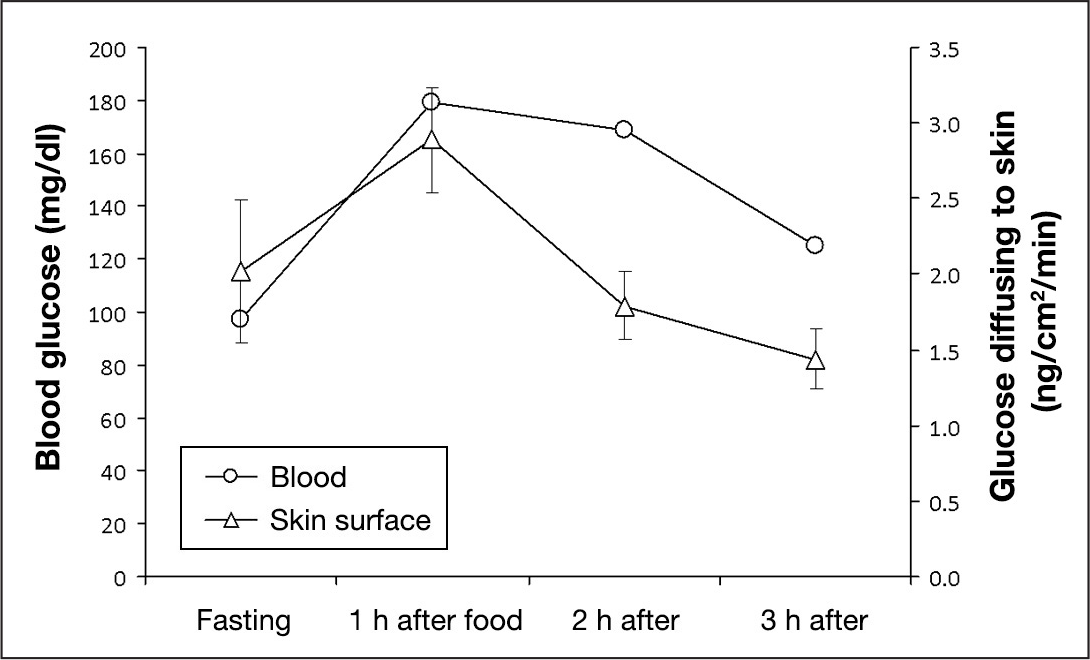
Next, we collected some samples from the skin surface of an adult before food intake and 1, 2, and 3 h after food intake. At the same time, blood glucose concentrations were measured with a Precision Xtra glucometer produced by Abbott (Alameda, CA).
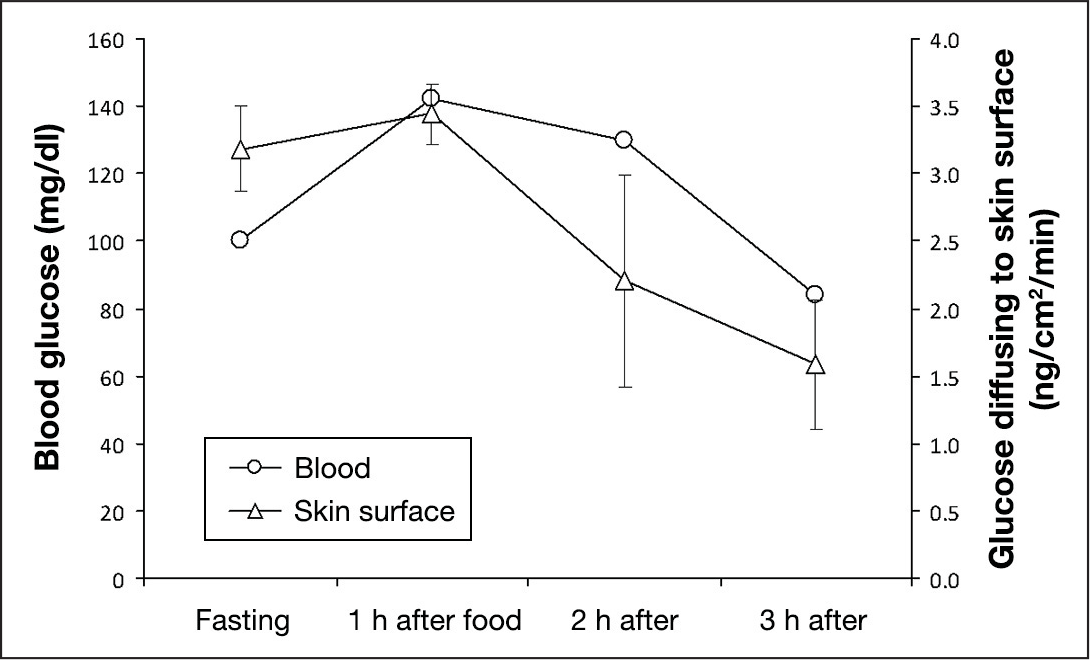
The amounts of glucose diffusing to the skin surface measured by GBP versus the blood glucose concentrations. The error bars are the standard deviations of three repeated assays.
Note that the amount of glucose diffusing to the adult's skin surface is 1.6∼3.2 ng/cm2/min. Such trace amounts of glucose cannot be measured with the conventional glucose-oxidase-based sensor. An extremely sensitive glucose sensor such as the GBP (Kd = 0.4–1.2 μm) is required. 2 Another interesting observation is that the glucose diffusion rate through the skin is much slower than through the semipermeable membrane, even when the latter has a similar water loss rate as the skin. This means that, although water loss rate is related to the glucose diffusion rate, it is only one of the many factors affecting the glucose diffusion rate. These factors include pore size and distribution, thicknesses of the dermis and epidermis, and vascularity of the subcutaneous layer, which will require more in-depth study of skin physiology beyond this article.
To verify that the GBP results can be duplicated using a standard analytical method, we repeated the sampling procedure and analyzed the collected TG samples using HPAEC-PED.
The amounts of glucose diffusing to the skin surface measured by HPAEC and PED versus the blood glucose concentrations. The error bars are the standard deviations of three repeated assays.
Conclusions
We showed that trace amounts of glucose that passively diffuse to the surface of a semipermeable membrane can be collected with a simple moistened swab or by direct sampling procedure. Measurements of the trace glucose levels are made possible with the highly sensitive fluorescent GBP and verified by the standard high-performance liquid chromatography method. The glucose concentration on the surface increases with the time after surface cleaning but gradually levels off. The sampling time also affects the glucose concentration in the sample collected. At a fixed lapse time after surface cleaning and a fixed sampling time, the glucose concentration in the collected sample is linearly proportional to the glucose concentration in the chamber. Because the skin is a semipermeable membrane, it is expected to behave somewhat similarly as the surrogate membrane. The TEWL of skin at various parts of the body correlates with glucose collected. Preliminary studies on adult skin before and after a meal showed that the amount of glucose diffusing to the surface of human skin follows changes in blood glucose. Note that this procedure samples the passive diffusion of glucose through the SC, and no external force (e.g., iontophoresis or ultrasound) was employed. One can argue that bathing the skin surface with buffer softens the hornified cells on the SC and induces diffusion through the concentration gradient. Nevertheless, the process is no harsher than washing the skin with water and should not produce adverse effects on the skin surface.
Automation, standardization and further optimization of the sampling device are now being undertaken and should lead to a novel, noninvasive method of glucose monitoring. Additionally, larger population studies are currently being conducted for noninvasive blood glucose monitoring using the direct sampling procedure versus YSI.
Footnotes
Abbreviations:
This work was supported by National Institutes of Health Grant #1R41HD06920701.
Acknowledgments:
We thank Ms. Karuna Sri Mupparapu for the preparation of the GBP, Mr. Michael Tolosa for fabrication of the experimental chamber, and Dr. William La Course for the use of the HPAEC-PED. We dedicate this article to Dr. Freeman Hrabowski, University of Maryland, Baltimore County, president, on his 20-year anniversary as a transformational leader in higher education.