
Abstract
Introduction
The distribution of adipose tissue and fibrosis in the heart is important because of its associations with cardiovascular conditions. However, research on the specific locations of adipocytes and fibrosis across the four cardiac chambers of the heart remains limited. Our study aimed to quantify the distribution of adipocytes and fibrosis across the four chambers of the human heart and to relate these structural findings to the causes of death in the post-mortem cases.
Materials and Methods
As part of routine cardiac examination, images of Masson Trichrome-stained transverse myocardial slices from each of the four chambers of the heart of 52 post-mortem cases were analysed for adipocyte, fibrosis and cardiomyocyte area.
Results
The greatest adipocyte area was observed in the right atrium (∼45%), with both the right atrium and left atrium having the greatest fibrosis formation (∼20-23%), whereas the right ventricle (8%) had substantially more adipocytes compared to the left ventricle (∼0.6%), but rather similar levels of fibrosis (∼3-4%). The post-mortem cases that were diagnosed with a cardiac cause of death had greater adipocyte area and less cardiomyocyte area in the left ventricle compared to cases without a cardiac cause of death.
Discussion and Conclusion
Our descriptive study suggests that adipocyte and fibrosis distribution are clearly different in the four chambers of the heart, and that the location might be important for the development of cardiovascular diseases and potential cardiac death.
INTRODUCTION
The adipose tissue in the heart plays a crucial role in various physiological functions ((1)). Heart fat can be present on the outside of the heart surface as epicardial adipose tissue, surrounding the coronary vessels as perivascular adipose tissue, and within the myocardium as intramyocardial adipose tissue. In conditions like obesity and type 2 diabetes, the amount of heart fat can significantly increase, sometimes accounting for up to 50% of total heart mass in severe cases ((2)). This excess fat is linked to various cardiovascular diseases ((2,3)), and intramyocardial adipose infiltration might disrupt the connectivity between cardiomyocytes ((4)), which potentially leads to increasing conduction heterogeneity ((5,6)).
The distribution of adipose tissue within the heart might be important, particularly regarding its associations with cardiovascular conditions. Selthofer-Relatić et al (2018) observed greater adipose deposition in the right ventricle (RV) compared to the right atrium (RA) in male postmortem cases ((7)). Others reported greater adipose tissue in the RV compared to the left ventricle (LV) in patients without cardiac disease ((8,9)). Unlike overall adipose tissue distribution, research on the specific locations of adipocytes across the four heart chambers remains limited. Furthermore, the association of the adipose tissue distribution in the heart with causes of death (non-cardiac vs cardiac) has not been assessed.
Heart fat has also been associated with cardiac fibrosis. For instance, epicardial adipose tissue has been found to secrete pro-fibrotic adipokines ((10)), while intramyocardial adipose within the atrial myocardium has been shown to trigger fibrosis in experimental models ((3)). This suggests a potential association between adipose deposition and fibrosis formation. Interestingly, fibrosis is also not uniformly distributed within the heart. In canines, Burstein et al (2008) demonstrated that atrial fibroblasts exhibit a more reactive and pronounced fibrotic response compared to ventricular fibroblasts ((11)). Whether a similar chamber-specificity exists for fibrotic deposition in the human heart is unknown.
Our study aimed to provide a quantitative snapshot of the distribution of adipocytes and fibrosis across the four chambers of the heart in post-mortem cases. Additionally, we aimed to relate our structural findings to the anthropometric data, as well as the causes of death in the post-mortem cases.
METHODS AND MATERIALS
Post-Mortem Cases
Heart tissue images from post-mortem cases were collected during a six-month prospective study. This study involved routine coronial post-mortem examinations conducted between November 2019 and April 2021, which have been studied previously ((12–16)). Paediatric cases (younger than 18 years of age) were excluded from the study, as were cases with a suspicious cause of death, or those where the body was severely decomposed, malnourished, or cachectic. The total post-mortem cases for this study, where all four heart chamber images were available, included N = 52 cases.
Most of the information collected for these cases included age, sex, ethnicity, body weight, and body height. This data allowed for the calculation of body mass index (BMI), which is determined by body weight [kg]/body height [m]2), and body surface area (BSA) using the DuBois method: 0.007184 × (body height [cm]0.725 × body weight [kg]0.425). Available and additional information included the cause of death as recorded by the coroner and the dissected heart weight.
Heart Weight
A forensic pathologist removed the hearts for routine examination in accordance with standard procedures ((17,18)). In brief, to measure the weight of the dissected hearts, the great vessels were cut approximately 30 mm above the semilunar valve, and the pulmonary veins were severed at the pericardial reflection. This allowed for the heart to be removed from the pericardial sac, in accordance with American and European guidelines. The vena cavae were cut at the diaphragm and about 20 mm above the point where the superior vena cava meets the atrial appendage. The short-axis method was employed for the dissection of the heart. Blood and blood clots were removed from the heart chambers, and the heart was patted dry before weighing. An SW15KM digital scale, with a 5 g margin of error, was used to measure the weight of the dissected heart (A & D Company Ltd, Tokyo, Japan).
Heart Tissue Procurement and Processing
After weighing, a forensic pathologist fixed the dissected hearts in 10% formaldehyde. As part of routine coronial post-mortem cardiac examination, a standardised transverse myocardial slice was obtained from each chamber of the heart (left atrium (LA), RA, LV, RV) at the mid-level of the chamber. The heart tissue was embedded and sectioned (4 µm), and was stained for Masson Trichrome, colouring the cardiomyocytes red, fibrosis blue, and adipocytes and background area white. The tissues on the slides were dewaxed, hydrated, and treated with Bouin's fixative for 1 h at 60 °C in an oven and cooled for 10 min. The slides were then washed and put into the automatic multi-stainer and stained sequentially with Weigert's Haematoxylin and Biebrich Scarlet-Acid Fuschsin for 10 min. Samples were then differentiated in Phosphomolybdic/Phosphotungstic acid for 15 min, counter-stained in Aniline blue for 6 min, and differentiated in 1% acetic acid for three minutes. In each step of staining, differentiating, and counterstaining, the slides are washed in water. Finally, the slides were dehydrated, cleared and mounted.
Following staining, the slides were viewed on an Olympus BX53 microscope (Olympus, Japan) using a UPlanFL N 4× objective lens. One digital image was taken of each sample using either an Olympus UC50 digital camera (Olympus, Japan) or an AmScope HD1080A digital camera (AmScope, United States). Heart tissue images (either TIFF or JPEG format) were then transferred to the laboratory for digital image analysis.
Image Analysis and Unit Conversion
The analysis of fibrosis and cardiomyocyte areas was conducted for all four chambers of the heart using Affinity Photo (version 2.6). A live hue mask was applied to the original image, and the output inverter was used to ensure that all blue hues were selected for fibrosis and all red hues for cardiomyocytes. The modified image was then exported to ImageJ (version 1.54), where a colour threshold was applied to the relevant pixels in a binary image. This final image was analysed to determine the area and the area fraction of the selected pixels. Similarly, the adipocyte area was analysed using the images from ImageJ. All visible, white-coloured, round-shaped adipocytes were manually circled using the lasso tool and added to the region of interest (ROI) manager, per image and summed, ensuring that any white processing artefacts or striations were excluded.
All data measured in pixels were converted to μm2 based on the image type and size, using either 5072480 for TIFF images or 5007744 for JPEG images. Each image represented an area of 10.5 mm2, corresponding to the total pixel count. The pixel count for each image was converted to area in μm2 by multiplying by 2.06999 for TIFF images or 2.09675 for JPEG images. While heart tissue images for all four chambers were collected from the 52 cases included in the study, some images had to be excluded due to issues such as blurriness, excessive saturation, or incorrect magnification. The actual number of images analysed is provided in the figure legends or corresponding text in the Results section.
Statistical Analysis
All statistical analysis was done using GraphPad Prism (version 10.0.0, GraphPad Software Inc., USA). Where appropriate, all continuous data are presented as mean or median values with range, and all categorical data are presented as numbers with percentages. The normality of distribution was determined using the Shapiro-Wilk test. Potential outlier values were determined by robust regression and outlier removal (ROUT) analysis (Q = 1%). Differences between the two groups of data were determined using unpaired t-tests, Mann-Whitney U tests, or Fisher's exact tests according to data normality. Differences between more than three groups were determined using one-way analysis of variance (ANOVA). Simple linear regression analyses of raw, untransformed data assessed associations between variables. P < 0.05 was considered statistically significant for all analyses.
RESULTS
Post-Mortem Cohort Characteristics
The key anthropometric characteristics, the heart weights, and the adipocyte, fibrosis and cardiomyocyte areas for the total 52 post-mortem cases are shown in
The Anthropometric Characteristics, the Heart Weights and the Adipocyte, Fibrosis and Cardiomyocyte Areas for the Total Post-Mortem Case Cohort.

Data is presented as mean or median value with range (continuous variables) depending on the normality of distribution or number with percentage (categorical variables). BMI body mass index, BSA body surface area, RA right atrium, LA left atrium, RV right ventricle, LV left ventricle.
Adipocyte, Fibrosis and Cardiomyocyte Areas
Examples of the Masson Trichrome-stained images of the four chambers of the heart are shown in

Examples of images of the four chambers of the heart (case 20F0815). (A) right atrium (B) left atrium (C) right ventricle (D) left ventricle. The tissue was Masson Trichrome stained, resulting in cardiomyocytes colouring red, fibrosis blue, and adipocytes and processing artefacts white. 4× objective lens, bar is 1 mm.

Adipocytes in the different chambers of the heart. The adipocyte area was greater in the atria compared to the ventricles (A) and greater on the right compared to the left side of the heart (B), whereas the adipocyte area in the four chambers of the heart was significantly different from each other (C), except for the LA and RV. The data in panels A and B were tested with a Mann–Whitney test, whereas for panel C, a one-way ANOVA Kruskal–Wallis test was used. Data are mean ± SD with P < 0.05 considered significant; *** P < 0.001, **** P < 0.0001 ns = non-Significant. RA, right atrium (N = 48); LA, left atrium (N = 46); RV, right ventricle (N = 46); LV, left ventricle (N = 49).
Fibrosis was significantly greater in the atria compared to the ventricles (
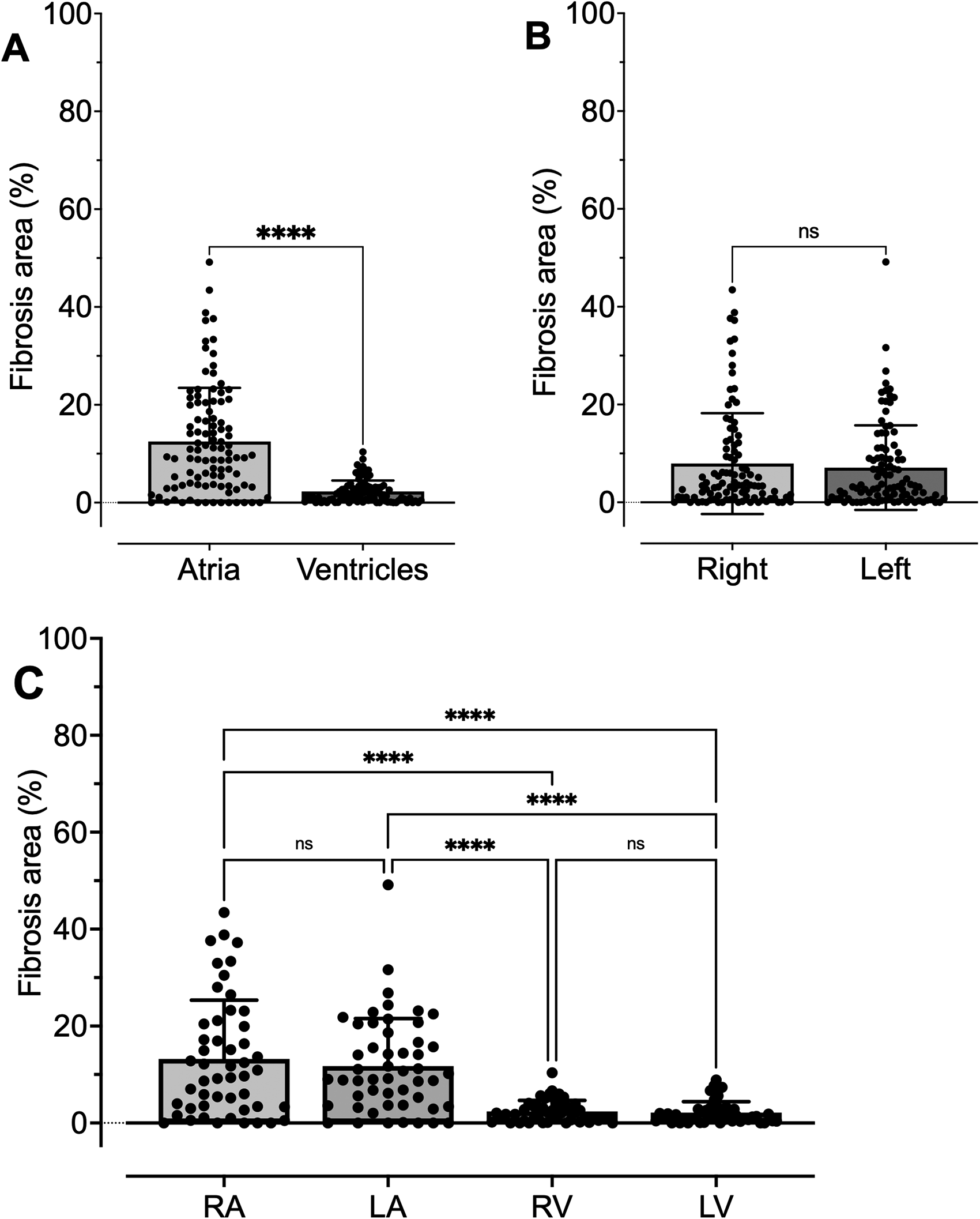
Fibrosis in the different chambers of the heart. Fibrosis area was greater in the atria compared to the ventricles (A), but did not differ between the right and the left side of the heart (B). This was confirmed when fibrosis was analysed in the four individual chambers of the heart (C). The data in panels A and B were tested with a Mann–Whitney test, whereas for panel C, a one-way ANOVA Kruskal–Wallis test was used. Data are mean ± SD with P < 0.05 considered significant; **** P < 0.0001, ns = non-Significant. RA, right atrium (N = 50); LA, left atrium (N = 51); RV, right ventricle (N = 48); LV, left ventricle (N = 48).
The cardiomyocyte area was significantly greater in the ventricles compared to the atria (
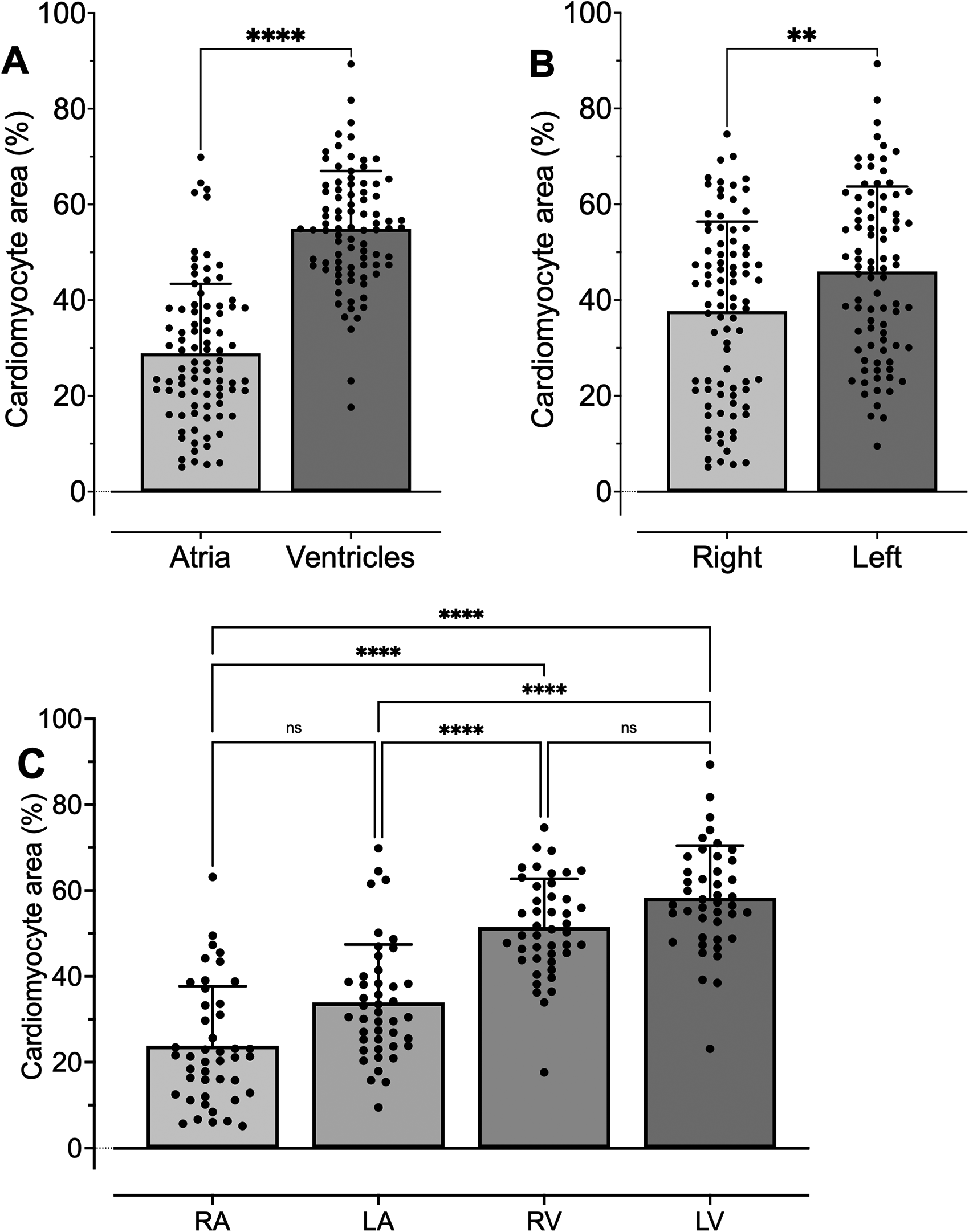
Cardiomyocytes in the different chambers of the heart. The cardiomyocyte area was greater in the ventricles compared to the atria (A) and greater on the left compared to the right side of the heart (B), whereas the cardiomyocyte area in the four chambers of the heart was significantly different from each other (C), except for the RA and LA and the RV and LV. The data in panels A and B were tested with a Mann–Whitney test, whereas for panel C, a one-way ANOVA Kruskal–Wallis test was used. Data are mean ± SD with P < 0.05 considered significant; ** P < 0.01, **** P < 0.0001, ns = non-significant. RA, right atrium (N = 44); LA, left atrium (N = 44); RV, right ventricle (N = 44); LV, left ventricle (N = 43).
Associations of Anthropometrics with Adipocyte, Fibrosis and Cardiomyocyte Area
Simple linear regression identified associations between the anthropometric characteristics and the areas of adipocytes, fibrosis and cardiomyocytes. LA cardiomyocyte area was negatively associated with age (
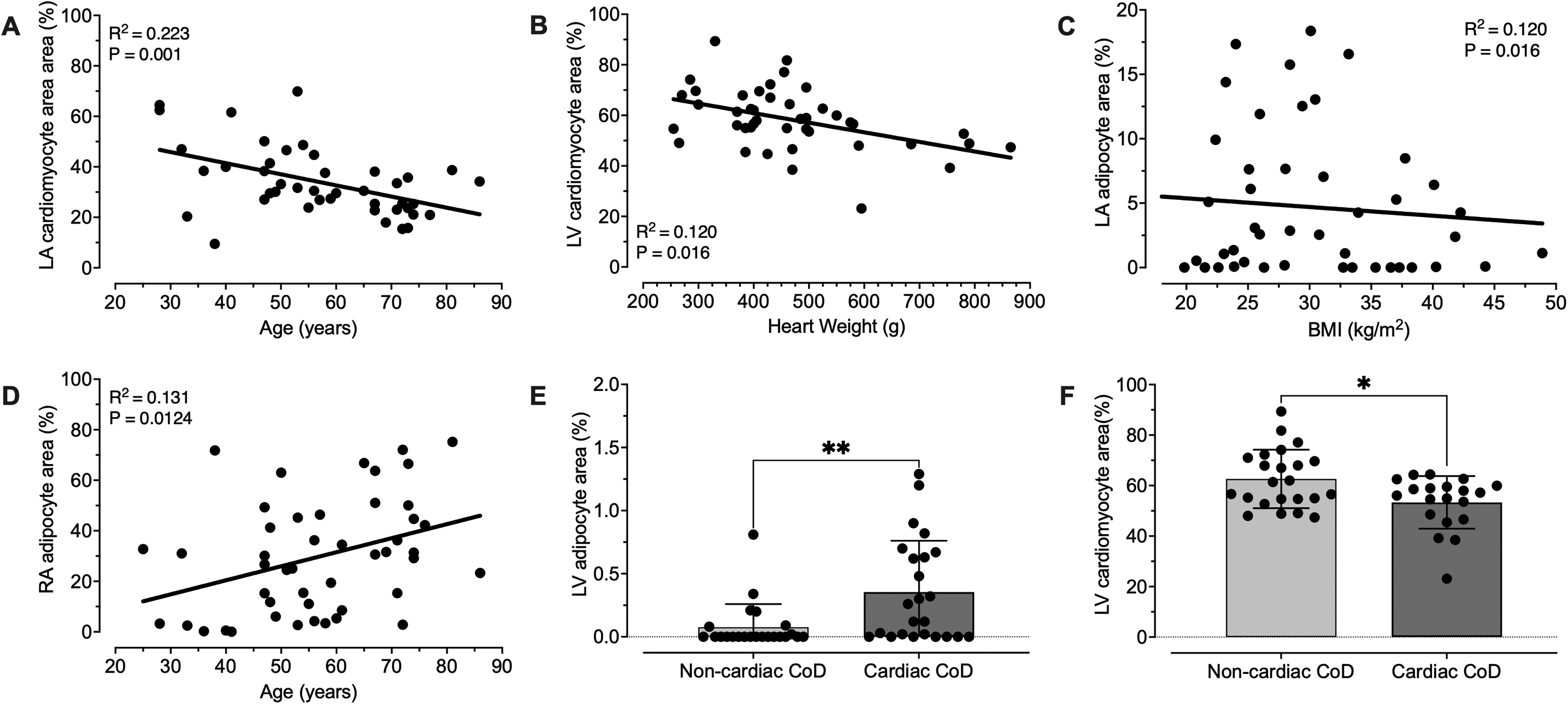
Anthropometric associations and cause of death with adipocyte, fibrosis and cardiomyocyte areas. (A) Left atrial (LA) cardiomyocyte area was negatively associated with age (N = 51), and (B) left ventricular (LV) cardiomyocyte area with heart weight (N = 52). (C) LA adipocyte area was negatively associated with body mass index (BMI; N = 52), and (D) right atrial (RA) adipocyte area was positively associated with age (N = 52). (E) LV adipocyte area was greater in post-mortem cases with a cardiac cause of death (CoD, N = 25) compared to non-cardiac CoD (N = 27), whereas (F) the LV cardiomyocyte area was less in the cardiac CoD group. Simple linear regression was used to determine associations (A–D). Data in panels E–F were tested with a Mann–Whitney test, with data mean ± SD, and P < 0.05 considered significant; * P < 0.05, ** P < 0.01.
Simple Linear Regression Analyses of Anthropometric Characteristics and the Adipocyte, Fibrosis and Cardiomyocyte Areas for the Total Post-Mortem Cohort.

The continuous variables (age, body mass index (BMI), body surface area (BSA) and heart weight were analysed via simple linear regression. The categorical variables, sex (female/male), diabetes (yes/no) and cause of death (non-cardiac/cardiac), were tested with the Mann-Whitney test. RA, right atrium; LA, left atrium; RV, right ventricle; LV, left ventricle. P < 0.05 is considered significant and is made
DISCUSSION
The main findings of our study are that in our post-mortem cohort the relative greatest adipocyte area was observed in the RA (∼45%), with both the RA and LA having the relative greatest fibrosis formation (∼20-23%), whereas the RV (8%) had substantially more adipocytes compared to the LV (∼0.6%), but rather similar fibrosis (∼3-4%). We have summarised these main findings in Figure 6. In addition, our study found that the adipocyte area was greater, and the cardiomyocyte area was less, in the LV of the post-mortem cases diagnosed with a cardiac cause of death (Figure 5E-F). Thus, adipocytes and fibrosis distribution are clearly different in the four chambers of the heart, and the location might be important for the development of cardiovascular diseases and potential cardiac death. Our descriptive study provides a quantitative snapshot on adipocytes and fibrosis distribution in the heart and can, in the future, be an important starting point for potentially larger, more detailed studies.

Adipose Tissue in the Heart
In our study, we observed that the amount of adipose tissue was more pronounced on the right side of the heart compared to the left side, affecting both the atria and ventricles. This finding aligns with previous studies investigating myocardial adipose distribution in the right and left ventricles ((8,9)). Furthermore, we found that the amount of adipose tissue was significantly greater in the atria than in the ventricles on both the right and left sides of the heart. This contrasts with the findings of Selthofer-Relatić et al (2018), who reported greater adipose distribution in the RV free wall compared to the RA ((7)). Notably, their RV fat percentage (7.5%) closely resembled our findings (8%), while their observation for RA fat (4.5%) was considerably lower than our results (45.1%). However, it is essential to note that their study included only 10 male postmortem cases, all of which had non-cardiac causes of death ((7)). On a critical note, the standard approach for coroner investigations involves taking a mid-transversal section through the four chambers of the heart, and unfortunately, this method does not allow for the assessment of adipocytes in different parts of each chamber. This might be significant because previous studies have suggested that adipose deposition is more pronounced in the apex or near the outflow tracts of the ventricles rather than in the free wall ((7,9,19–21)). Since this is a descriptive study, the underlying causes for the relatively large variations in adipose tissue across the four chambers of the heart remain speculative. Possible causes might relate to the different transmural pressures within the chambers and the concomitant variations in metabolic demands. Additionally, the observed chamber-specific adipose distribution raises questions about whether the adipocytes in the various chambers have distinct morphologies or physiological characteristics. This notion was already suggested several decades ago ((8)), and we recently demonstrated that sex differences in cell morphology of adipocytes in the heart exist ((14)), and that adipocyte hypertrophy, which normally facilitates the expansion of fat tissue during obesity, does not seem to occur in epicardial adipose tissue ((12,22)).
Fibrosis and Cardiomyocytes in the Heart
Distinct patterns of fibrosis are present throughout the myocardium ((23)). Our findings indicated that fibrosis was more pronounced in the atria than in the ventricles, which aligns with earlier studies conducted in canines ((24)). Research has shown that atrial fibroblasts display a more reactive and significant fibrotic response compared to ventricular fibroblasts in canines ((11)). Additionally, recent proteomic data from human hearts support the notion that different gene expression profiles and functions exist in the various chambers of the heart in relation to fibroblasts and extracellular matrix formation ((25–27)).
Our observation of a larger area of cardiomyocytes in the ventricles compared to the atria was not unexpected. Litvinukova et al (2020), using single-cell and single-nucleus transcriptomes, revealed that more cardiomyocytes are located in the ventricles than in the atria in the adult human heart ((28)). Similar to adipocytes and fibroblasts, cardiomyocytes might also have distinct morphologies or physiological characteristics in the different chambers of the heart. Bootman et al (2006) demonstrated differences in cardiomyocyte ultrastructure between the atria and ventricles ((29)). Additionally, Bussey et al (2015) showed that the expression of essential calcium-handling proteins differs between the right atrium and left ventricle ((30)). More recently, a quantitative proteomic analysis of the human heart found significant differences in protein expression, with 1220 proteins (13.7%) showing higher expression in the atria and 409 proteins (4.6%) exhibiting higher expression in the ventricles ((25)).
Cause of death
The relatively large areas of adipocytes in the RA (range: 0-75%) and in the LA and RV (range for both: 0-18%) did not show any differences between post-mortem cases with a cardiac cause of death or those without. However, the relatively small adipocyte area in the LV, which ranged from 0–2.5%, was significantly larger in the group of postmortem cases with a cardiac cause of death. Adipose deposition has previously been associated with cardiac death for the RV ((7,20,31–34)), as well as the LV ((35,36)), however, mostly in case reports. The underlying mechanisms of how fat deposits in the ventricles might promote arrhythmogenicity remain speculative but might be caused by the secretion of adipokines or metabolites, which have been shown to induce arrhythmogenic behaviour in human atrial tissue ((37–39)). Why the relatively small amount of fat in the LV seems to be more detrimental compared to the larger amounts of adipocytes in the other chambers of the heart is intriguing. Potential underlying reasons might again relate to the higher transmural pressures, the concomitant increased metabolic demands, or the distinct morphologies and physiological characteristics of adipocytes or cardiomyocytes in the LV, which all warrant further investigations. It is important to note that our study did not differentiate between fat that was infiltrated in the myocardium or that was deposited as a layer on the outside of the chambers, nor did we measure fat deposition within the cardiomyocytes. Unfortunately, these distinctions were technically unfeasible based on the images of the post-mortem cases provided.
Anthropometric Associations
Our analysis of anthropometric data revealed that the area of RA adipocytes increased with age, while the area of LA adipocytes decreased with BMI, though both associations were weak. Additionally, we found that none of the other anthropometric characteristics (such as age, sex, BMI, BSA, diabetes, or heart weight) showed any association with the various adipocyte or fibrosis areas in the heart chambers. Previous studies have indicated that the epicardial fat layer can be influenced by factors like sex ((7,9,21)), age ((9,21)), and BMI ((9)), with larger adipose deposits observed in older individuals, females, or those with a higher BMI. In contrast, some computed tomography (CT) studies reported no significant gender differences in myocardial adipose deposition ((40,41)). Furthermore, fibrosis was also less prevalent in females compared to males in both murine and human studies ((26,42)). Our 2D histological approach, which assessed adipocyte area in only a single plane of the heart chambers, might have contributed to these differing results when compared to more comprehensive and costly volumetric imaging techniques. Moreover, our descriptive study cannot establish causation, which would require intervention studies. However, ethical constraints will make this challenging in human studies, whereas conducting such studies in small rodent models is difficult due to their lack of epicardial adipose tissue ((43)).
Limitations
As part of routine coronial post-mortem cardiac examination, only one standardised transverse myocardial slice was available from each chamber of the heart at mid-level. Although some images displayed perivascular fibrosis, the overall analysis of fibrosis for this study included both myocardial and perivascular fibrosis because differences could not be precisely determined from transverse sections, especially when the section was exactly cut through the fibrosis area without exposing the vessels. Therefore, future research will need to verify how representative our findings in the human heart are by using multiple myocardial sections or potentially more advanced imaging techniques.
Recently, we showed that heart weight can be quite variable within this cohort of post-mortem cases ((16)), which could have affected adipose or fibrosis distribution. However, for this study's cohort, we did not have enough cases to analyse hypertrophied and non-hypertrophied hearts separately. We did not find any associations between adipose or fibrosis distribution and BMI, diabetes or age; however, other potential co-morbidities, such as hypertension, cardiomyopathies, and autoimmune diseases, could also be important. Sub-analysis was not feasible due to a lack of specific information or relatively low case numbers, and future larger studies should control for age, sex, BMI and comorbidities.
CONCLUSION
Our descriptive study provides a quantitative snapshot, which indicates that adipocyte deposition and fibrosis formation are different in the four chambers of the human heart. The determination of the exact location of adipose tissue and fibrosis in the heart might be an important starting point for future studies and potentially for the development of cardiovascular diseases and cardiac death.
Footnotes
AUTHOR CONTRIBUTION
Conceptualization: RDT, SC, HMA, RRL; Methodology: YAL, GRRH, ICFN, RDT, HMA, RRL; Formal analysis: YAL, GRRH, SC, RDT, HMA, RRL; Writing - original draft: YAL, HMA, RRL; Writing - review and editing: YAL, GRRH, ICFN, SC, RDT, HMA, RRL; Funding acquisition: HMA, RRL; Supervision: HMA, RRL. All authors read and approved the final manuscript.
DATA AVAILABILITY
The data that support the findings of this study are available from the corresponding author upon reasonable request.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
ETHICS APPROVAL
The Chief Coroner authorised all examinations on the condition that no individuals could be identified from the provided information. Only the forensic pathologist had access to the heart tissue and the identifying details, and the images used for analysis did not contain any identifiable information. As a result, a full ethical review was not required by our University Human Ethics Committee. The study is in accordance with the Helsinki Declaration of 1975.
This work was supported by the Heart Foundation of New Zealand (Grant 1766 awarded to RRL; Grant 1905 awarded to HMA).
Heart Foundation of New Zealand, (grant number 1766, 1905).
Authors