
Abstract
Coccidioidomycosis is a fungal infection prevalent in the Southwestern United States and Northern Mexico. Given its rarity and often asymptomatic nature, disseminated coccidioidomycosis frequently omitted in preliminary differential diagnoses. Our case study presents the postmortem results of an individual who had a reactivated coccidioidomycosis, causing diffuse alveolar damage and resulting in his death. This case study underscores the importance of considering coccidioidomycosis in initial differential diagnoses, particularly in patients with prior exposure to the infection and associated risk factors.
Keywords
Introduction
The condition known as “Valley Fever” is caused by a Coccidioides infection and can lead to a widespread, severe disease known as “Disseminated coccidiomycosis” when it spreads throughout the body. Even though just 1% of those affected progress to this disseminated stage, it can impact various organ systems such as the skin, central nervous system, joint, and bones. The severity of the infection can vary from mild symptoms to life-threatening conditions. Several factors heighten the risk of widespread infection, including old age, weakened immune systems, chronic illnesses, pregnancy, and individuals of African or Filipino descent (1).
Herein, we report postmortem findings of a patient with previous diagnosis of coccidioidomycosis many years ago. Damage from the infection was evident in the lungs, liver, spleen, brain, thyroid, and kidneys. This case outlines the patient’s comprehensive medical history and illustrates that identifying possible reactivation of previously identified coccidioidomycosis can help avert the deadly progression of the disease, especially as the infection can trigger acute respiratory distress syndrome (ARDS).
Case Presentation
An 88-year-old male patient with a medical history that included atrial fibrillation, congestive heart failure, chronic anemia, multiple lung nodules, gastroesophageal reflux disease, postintervention coronary artery disease, osteoarthritis, benign prostate enlargement, chronic hematuria with negative cystoscopy, lung-confined coccidioidomycosis from 20 years ago, hypersensitivity lung disease, and ongoing respiratory failure requiring home oxygen came in with worsening weakness, cough, fatigue, shortness of breath, low blood pressure, and anemia. He was hospitalized and released after 20 days. Key laboratory findings were high liver enzyme levels, reduced Hb (7.2), and a decreased platelet count (58 k/cmm). A recent chest CT revealed numerous new small nodules in both lungs, comparing to the scan from three months prior. However, earlier ground glass opacities showed improvement. Radiology recommended exploring non-specific inflammation, like unusual pneumonia, viral pneumonia, or exposure to environmental factors. Despite having high inflammatory markers, there were no indications of an active infection. An echocardiogram didn’t display any systolic or diastolic issues that might cause shortness of breath. His situation became more complex due to high potassium levels, necessitating hemodialysis. The patient’s breathing worsened rapidly, his blood pressure dropped consistently, and he was pronounced dead on the sixth day after first showing symptoms.
Autopsy Findings
The most salient finding at the autopsy was that bilateral pleural effusion (left: 250 cc, right: 350 cc) with right-sided pleural and interlobar adhesions. Lungs were both congested (left: 910 gm, right: 1350 gm). Multiple enlarged and calcified paratracheal lymph nodes were identified. Additional findings included multiple scattered white/yellow lesions in liver parenchyma and grossly enlarged spleen (380 grams) with congested and necrotic parenchyma. Remaining organs were grossly unremarkable except for a simple cyst in right kidney, mild cardiomegaly, and moderate to severe calcified atherosclerosis in aorta.
Microscopic examination of the lungs revealed diffuse alveolar damage (DAD), interalveolar edema, micro abscess with fungal organisms, and necrotizing granulomatous inflammation associated with spherules indicating a fungal infection had spread to the lungs. Fungal organism identified on periodic acid–Schiff stain was morphologically consistent with Coccidioides spp.
Notably, DAD, mostly in its exudative (acute) phase, accompanied by interstitial, intra-alveolar edema, hyaline membranes on alveolar duct or sacs, and micro abscess were observed in both lungs (Figures 1 –3). There were also many granulomas, with some even having metaplastic bone formations in the right lung apex. This could indicate a prolonged reactive process, possibly secondary to coccidiomycosis. Paratracheal lymph nodes displayed by hyalinized/calcified necrotizing granulomatous inflammation containing coccidioidomycosis spherules.
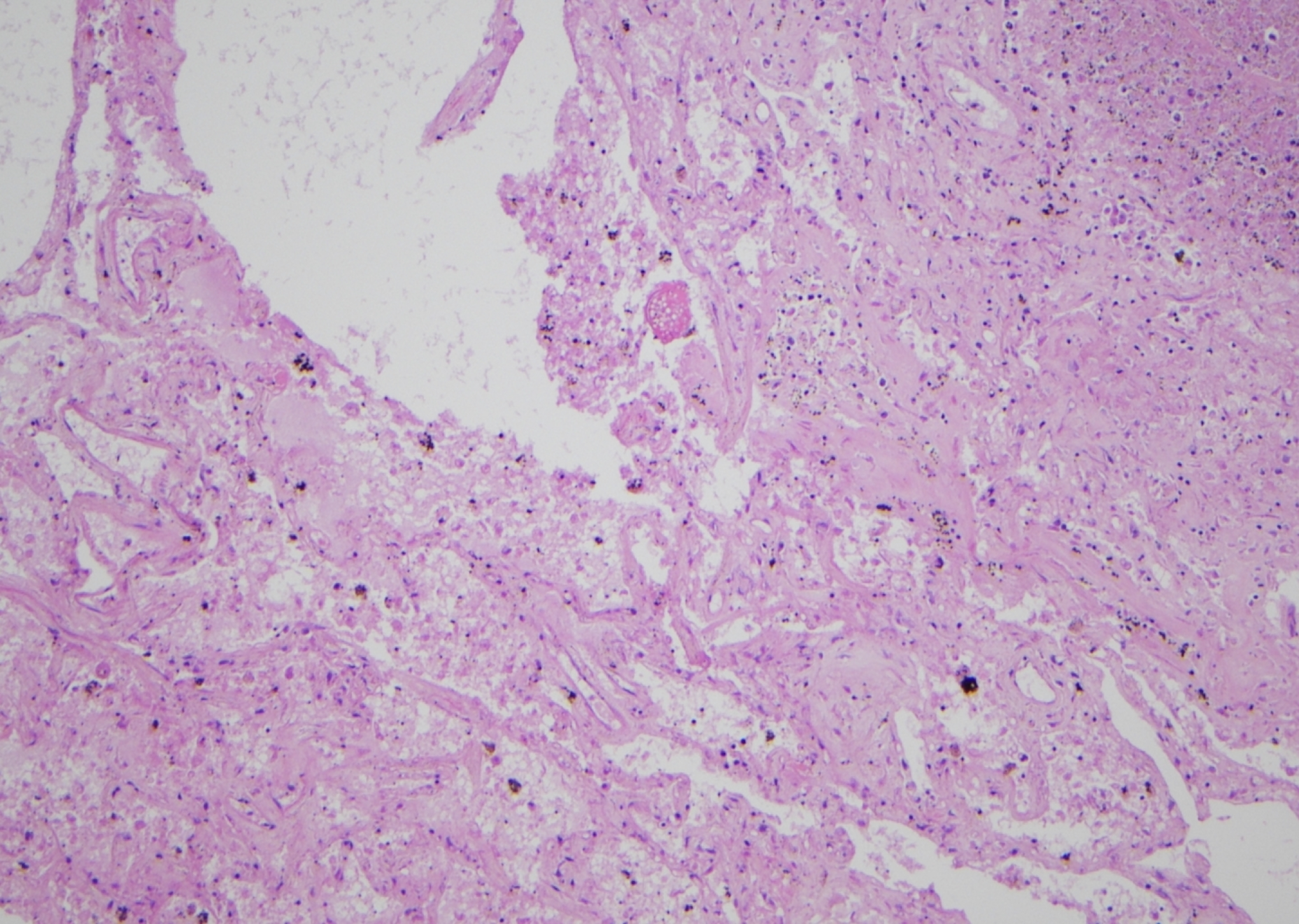
Hematoxylin and eosin (H&E) slide showing diffuse alveolar damage which has intra-alveolar fibrin deposits.
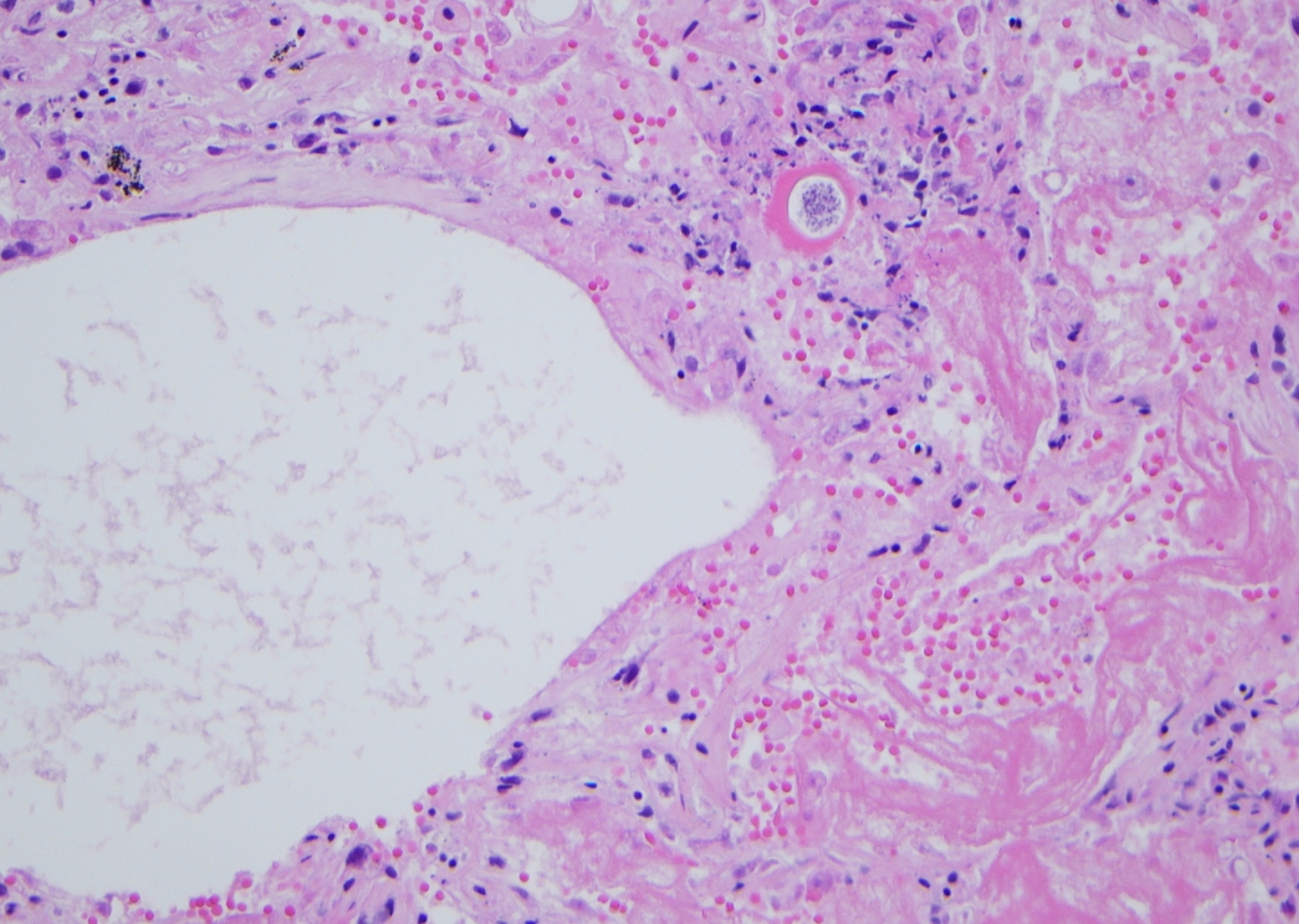
Hematoxylin and eosin (H&E) slide showing formation of hyalin membrane and coccidiomycosis.
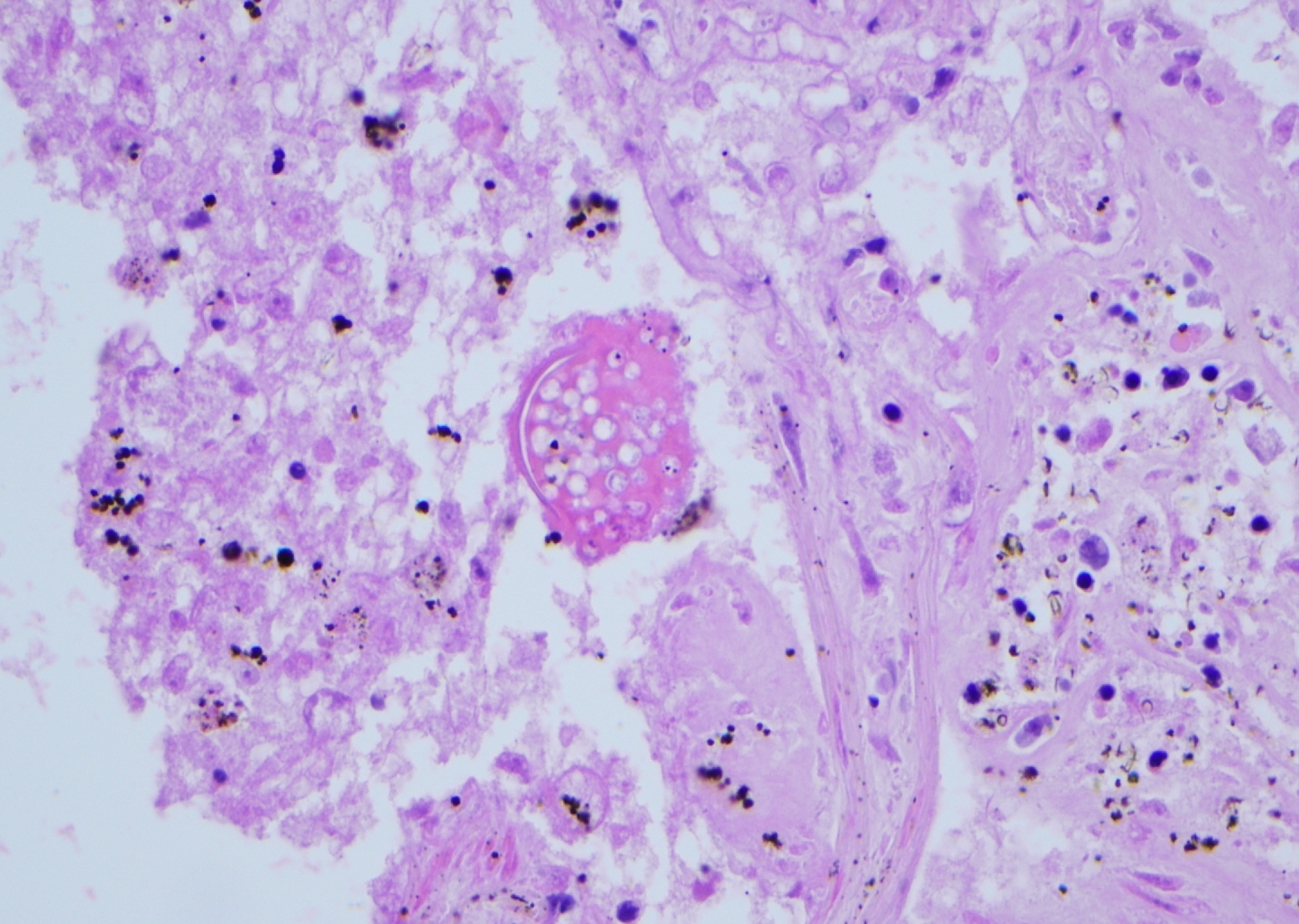
(Continued).
Furthermore, signs of the fungal infection’s spread were evident in the kidneys, liver, spleen, thyroid, and brain (Figure 4). In particular, the glomeruli and interstistium involved by micoabscesses admixed with coccidiomycosis fungal organisms (Figure 5). There weren’t any signs suggesting other organs were affected. The cause of death is favored to be respiratory failure due to DAD with contributing comorbidities disseminated coccidioidomycosis and coronary artery disease.
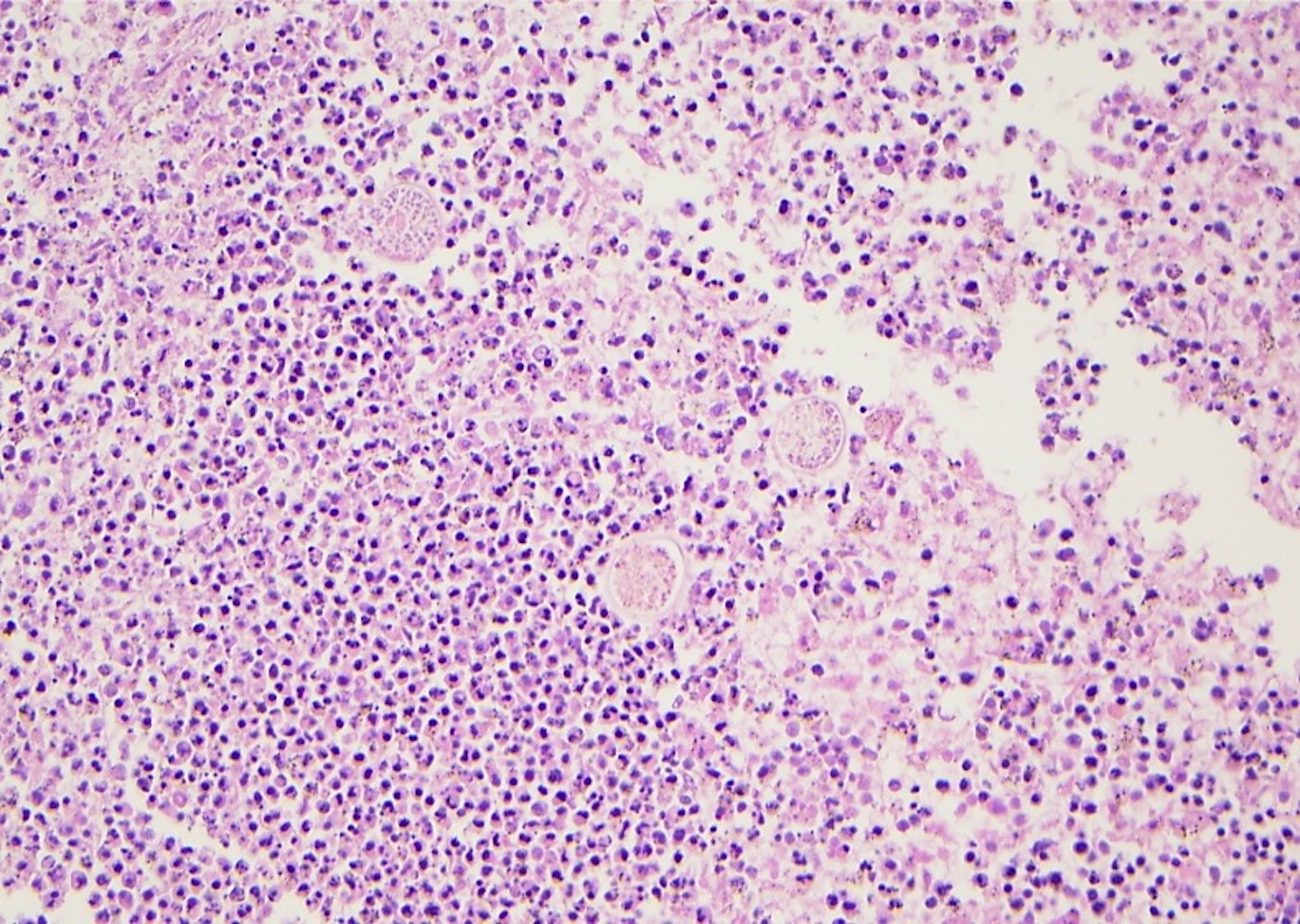
Hematoxylin and eosin (H&E) slide demonstrating micro abscess formation with coccidiomycosis organisms at spleen.
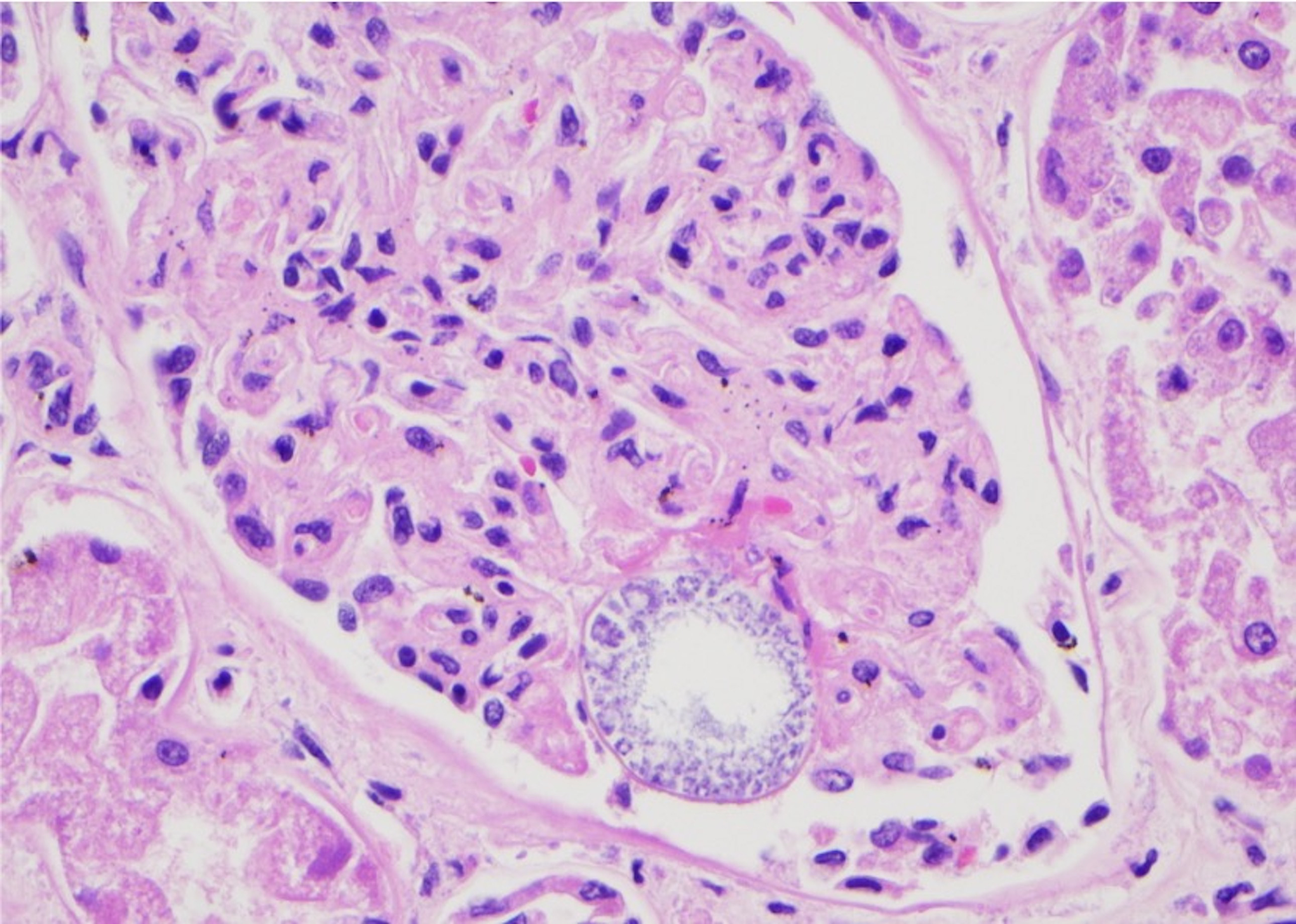
Hematoxylin and eosin (H&E) slide showing glomeruli with coccidiomycosis.
Discussion
Coccidioides infection is endemic in specific regions, notably the southwestern United States (including Arizona, California, Nevada, New Mexico, Texas, and Utah), as well as certain areas in Mexico and Central and South America. The fungus is found in soil or dust and infects people through inhalation. The patient discussed in this case, a construction worker from Arizona, was diagnosed with coccidiomycosis two decades ago.
Exposure to the Coccidioides does not necessarily lead to infection. Many remain unaffected, but those who do get infected may experience non-specific symptoms within weeks to months, such as fever, cough, fatigue, shortness of breath, and night sweats. Identifying disseminated coccidioidomycosis can be challenging due to its ambiguous symptoms. Interestingly, men seem to have a heightened risk of dissemination. While not all infected individuals need antifungal treatment, the Infectious Diseases Society of America advises treating those at high risk, including the immunocompromised, pregnant women, diabetics, critically ill patients, and those of African or Filipino descent. In cases where the infection spreads, treatments like fluconazole or amphotericin B are typically prescribed. The skin is usually the primary site of dissemination, but it can also affect joints, bones, and meninges (1,2).
Chee et al. previously demonstrated the involvement of the tongue, lungs, brain, and adrenal glands in an autopsy case (3). Notably, the patient had a clinical history of cirrhosis and lymphocytopenia and died of aspiration pneumonia, even after receiving antifungal treatment. Their literature review of just five cases revealed instances of tongue infection. In a related study, Raza et al. discussed an unusual case of disseminated Coccidioidomycosis in a thyroid nodule (4). They pointed out the rarity of thyroid involvement, with fewer than 10 cases reported. Our case similarly showed thyroid involvement by disseminated Coccidioidomycosis.
Woo et al. also reported the involvement of the lungs, liver, tracheobronchial lymph nodes, adrenal glands, spleen, and skin in an autopsy report (5). The deceased, once a resident of an endemic region, experienced a reactivation of the infection three years after the initial diagnosis of pulmonary coccidioidomycosis. In our situation, the reactivation took place 20 years post-initial diagnosis. In another autopsy report, Amoth et al. described a forensic case of disseminated coccidioidomycosis found in a nonendemic area (6). Although a past residency in California was discovered, the deceased had no known immunocompromising conditions. Due to this, coccidioidomycosis wasn’t initially considered in their primary diagnosis. The authors emphasize the importance of considering coccidioidomycosis as a possible diagnosis, regardless of a patient’s clinical history.
Reactivation of an infection can lead to dissemination even years after the primary infection. Monitoring the disease is crucial for clinicians when evaluating a patient with past medical history of the infection. Arbeloa et al. highlighted the unpredictable nature of these reactivations in a case study (7). They described a patient who had previously recovered from pneumonia showed reactivation of a Coccidioides infection 56 years after leaving the endemic area. Most patients with coccidioidomycosis infectious are asymptomatic; symptomatic patients typically present with pneumonia. Although usually self-limiting, it may develop into acute respiratory distress syndrome (ARDS) as a result of disseminated coccidioidomycosis (8).
Conclusion
Diagnosis of coccidioidomycosis can be challenging, especially in nonendemic regions. This challenge arises from its infrequent occurrence and as well as its nonspecific symptoms which often leads to misdiagnoses or delayed interventions. Many patients with coccidioidomycosis infections show no symptoms, but those who do often exhibit signs of pneumonia. While this condition is generally self-resolving, it can progress to ARDS due to the spread of coccidioidomycosis. Comprehensive medical history documentation enhances clinical suspicion, facilitating faster treatment and improving patient prognosis. In our unique case, the reactivated disseminated coccidioidomycosis led to DAD, which was evidenced by the presence of hyaline membranes, a histological correlate of ARDS.
Footnotes
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Disclosures & Declaration of Conflicts of Interest
The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest.
Financial Disclosure
The authors have indicated that they do not have financial relationships to disclose that are relevant to this manuscript.