
Abstract
Aortoesophageal fistula (AEF) is a rarely encountered clinical outcome that is often fatal. It is most commonly a postoperative complication of vascular surgery (secondary AEF). Reported primary causes of AEF include aortic aneurysm, atherosclerosis, infection, foreign objects, achalasia with megaesophagus, gastrointestinal malignancy, and radiotherapy. Aortoesophageal fistula is often not a top diagnostic consideration for clinicians or pathologists and has the potential to be overlooked. This report describes a rare case of AEF secondary to an esophageal traction diverticulum and associated abscess that resulted in the sudden unexpected death of a 78-year-old male. Aortoesophageal fistula is an important consideration for pathologists and requires careful consideration in the postmortem setting.
Introduction
Aortoesophageal fistula (AEF) is a rarely encountered clinical outcome that is most often a result of esophageal malignancy or a postoperative complication from thoracic aortic aneurysm endovascular repair (TEVAR procedure) (1 -8). It has also been reported in the rare settings of a swallowed foreign object, achalasia with megaesophagus, as part of a trachea–AEF in the setting of a patient with a double aortic arch and tracheostomy, esophageal infection, radiotherapy, bronchial carcinoma, caustic ingestion, and perforation of Barrett’s ulcer (9 -17). Regardless of the etiology, the outcome for patients with AEF is often fatal due to exsanguination.
The clinical presentation of AEF can vary, ranging from hematemesis, chest pain, or sudden unexpected death (18). Unless the patient has a clear history of esophageal malignancy or TEVAR procedure, AEF may not be considered in the differential diagnosis in both the ante- and postmortem settings.
In this case report, we describe a rare case of AEF secondary to esophageal traction diverticulum resulting in the sudden and unexpected death of a 78-year-old male.
Case Report
A 78-year-old male with a past medical history of benign prostatic hypertrophy and hypercholesterolemia had new-onset chest pain six days prior to his death. The decedent presented with chest pain radiating to the right and left upper quadrants of the abdomen and to the left arm. His other presenting signs and symptoms included nausea, vomiting, diaphoresis, cough, and shortness of breath. He was afebrile at initial presentation. Initial chest X-ray showed cardiomegaly and increased vascular markings. Electrocardiogram showed sinus tachycardia, and troponin was negative. He was treated for presumed pneumonia with intravenous ceftriaxone and azithromycin. A computerized tomography scan was ordered and pending to rule out pulmonary embolism. Within moments of receiving hydromorphone for chest pain, the decedent experienced tonic–clonic seizures. Lorazepam was administered, but unfortunately, resuscitation efforts were unsuccessful, and he died shortly after.
A complete medicolegal autopsy was performed. The external examination demonstrated an Asian male appearing 78 years of age. No external evidence of injury was present. Internal examination revealed bilateral hemothoraces, with 250 mL of blood present in the left pleural cavity and 2000 mL of partially clotted blood present in the right pleural cavity. Subsequent examination revealed a mediastinal hematoma and paraesophageal hemorrhage at the level of the mid-thoracic esophagus and ascending aorta.
A cardiovascular pathologist was consulted, confirming the presence of a paraesophageal and para-aortic abscess cavity, measuring approximately 2.5 cm, of the mid-thoracic esophagus and ascending aorta (
Figures 1
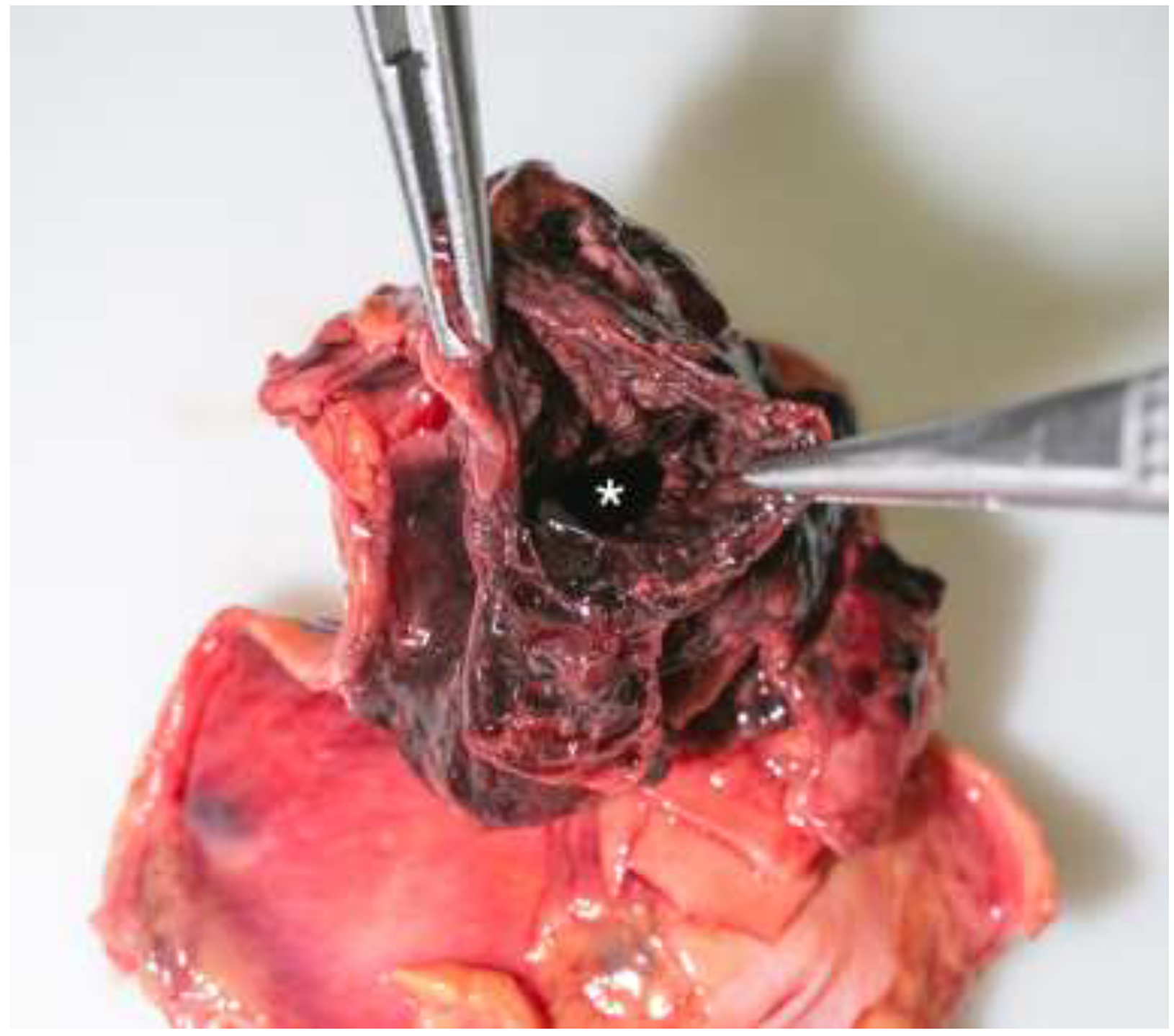
Abscess cavity(*) between the esophageal and aortic defects.

Cross section of esophageal (*) and aortic(↓) defects with adjoining abscess cavity (⇒), formalin-fixed specimen.

Esophagus with transmural defect extending into adjacent abscess cavity.

Aorta with severe, complicated atherosclerosis and a 0.6 cm defect.
Microscopic examination of the abscess determined the presence of polymicrobial bacteria, staining positive for both gram-positive and gram-negative cocci clusters and chains. Within the abscess cavity were bundles of smooth muscle, attributed to a traction esophageal diverticulum (
Figures 5
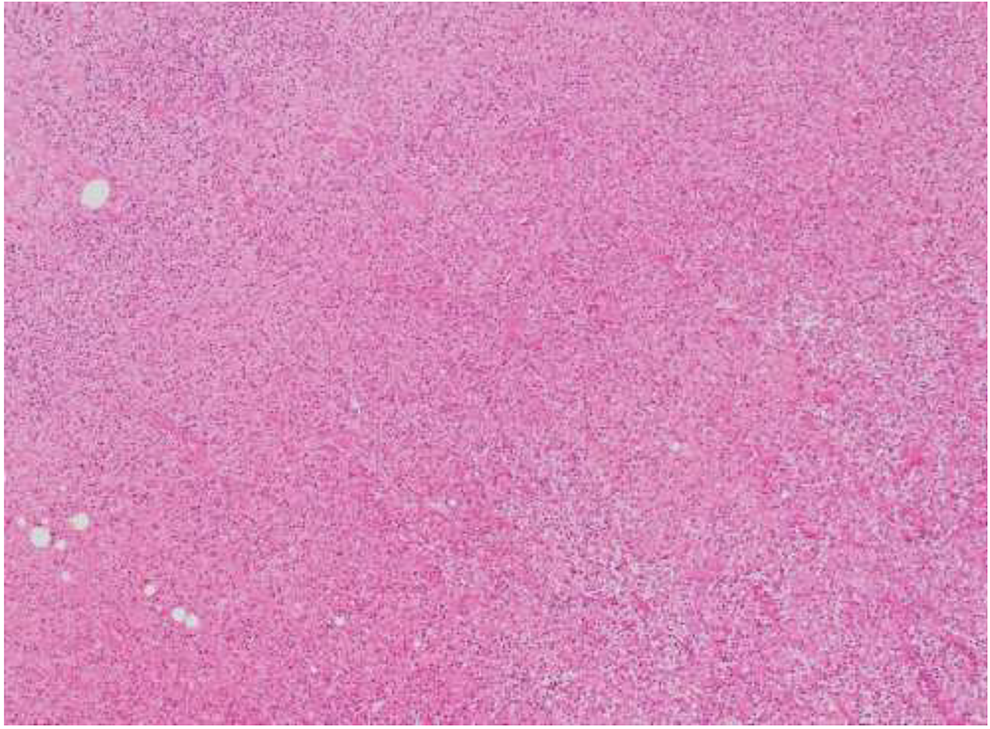
Abscess cavity with bundles of smooth muscle, attributed to a traction esophageal diverticulum (hematoxylin and eosin [H&E], ×4 magnification).
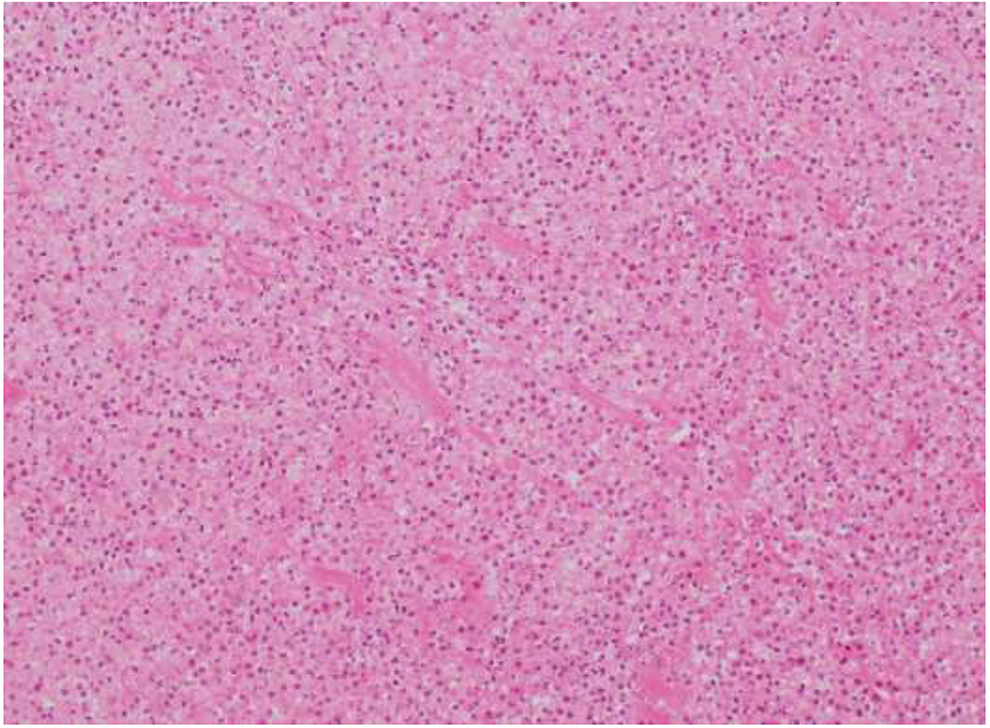
Abscess cavity with bundles of smooth muscle, attributed to a traction esophageal diverticulum (hematoxylin and eosin [H&E], ×40 magnification).
Discussion
Aortoesophageal fistula is characterized by Chiari’s triad of mid-thoracic pain, a subsequent “herald” hemorrhage, followed by massive hematemesis that is often fatal (16). It is an uncommon presentation of sudden unexpected death in forensic pathology. As is true in this case, the clinical presentation may be initially mistaken for more commonly encountered entities such as a myocardial infarction or pulmonary embolism. Due to the possibility of massive hematemesis, the scene at which death occurs may initially appear to be suspicious. For this reason, a thorough medicolegal investigation by a forensic pathologist is of utmost importance to correctly classify the cause of death.
Primary aortoenteric fistula (PAEF) is an open connection between the aorta and a part of the gastrointestinal (GI) tract (18). Causes include aortic aneurysm, atherosclerosis, infection (tuberculosis, syphilis, candida), foreign objects, achalasia with megaesophagus, trachea–AEF in the setting of a patient with a double aortic arch and tracheostomy, GI malignancy, bronchial carcinoma, caustic ingestion, and perforation of Barrett’s ulcer (9 -20). The reported incidence of PAEF in the general population is 0.07%, and the mortality rate can approach 100% if it is not rapidly diagnosed and managed (18). Among PAEF, AEFs comprise approximately 25% of cases, attributable to the close contact of the aorta and esophagus over a long distance (18).
A more frequently encountered scenario, termed a secondary aortoenteric fistula, results from previous vascular surgery, such as a TEVAR procedure (18). Distinguishing the two entities is an important part of the postmortem examination to accurately determine the cause of death.
Esophageal traction diverticulum often results from mediastinal inflammation in a setting of infection, such as tuberculosis or histoplasmosis (21). Only one previous fatal case of a similar traction diverticulum resulting in AEF and sudden death was described in 1975. However, this case differed from ours in that the patient had known long-standing tuberculosis involving the esophageal diverticulum, whereas our patient had no documented history of infection (22). To our knowledge, this case represents one of the first documented primary AEFs from a traction diverticulum presenting with sudden unexpected death. Due to the limited available medical history at the time of the autopsy, the exact cause of the traction diverticulum was not able to be determined in this case.
In summary, aortic-esophageal fistula is a rare clinical outcome that has a high mortality and that can present as a sudden unexpected death. This case adds to the literature available, as it is one of the first reported cases of primary AEF due to a traction diverticulum of the esophagus. A complete medicolegal autopsy is an important element in determining both the cause of death and the etiology of the AEF.