
Abstract
Importance
Tonsillectomy has long been scrutinized for its potential long-term impacts on health, with conflicting evidence linking it to increased risks of several diseases, such as cancer, psychiatric disorders, and immune dysfunctions.
Objective
To comprehensively analyze the effects of tonsillectomy on various disease outcomes.
Design
Longitudinal cohort study, 2-sample Mendelian randomization (MR) analysis, and multivariable MR (MVMR) analysis.
Setting
The UK Biobank.
Participants
All UK Biobank (UKB) participants who did not withdraw from the UKB were included. Individuals diagnosed with benign or malignant tonsil tumors, with conflicting information regarding the timing of tonsillectomy, a history of adenoidectomy without tonsillectomy, and incomplete data on birth year, sex, and ethnic background were excluded.
Intervention or exposures
Tonsillectomy.
Main outcome measures
Incident diseases diagnosed based on International Classification of Diseases diagnostic codes and self-reported doctor-diagnosed disease histories.
Results
Tonsillectomy was significantly associated with 17 primary core outcomes (incidence ≥ 1%, P < .001, hazards ratio [HR] ≥ 1.10 or HR ≤ 0.90) among the general population. Among individuals with tonsillitis, those who underwent tonsillectomy were at greater risk of developing 7 secondary core outcomes than those who did not have the surgery. To assess potential causal associations, we performed 2-sample MR analysis and observed that tonsillectomy was causally associated with asthma, depression, irritable bowel syndrome (IBS), and anxiety. Additionally, tonsillitis was causally associated with depression, IBS, and anxiety. However, when applying MVMR analysis to account for potential confounders, the causal relationship between tonsillectomy or tonsillitis and depression or anxiety were no longer observed. Notably, tonsillitis remained causally associated with IBS in the MVMR analysis.
Conclusions
These findings suggest that the observed associations between tonsillectomy and various disease outcomes may be more attributable to the underlying effects of tonsillitis, rather than causal effects of the surgery itself. This evidence supports the safety of tonsillectomy in clinical practice.
Relevance
The findings of this study addressed the concerns about the adverse effects of tonsillectomy, supporting the safety of tonsillectomy in clinical practice.

Keywords
Key Message
Tonsillectomy seemed to be a double-edged sword, epidemiologically associated with higher risks of certain diseases while lower risks of some others.
Tonsillectomy was not causally associated with the diseases we tested, indicating that the observed clinical relevance was due to some underling factors.
Epidemiologically, age 8 was a turning point at which the potential impact of tonsillectomy changed from risk-decreasing to risk-increasing for most disease outcomes.
Introduction
The tonsils are immune organs located in the posterior part of the oral cavity, at the entrance of the respiratory and digestive tracts. This special anatomic location exposes the tonsils to various environmental agents, enhancing their roles as the first line of defense against antigens. 1 Although the immune function of the tonsils peaks between the ages 3 and 10 and declines after adolescence,2,3 recent studies have highlighted an underestimated immune role of the tonsils in adulthood.3 -5
The primary indications for tonsillectomy include chronic inflammatory conditions such as recurrent tonsillitis and tonsil hypertrophy.6,7 Although the indications, surgical rates, and surgical techniques vary across different countries and over time within the same regions, tonsillectomy remains 1 of the most common surgical procedures performed on children and young adults.8 -10 Therefore, the high rates of surgical removal, coupled with the still elusive immune roles of the tonsils, have raised significant concerns regarding the long-term effects of tonsillectomy on human health and the optimal age for surgery.
Numerous studies have examined the effects of tonsillectomy on various health-related outcomes, yet no consensus has been reached. There is accumulating evidence suggesting that tonsillectomy is associated with increased risks of developing Hodgkin lymphoma, leukemia, breast cancer, and oral cancer, while contradictory findings have also been reported. Besides, some researchers have argued that the elevated disease risks observed in participants undergoing tonsillectomy may be attributable to the effects of tonsillitis or a heightened susceptibility to infections, rather than the procedure itself.11 -13 Results from a genome-wide association study (GWAS) further support this perspective, demonstrating that mutations in the HORMAD2 gene are associated with both tonsillectomy and tonsillitis, rendering the impacts of tonsillectomy still confusing. 14
In this study, we conducted an outcome-wide association analysis using the large-scale population-based UK Biobank (UKB) cohort to explore the potential associations between tonsillectomy and various health-related outcomes. Besides, we employed Mendelian randomization (MR) and multivariable MR (MVMR) approaches to infer the causal relationships between tonsillectomy or tonsillitis with clinically relevant outcomes, aiming to provide further insights into the safety concerns associated with tonsillectomy.
Methods
Data Source and Ethics
The current outcome-wide association analysis was conducted using the UKB cohort 15 under generic ethical approval obtained by UKB from the North West Multi-Centre Research Ethics Committee. Over 500,000 participants completed touchscreen questionnaires, verbal interviews, and physical measurements after providing written informed consents.
Exposure
The exposure of this study was tonsillectomy, defined as a self-reported history of tonsillectomy (self-reported operation code 1478 and 1561), or an Office of Population Censuses and Surveys Classification of Interventions and Procedures version 4 (OPCS4) code F34 or version 3 (OPCS3) codes 231, 233 or 234.
Participants Inclusion and Exclusion Criteria and Matching Process
All UKB participants who did not withdraw from the UKB were included. Individuals diagnosed with benign or malignant tonsil tumors by International Classification of Diseases version 10 (ICD-10) codes D104 or C09 or version 9 (ICD-9) codes 1460, 1461, or 1462 were excluded. Further exclusion criteria included conflicting information regarding the timing of tonsillectomy, a history of adenoidectomy without tonsillectomy, and incomplete data on birth year, sex, and ethnic background. In the subsequent primary and secondary outcome-wide association analyses, participants who developed the outcome before or within 1 year of the start of follow-up were excluded from the corresponding analysis (Figure 1).
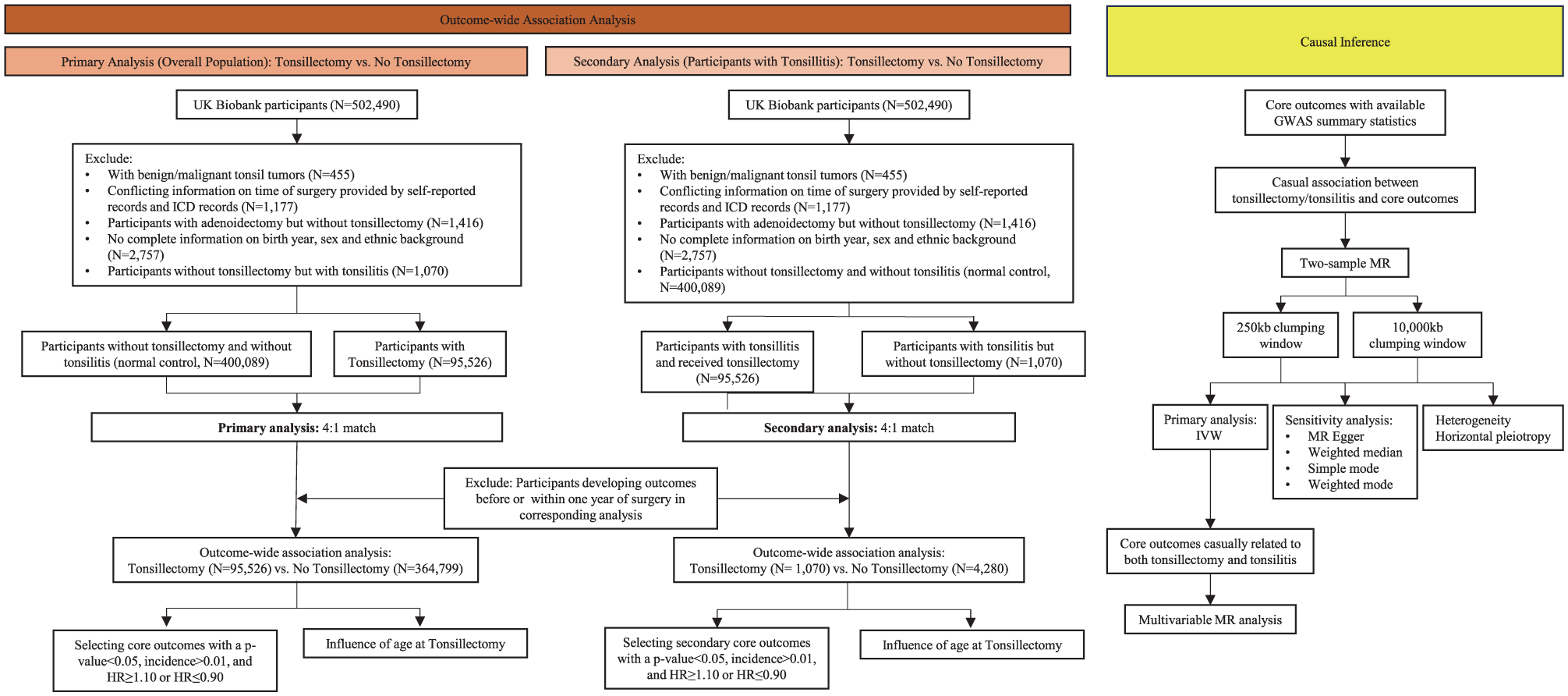
Flowchart of the study design. ICD, International classification of diseases; HR, Hazards ratio; GWAS, Genome-wide association study; MR, Mendelian randomization.
In primary analysis, we compared participants who underwent tonsillectomy to normal controls without tonsillectomy and tonsillitis (ICD-10 codes J350, J351, J353, J358, J359, or J36; ICD-9 codes 474 or 475; self-reported doctor-diagnosed disease history code 1598). For each participant with tonsillectomy, we matched up to 4 normal controls based on birth year, sex, and ethnic background using nearest neighbor propensity score matching.
In secondary analysis, we compared disease-related outcome differences between patients with tonsillitis who did not undergo tonsillectomy and those who did. This analysis was limited to participants aged 35 years or older, as most tonsillitis patients in the UKB were diagnosed after this age. For each participant with tonsillitis who did not receive tonsillectomy, we matched up to 4 participants who had undergone tonsillectomy using the same method and variables as the primary analysis (Figure 1).
Covariates
Information on birth year, sex, ethnic background, smoking status, regular physical activity (Supplemental Table 1), 16 diet (Supplemental Table 1), 17 and alcohol consumption (Supplemental Table 1) 17 was obtained from the UKB touchscreen questionnaires.
Outcomes and Follow-up
Outcomes for the current study were defined as incident diseases diagnosed based on ICD-10 codes, ICD-9 codes, and self-reported doctor-diagnosed disease histories during the follow-up period. The outcomes included in the subsequent outcome-wide association analysis were determined through the following procedures. First, we restricted our disease classifications to ICD-10 coding chapters 1 to 14, excluding codes related to pregnancy, childbirth, perinatal conditions, congenital conditions, unclassified symptoms or signs, external causes, external causes of morbidity and mortality, and factors influencing health status and contact with health services. Next, we defined outcomes based on the 2-digit ICD-10 codes and grouped them according to clinical or biological similarities. Finally, diagnoses from ICD-9 codes and self-reported doctor-diagnosed disease histories were mapped to the ICD-10 defined outcomes. The detailed codes used to define each of the 474 outcomes are listed in Supplemental Table 2. Four outcomes were excluded from the analysis due to a limited number of cases (N < 10): “Nutritional and metabolic disorders in diseases classified elsewhere” and “Keratoderma in diseases classified elsewhere,” as well as indications rather than consequences of tonsillectomy: “Chronic disease of tonsils and adenoids” and “Peritonsillar abscess.” This resulted in a final list of 470 outcomes.
Participants with tonsillectomy were followed up from the age of surgery, while those without tonsillectomy were followed up from the surgery age of their matched counterparts. All participants were followed up until death, diagnosis of a certain outcome in the corresponding analysis, or the start of the study (June 22, 2022), whichever came first.
Statistical Analysis
Descriptive Analysis
Categorical variables were presented as frequencies with percentages, while continuous variables were presented as means with standard deviations or medians with ranges. Student’s t-tests and Chi-square tests were performed as appropriate to evaluate the differences in characteristics between participants with and without tonsillectomy.
Outcome-wide Association Analysis of the Influence of Tonsillectomy on Disease Outcomes
Univariable and multivariable Cox proportional hazards regression models were constructed to perform the outcome-wide association analysis evaluating the effects of tonsillectomy on disease outcomes. Covariates included current smoking status, regular physical activity, diet habits, and moderate drinker status in the multivariable models. Primary and secondary core outcomes were defined as disease outcomes with an incidence ≥1% among participants with tonsillectomy, a P-value < .001, and a hazards ratio (HR) ≥ 1.10 or ≤0.90 as they represent the most prevalent and statistically robust diseases that are more clinically relevant.
Exploring the Effects of Age at Tonsillectomy
As the tonsils play a crucial role in the development of the immune system, the effects of tonsillectomy on disease outcomes may vary depending on the age at which the surgery is performed. To test this hypothesis, we modeled a nonlinear relationship between age at tonsillectomy and core outcomes using restricted cubic spine (RCS) models, adjusting for the same variables used in the multivariable outcome-wide associations. Besides, cumulative incidence plots were further generated to visualize the incidence of core outcomes following tonsillectomy, based on the turning point age of tonsillectomy determined by the RCS models.
Two-sample MR Analysis Evaluating the Causal Effects of Tonsillectomy on Disease Outcomes
Two-sample MR analyses were carried out to evaluate the potential causal links between core outcomes with tonsillectomy and/or tonsillitis. GWAS summary statistics for the exposures in the MR analysis, specifically tonsillectomy and tonsillitis, were obtained from the FinnGen study (data release version 7). 18 Only core outcomes with available GWAS summary statistics were included as MR analysis outcomes. We generated 2 sets of instrumental variables (IVs) for tonsillectomy and tonsillitis by clumping genetic variants associated with tonsillectomy/tonsillitis at a suggestive genome-wide significance level (P < 5E-5) based on linkage disequilibrium (LD, r2 = 0.10) and 2 physical position thresholds (up/downstream ± 10,000 kb and up/downstream ± 250 kb, respectively). For IVs not present in the outcome GWAS summary statistics, variants in high LD (r2 > 0.80) from the 1000 Genomes European dataset were selected and served as LD proxies.
The causal effects of tonsillectomy and tonsillitis on each outcome were tested using the Inverse Variance Weighted method19,20 with the 2 sets of IVs, respectively.
Multivariable MR Analysis Eliminating the Influence of Potential Cofounder
For outcomes with a causal association with both tonsillectomy and tonsillitis in the 2-sample MR analysis using either set of IVs, we employed MVMR analysis to further dissect these causal associations. Body mass index (BMI), smoking initiation, and Type 2 diabetes (T2D) were included as covariates in the MVMR analysis due to their significant impacts on the immune system. We adjusted the effects of these covariates in turn (2-way MVMR, tonsillectomy/tonsillitis + BMI, tonsillectomy/tonsillitis + smoking initiation, or tonsillectomy/tonsillitis + T2D) or adjusted for all covariates simultaneously (4-way MVMR, tonsillectomy/tonsillitis + BMI + smoking initiation + T2D).
Software
All analysis were performed using the R software (version 3.6.3, https://www.r-project.org/). A two-tailed P-value < .05 was considered statistically significant. Matching was conducted using MatchIt R package (version 4.5.3). Outcome-wide association analyses were performed using the survival R package (version 3.5.5). MR and MVMR analyses were performed using the 2-sample MR R package (version 0.5.6). Moreover, RCS models were generated using the rms R package (version 6.7-1).
Patient and public involvement statement
Patients or the public WERE NOT involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Baseline Characteristics of Participants Undergoing Tonsillectomy versus Normal Controls
A total of 460,325 participants were included in the study with a median age of 58 years (range: 39-73). Among them, 95,526 participants underwent tonsillectomy and 364,799 normal controls without tonsillectomy or tonsillitis were matched for comparison at a 1:4 ratio based on birth year, sex, and ethnicity. No significant differences in baseline characteristics were observed between participants with tonsillectomy and normal controls (Supplemental Table 3).
Primary Analysis: Outcome-wide Association Analysis of Participants Undergoing Tonsillectomy Compared to Normal Controls
To comprehensively explore the impacts of tonsillectomy on various disease outcomes, we performed an outcome-wide association analysis using both univariable and multivariable Cox proportional hazards regression models (Figure 1). This analysis identified 147 disease outcomes significantly associated with tonsillectomy (Supplemental Table 4, Figure 2). To provide the most prevalent and statistically robust disease associations, we focused on a set of 17 primary core outcomes that had an incidence of ≥1% in participants with tonsillectomy, a P-value < .001, and a HR ≥ 1.10 or ≤0.90 (Table 1). Specifically, tonsillectomy exhibited preventive effects on the development of physiological condition triggered delirium (incidence = 1.33%, HR = 0.88, 95% CI 0.83-0.94), acute myocardial infarction (incidence = 4.06%, HR = 0.89, 95% CI 0.86-0.92), and respiratory failure (incidence = 1.44%, HR = 0.86, 95% CI 0.81-0.91). Nevertheless, opposite effects were observed between tonsillectomy and the remaining 14 primary core outcomes across various systems.

Results of the outcome-wide association analysis evaluating the effects of tonsillectomy on incident diseases. (a-b) The results of the primary (a) and secondary (b) outcome-wide association analyses. Different colors represent different categories of diseases; area size indicates hazards ratio; (+) indicates hazards ratio >1 and (-) indicates hazards ratio <1. ** indicates “core outcomes.” (c) The evidence level of the association between tonsillectomy and diseases. MR, Mendelian randomization; MVMR, Multivariable Mendelian randomization; IBS, Irritable bowel syndrome.
The Results of the Outcome-Wide Association Analysis for the Effects of Tonsillectomy.

Abbreviations: CI, Confidence interval; HR, Hazards ratio. Bold P-values indicates significant P-values < .05.
Only the disease outcomes with a P-value < .001, an HR ≥ 1.10 or an HR ≤ 0.90, and an incidence ≥1.00% were listed here, and the full results for the significant associations were listed in Supplemental Table 4.
Secondary Analysis: Outcome-wide Association Analysis of Tonsillectomy versus Non-tonsillectomy in Patients with Tonsillitis
Given that tonsillitis is a common situation observed in participants who have undergone tonsillectomy, it may influence the relationship between tonsillectomy and disease outcomes. Therefore, we compared disease outcomes in participants with tonsillectomy (n = 4,280) to those without tonsillectomy among individuals with tonsillitis (n = 1,070), employing a 4:1 matching approach (Supplemental Table 5). This further analysis identified 48 outcomes significantly associated with tonsillectomy (Supplemental Table 7, Figure 2). Among these, 7 diseases were classified as “secondary core outcomes,” meeting the criteria of a P-value < .001, a HR ≥ 1.10 or ≤0.90, and an incidence ≥1% in participants with tonsillectomy. These secondary core outcomes included tobacco abuse, depression, anxiety, sleep disorder, upper respiratory infections, pneumonia, and umbilical hernia (Supplemental Table 7).
Mediating Effects of Age at Surgery on the Outcome-wide Association Analysis of Tonsillectomy
To investigate the mediating effects of age at surgery on the impacts of tonsillectomy on disease risks, we modeled the nonlinear effects of tonsillectomy on core outcomes, with the effects varying according to the age at which tonsillectomy was performed. Our primary analysis revealed that the effect of tonsillectomy shifted with age, identifying age 8 as a turning point at which the impact changed from risk-reducing to risk-increasing for most outcomes (Supplemental Figure 1). This suggests that age 8 may be the optimal age for tonsillectomy to minimize adverse sequela. In the secondary analysis, we observed that age 56 also served as a turning point; however, a consistent trend in the changing effects of tonsillectomy was not observed. Cumulative incidence plots for the core outcomes, stratified by tonsillectomy status and age at tonsillectomy, were presented in Supplemental Figure 2.
Causal Evaluation of Tonsillectomy/Tonsillitis on Primary Core Outcomes
To further infer the causal relationships between tonsillectomy/tonsillitis and disease outcomes, we employed 2-sample MR analysis on core outcomes with available GWAS summary statistics (11 out of 23 core outcomes). The results suggested that there was no causal association between tonsillectomy/tonsillitis with allergic rhinitis, acute myocardial infarction, hypothyroidism, migraine, pneumonia, sleep disorder, nor umbilical hernia using a clumping window of 250 kb and 10 Mb. Nevertheless, we found evidence of causal effects of both tonsillectomy and tonsillitis on the development of depression (tonsillectomy: clumping window = 10 Mb, odds ratio [OR] = 1.11, 95% CI 1.00-1.22, P = .045; tonsillitis: clumping window = 10 Mb, OR = 1.55, 95% CI 1.07-1.23, P < .001; tonsillitis: clumping window = 250 kb, OR = 1.15, 95% CI 1.09-1.22, P < .001), anxiety (tonsillectomy: clumping window = 250 kb, OR = 1.36, 95% CI 1.07-1.72, P = .011; tonsillitis: clumping window = 10 Mb, OR = 1.26, 95% CI 1.02-1.55, P = .030; clumping window = 250 kb, OR = 1.32, 95% CI 1.09-1.60, P = .005), and IBS (tonsillectomy: clumping window = 250 kb, OR = 1.14, 95% CI 1.07-1.21, P < .001; tonsillitis: OR = 1.07, 95% CI 1.01-1.13, P = .013). Besides, tonsillectomy was significantly associated with asthma (clumping window = 250 kb, OR = 0.62, 95% CI 0.45-0.84, P = .002).
However, the results of the 2-sample MR analyses could not eliminate the effects of conventional confounding factors such as BMI, smoking initiation, and T2D. Therefore, we applied MVMR to further validate these potential causal associations (Figure 2). Tonsillectomy was causally associated with a higher risk of depression only after adjusting for T2D (10 Mb clumping window: OR = 1.22, 95% CI 1.05-1.42, P = .00998; Supplemental Table 8), while the association between the 2 were no more significant after adjusting for BMI or smoking initiation. Furthermore, results of the 4-way MVMR also declined any causal association between tonsillectomy and depression (Figure 3 and Supplemental Table 8). Similarly, the 4-way MVMR results suggested no causal association between tonsillitis and depression, nor between tonsillectomy or tonsillitis and anxiety (Figure 3 and Supplemental Table 8). In contrast, while tonsillectomy was not significantly associated with IBS in the 4-way MVMR, tonsillitis showed a causal association with IBS after accounting for T2D, smoking initiation, and BMI (Figure 3 and Supplemental Table 8).

The schematic diagram of the MVMR analysis revealing the associations between tonsillectomy/tonsillitis and depression, anxiety, or IBS. The dash arrow and blue “×” indicate the instrumental variable assumptions of mendelian randomization analysis. Red “×” indicates no causal association between the variable and the outcome in the MVMR. These results suggested that there is no causal association between tonsillectomy and depression (a), anxiety (b), nor IBS (c). There is also no causal association between tonsillitis and depression (d and g) or between tonsillitis and anxiety (e and h). However, there was a significant causal association between tonsillitis and IBS (f). Detailed results were listed in Supplemental Table 8. MVMR, Multivariable Mendelian randomization; SNP, single-nucleotide polymorphism; IBS, irritable bowel syndrome.
Collectively, our results indicated no causal relationship between tonsillectomy and various disease outcomes, including allergic rhinitis, acute myocardial infarction, hypothyroidism, migraine, pneumonia, sleep disorder, umbilical hernia, depression, and anxiety, etc., whereas tonsillitis was found to be causally associated with IBS.
Discussion
The high rates of tonsillectomy and the uncertain immune function of the tonsils have raised significant concerns about the long-term effects of tonsillectomy on human health. In this study, we investigated the associations between tonsillectomy and various disease risks using 2 approaches: an outcome-wide association study based on clinical and demographic data from the large prospective database (UKB) and a MR study utilizing genetic data from several large-scale genome research collaborations.
Comparing participants with tonsillectomy to normal controls without tonsillectomy and tonsillitis, our outcome-wide association analysis demonstrated that tonsillectomy exhibited preventive effects on the development of physiological condition triggered delirium, acute myocardial infarction, and respiratory failure. Conversely, opposing effects were observed for the other 14 primary core outcomes (an incidence ≥1% in participants with tonsillectomy, P-value < .001, and a HR ≥ 1.10), including diseases affecting the nervous, immune, endocrine, auditory, respiratory, integumentary, and genitourinary systems. However, this comparison does not clarify whether the 17 primary core outcomes were attributable to tonsillectomy or to tonsillitis itself. To address this, we performed a secondary analysis among participants with tonsillitis. Of the 17 primary core outcomes, only depression showed a significant association with tonsillectomy. The lack of significance for the other primary core outcomes aligns with previous hypotheses that the increased diseases risks observed in participants undergoing tonsillectomy may stem from the effects of tonsillitis itself rather than from tonsillectomy.11,13 A recent cross-sectional study reported that tonsillectomy was robustly associated with a wide range of psychiatric disorders, including depression and suicidal behavior. 21 Besides, using 2-sample MR, we observed that the genetic susceptibility to tonsillectomy was also associated with depression. To further investigate the mechanisms behind this association, we included established risk factors for depression in the MVMR analyses. Although T2D did not diminish the estimated effect of tonsillectomy on depression risk, we observed partial mediation of this effect by BMI and smoking initiation. Furthermore, the results of the 4-way MVMR indicated no causal association between either tonsillectomy or tonsillitis and depression. Collectively, these findings suggested that while depression is clinically relevant, it is not causally associated with either tonsillectomy or tonsillitis.
IBS is conventionally regarded as a functional gastrointestinal disorder characterized by changes in bowel habits and recurrent abdominal pain. 22 Previous studies have demonstrated the crucial role of tonsils in generating mucosal immunity, with their absence potentially facilitating pathogen invasion into the gastrointestinal tract, leading to localized inflammation and gut dysbiosis.23,24 This association was further supported by a nationwide longitudinal population-based cohort study that found individuals who underwent tonsillectomy had a 1.84-fold increased risk of developing IBS compared to those who did not. 25 However, our results from the 4-way MVMR revealed a causal association between tonsillitis and IBS, rather than between tonsillectomy and IBS. A possible explanation for this discrepancy is that tonsillitis frequently occurs in individuals who have undergone tonsillectomy. Thus, the previously reported association between tonsillectomy and IBS in observational studies may be influenced by the underlying effects of tonsillitis. Therefore, our findings suggested a strong causal relationship between tonsillitis and IBS, while tonsillectomy alone might not be responsible for the development of IBS.
Additionally, given that there is currently no consensus on the optimal surgical age for tonsillectomy,26,27 we investigated the effects of age at surgery on the outcomes associated with tonsillectomy by modeling the nonlinear impacts of tonsillectomy. Our results suggested that the effects of tonsillectomy varied with age, with age 8 was identified as the turning point from risk-reducing to risk-increasing effects in our primary analysis. Although we identified age 56 as an additional turning point in the secondary analysis, this age threshold was inconsistent across disease outcomes and not replicated in primary analysis. Therefore, we suggested that age 8 might be the recommended age for tonsillectomy to minimize sequelae.
This large-scale population-based observational and MR study comprehensively explored the outcome-wide associations of tonsillectomy. However, several limitations warrant discussion. First, we defined tonsillectomy using both documented operation records and self-reported operation histories. These self-reported tonsillectomy histories may be subject to recall bias, particularly for surgeries performed in early childhood. While we used OPCS codes to supplement self-reports, residual misclassification remains possible. Second, we defined tonsillitis using ICD codes and self-reported doctor-diagnosed disease histories, which included chronic tonsillitis, hypertrophy of tonsils, and other nonneoplastic tonsil diseases. This broad definition may not fully capture the heterogeneity and severity spectrum of chronic tonsillitis and was an inherent problem of large-scale database like the UKB. Future studies with detailed phenotyping (e.g., biopsy records, detailed symptoms, and symptom durations) are needed to refine the associations we observed. Third, the statistical power was limited for analyses of less common disease outcomes, which might explain the absence of associations between these conditions and tonsillectomy. Fourth, genetic data was only available for a small portion of diseases, resulting in a limited number of outcomes included in our MR analysis for causal inference. Finally, as disease outcomes were primarily obtained from inpatient records and self-reported doctor-diagnosed disease histories, common mild diseases such as cold, were less likely to be included, leaving the impacts of tonsillectomy on these common mild diseases to be further investigated.
This large-scale population-based study comprehensively explored the associations between tonsillectomy and various disease outcomes, complementing conventional epidemiological research with causal inference through MR. Our findings highlighted the potential influence of tonsillitis, rather than direct causality of tonsillectomy, in explaining the observed clinical associations between tonsillectomy and multiple disease outcomes, revealing evidence for the safety of tonsillectomy.
Supplemental Material
sj-docx-1-ohn-10.1177_19160216261416896 – Supplemental material for Influence of Tonsillectomy on Various Disease Outcomes: An Outcome-wide Association Analysis and Mendelian Randomization Analysis
Supplemental material, sj-docx-1-ohn-10.1177_19160216261416896 for Influence of Tonsillectomy on Various Disease Outcomes: An Outcome-wide Association Analysis and Mendelian Randomization Analysis by Junhong Li, Ke Qiu, Ping An, Yuyang Zhang, Ziyan Zhang, Lan Feng, Shuo Li, Yanling Liang, Danni Cheng, Yufang Rao, Wendu Pang, Yao Song, Minzi Mao, Tao Shu, Xiuli Shao, Rong Yu, Yongbo Zheng, Wei Xu, Yu Zhao and Jianjun Ren in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Acknowledgements
We thank all participants in the UK biobank study and the members of the survey teams, as well as the project development and management teams. We also want to acknowledge the participants and investigators of the FinnGen study. The computations in this article were supported by the High Performance Computing platform at West China Biomedical Big Data Center, West China Hospital, Sichuan University.
Author Contributions
J.H.L., K.Q., and P.A. contributed equally to this work and are joint first authors. J.J.R., Y.Z., and W.X. contributed equally to this work and are joint senior authors. J.J.R., Y.Z., W.X., J.H.L., K.Q., and P.A. designed the study. Y.Y.Z., Z.Y.Z., L.F., S.L., Y.L.L., D.N.C., and Y.F.R. acquired the data. J.H.L., K.Q., X.L.S., and T.S. conducted the statistical analysis. J.H.L., K.Q., P.A., W.D.P., Y.S., M.Z.M., R.Y., and Y.B.Z. interpreted the results. J.H.L., K.Q., and P.A. wrote the first draft and all other authors had critically revised the manuscript. J.J.R., Y.Z., and W.X. are the guarantors of the manuscript and accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish. The corresponding authors attest that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Postdoctor Research Fund of West China Hospital, Sichuan University (QK, grant #2024HXBH111; RYF, grant #2023HXBH121); The Science and Technology Department of Sichuan Province (QK, grant #2024NSFSC1510; ZY, grant #2024YFHZ0076; RJJ, grant #2024YFHZ0335; CDN, grant #2024NSFSC1513; RYF, grant #2025ZNSFSC1528; SY, grant #2025ZNSFSC1530; PWD, grant #2025ZNSFSC1526); Chengdu Science and Technology Bureau (RJJ, grant #2024-YF05-00908-SN; ZY, grant #2024-YF05-00050-SN); West China Hospital, Sichuan University (ZY, grant #ZYJC21027); Sichuan University (PWD, grant #2023HXBH119); Health Care Research Project of Sichuan Province (ZY, grant#ZH2025-102); and The Foundation of National Clinical Research Center for Geriatrics (ZY, grant #Z2023LC002). The funders had no role in study design, in the collection, analysis and interpretation of data, in the writing of the report, or in the decision to submit the article for publication.
Ethics Approval
This study was performed under generic ethical approval obtained by UK Biobank from the North West Multi-centre Research Ethics Committee (MREC) (REC reference: 21/NW/0157, 29 June 2021).
Consent to Participate
All UK Biobank participants provided written informed consents at enrollment.
Data Availability Statement
UKB data are available in a public, open access repository. This research has been conducted using the UK Biobank Resource under Application Number 80787. The UK Biobank data are available on application to the UK Biobank (![]() ). The GWAS summary statistics for the following exposures and outcomes were utilized: tonsillectomy (the FinnGen study, data release 7), tonsillitis (the FinnGen study, data release 7), all asthma (PMID = 29273806), adult asthma (PMID = 30929738), child asthma (PMID = 30929738), allergic rhinitis ( MRC-IEU, ukb-b-16499/), Acute myocardial infarction (PMID = 33532862), depression (PMID = 30718901), Hypothyroidism (PMID = 36093044), Irritable bowel syndrome (PMID = 34741163), Migraine (MRC-IEU, ukb-b-16868/), Anxiety (PMID = 26754954), Pneumonia (PMID: 30104761), Sleep disorders (PMID: 30104761), Umbilical hernia (PMID = 35680855), Body mass index (PMID = 30239722), Smoke initiation (PMID: 36477530), and type 2 diabetes (the FinnGen study, data release 7).
). The GWAS summary statistics for the following exposures and outcomes were utilized: tonsillectomy (the FinnGen study, data release 7), tonsillitis (the FinnGen study, data release 7), all asthma (PMID = 29273806), adult asthma (PMID = 30929738), child asthma (PMID = 30929738), allergic rhinitis ( MRC-IEU, ukb-b-16499/), Acute myocardial infarction (PMID = 33532862), depression (PMID = 30718901), Hypothyroidism (PMID = 36093044), Irritable bowel syndrome (PMID = 34741163), Migraine (MRC-IEU, ukb-b-16868/), Anxiety (PMID = 26754954), Pneumonia (PMID: 30104761), Sleep disorders (PMID: 30104761), Umbilical hernia (PMID = 35680855), Body mass index (PMID = 30239722), Smoke initiation (PMID: 36477530), and type 2 diabetes (the FinnGen study, data release 7).
Supplemental material
Supplemental material for this article is available online.