
Abstract
Importance
Sudden sensorineural hearing loss (SSNHL) is often accompanied by vestibular dysfunction, yet the relationship between patterns of peripheral vestibular organ involvement and hearing prognosis requires systematic evaluation. Clarifying this association is essential for guiding clinical assessment and prognosis.
Objective
To explore the prognostic value of vestibular function tests in patients with SSNHL by assessing the functional status of peripheral vestibular receptors.
Design
Retrospective cohort study.
Setting
Inpatient departments of Jiaxing Second Hospital and the Hospital of the China Coast Guard (September 2020 to September 2021).
Participants
A total of 76 inpatients with unilateral SSNHL were enrolled and divided into a vertigo group (n = 29) and a non-vertigo group (n = 47).
Exposures or Interventions
All patients underwent pure-tone audiometry (PTA), cervical vestibular-evoked myogenic potentials (cVEMP), ocular VEMP (oVEMP), video head impulse test, and caloric testing to assess peripheral vestibular involvement.
Main Outcome Measures
Hearing recovery, defined by improvement in PTA thresholds.
Results
Patients with vertigo had significantly-worse baseline PTA thresholds compared with those without vertigo [67.91 ± 31.67 degrees of hearing loss (dBHL) vs 54.98 ± 29.03 dBHL, P = .001]. Vestibular dysfunction was common, most frequently involving semicircular canal lesions (49/76), followed by abnormal cVEMP (41/76) and abnormal caloric testing (39/76). Univariate analysis showed that cVEMP, oVEMP, and caloric testing results were significantly associated with treatment outcomes (all P < .001), with the combined assessment of oVEMP and caloric testing demonstrating particular prognostic value (P = .007). Multivariate logistic regression further identified vertigo (OR = 0.132), cVEMP abnormality (OR = 6.460), and oVEMP abnormality (OR = 0.147) as independent predictors of hearing prognosis (all P < .05).
Conclusion
Vestibular dysfunction reflects the extent of inner ear involvement in SSNHL, with semicircular canal impairment being the most common, followed by saccular and utricular lesions. Combined oVEMP and caloric testing appears to be an optimal approach for evaluating vestibular function and predicting hearing prognosis.
Relevance
This study supports the integration of multiple vestibular assessments to more comprehensively characterize inner ear involvement in SSNHL and to provide clinicians with reliable prognostic reference tools.

Key Points
Vestibular dysfunction is common in sudden sensorineural hearing loss (SSNHL), with semicircular canal impairment most frequent, followed by saccular and utricular involvement.
Abnormal oVEMP, cVEMP, and caloric test results are significant predictors of hearing prognosis, with oVEMP plus caloric test (CT) providing the strongest prognostic value.
Integrating multiple vestibular assessments enhances evaluation of inner ear involvement and offers clinicians a more reliable basis for prognosis in SSNHL.
Introduction
Sudden deafness, a prevalent condition affecting the inner ear, is characterized by an abrupt and unexplained sensorineural hearing loss of ≥20 degrees of hearing loss (dBHL) in at least 2 contiguous frequencies, manifesting suddenly and without a discernible cause within a 3-day period. 1 A previous study has indicated that 28% to 57% of patients experiencing sudden deafness also exhibit symptoms of vestibular involvement, such as vertigo, nausea, vomiting, and balance disturbances. 2 Conversely, certain patients with sudden deafness may either lack vertigo symptoms or present only mild dizziness during diagnosis, despite the presence of abnormal vestibular function. Another study has demonstrated a correlation between the prognosis of sudden deafness and the extent of inner ear damage, highlighting the increased challenge in achieving hearing restoration in patients concomitantly experiencing vertigo. 3 Consequently, there is heightened attention toward the assessment of vestibular function in patients with sudden deafness. 4
The vestibular system exhibits frequency-specific characteristics, with a wide frequency range covered by its components. Different tests were used to assess relevant functions within various frequency ranges. Comprised of 3 semicircular canals (horizontal, anterior, and posterior) and 2 otolithic organs (utricle and saccule), the vestibular receptors determine the system’s frequency response. The spontaneous discharge characteristics of hair cells and their arrangement within the ampullary crests of the semicircular canals dictate the vestibular frequency response. In the present study, we comprehensively employed a combination of various tests encompassing pure-tone audiometry (PTA), caloric test, cervical vestibular-evoked myogenic potential (cVEMP), ocular vestibular-evoked myogenic potential (oVEMP), and video head-impulse test (vHIT) to assess the vestibular damage extent in patients with sudden sensorineural hearing loss (SSNHL). We aimed to elucidate the relationship between vestibular impairment and hearing prognose and therefore providing valuable clinical insights in patients with sudden deafness.
Materials and Methods
Study Participants
The study participants consisted of 76 patients with unilateral SSNHL who were admitted to the Second Hospital Affiliated to Jiaxing College and the China Coast Guard Hospital of the Armed Police Force from September 2020 to September 2021. The inclusion criteria were based on the diagnosis and treatment guidelines (2015) for sudden deafness, with a consultation time ranging from 1 to 14 days after onset. 1 Patients were excluded if they present with abnormal conditions, such as external middle ear diseases, central nervous system disorders, and acoustic neuroma, or they already met the diagnostic criteria for definite Ménière’s disease or had a history of typical recurrent vertigo at the time of enrollment.
Research Method
Conventional therapy following admission
The guidelines for various types of sudden deafness issued by the Chinese Medical Association were adhered to in the treatment of all patients, with a treatment cycle lasting for 10 days. 1 Systemic administration of glucocorticosteroids was prioritized, alongside interventions aimed at enhancing blood circulation, dilating blood vessels, and nourishing nerves. For patients experiencing total deafness, the additional administration of Batroxobin was recommended. Pure-tone hearing thresholds were reassessed upon the completion of the initial treatment course and again following 1 month of consecutive treatment. The results of these assessments were used to ascertain the efficacy of the treatment.
The cases were primarily managed by otolaryngologists. For patients presenting with significant vestibular symptoms, neurologists were also consulted and involved in joint management.
Audiological examination and efficacy assessment
Prior to treatment, all patients underwent PTA using the Corina audiometer. Pure-tone audiograms were obtained, and the average hearing threshold of patients was calculated. All pure-tone audiometric examinations were performed in a standard soundproof booth by certified audiologists with extensive clinical experience. Based on the frequency and severity of sudden deafness, the following categories were established: high-frequency descending type, low-frequency ascending type, flat descending type, and total deafness type. The low-frequency ascending type was characterized by a hearing loss at frequencies of 1000 Hz or lower, with a loss of at least 20 dBHL at 250 and 500 Hz. The high-frequency descending type involved a hearing loss at frequencies of 2000 Hz or higher, with a loss of at least 20 dBHL at 4000 and 8000 Hz. The flat descending type exhibited a decrease in hearing at all frequencies, with an average threshold of 250 to 8000 Hz (250, 500, 1000, 2000, 3000, 4000, 8000 Hz) ≤80 dBHL. The total deafness type featured a decrease in hearing at all frequencies, with an average threshold of 250 to 8000 Hz (250, 500, 1000, 2000, 3000, 4000, 8000 Hz) ≥81 dBHL. 5 Hearing efficacy was determined by subtracting the average posttreatment hearing threshold from the average pretreatment hearing threshold. If there was no response even when a frequency exceeded the maximum output of the instrument, a threshold of 120 dBHL was used for threshold estimation to calculate the average threshold. Criteria for assessment included the following: recovery, where the threshold of the affected frequency returned to normal, or reached the level of the healthy ear, or reached the level before the current illness; significant improvement, where the average hearing at the affected frequency increased by more than 30 dB; effective, where the average hearing at the affected frequency improved by 15 to 30 dB; and ineffective, where the improvement in average hearing at the affected frequency was less than 15 dB. 1
Vestibular function examination
Vestibular function examinations were conducted for all patients, encompassing caloric test using the International Hearing Hot and Cold Stimulator, cVEMP and oVEMP assessed with the International Hearing Auditory Evoked Potential Analyzer (Eplice; Interacoustics A/S, Middelfart, Denmark), and vHIT performed using the International Hearing OtoAccess™ v.1.5 system in conjunction with EyeSeeCam (Interacoustics A/S, Middelfart, Denmark). Both cVEMP and oVEMP were elicited using air-conducted sound stimuli delivered via insert earphones.
All vestibular function examinations (including caloric testing, cVEMP, oVEMP, and vHIT) were performed by certified audiologists with extensive professional experience. We have supplemented this information in the Materials and Methods section. To accurately assess vestibular function in the early stage of onset, all vestibular function tests were performed after hospital admission but before the initiation of systemic pharmacological treatment. The time interval between vestibular testing and the initial audiological assessment was generally within 24 to 48 hours.
The caloric test was conducted using the international vestibular video-nystagmography system and a hot-cold air stimulation device. Subjects were placed in a supine position with a 30° forward tilt of the head to bring the horizontal semicircular canals (HSC) into a vertical position for hot and cold air irrigation. The stimulation sequence involved hot air (50°C) followed by cold air (24°C), with 4 irrigations performed bilaterally. The single-side canal paralysis (CP) was calculated using the Jongkee formula, where CP = [(RW + RC) − (LW + LC)]/(RW + RC + LW + LC) × 100%, with R and L representing the right and left sides, respectively, and W and C representing hot and cold air, respectively, and the slow-phase velocity of the stimulation was calculated. Analysis of the results showed that a CP value >25% indicated unilateral weakness, while bilateral weakness was defined as total responses in both ears during cold or hot irrigation <12°/s, that is, RC + RW < 12°/s and LC + LW < 12°/s (with the slow-phase velocity of RC, RW, LC, LW being taken as absolute values).
For cVEMP testing, the international auditory evoked potential analysis system (Eplice; Interacoustics A/S, Middelfart, Denmark) was used. Participants were seated upright, and surface electrodes were placed after skin preparation. During the examination, they were instructed to rotate their head to one side and maintain tonic contraction of the sternocleidomastoid muscle, as guided by a visual feedback bar (kept within the green zone). Real-time electromyographic monitoring was used to ensure that muscle activation consistently reached the preset threshold, and participants maintained this isometric contraction until stimulation on that side was completed. Electrodes were placed after cleaning the local skin, with interelectrode resistance less than 5 kΩ. The recording electrodes were placed in the upper segment of the sternocleidomastoid muscle on both sides, with reference electrodes placed on both sides of the manubrium and the ground electrode placed between the eyebrows. During testing, subjects were instructed to turn their heads to one side to tense the sternocleidomastoid muscle and maintain a certain duration of isometric contraction, and the sound was delivered monaurally via insert earphones. cVEMP exhibited positive (P13 or P1) and negative (N23 or N1) waves at around 13 and 23 ms, respectively.
For oVEMP testing, subjects were seated, and electrodes were placed below the midpoint of the lower margin of the orbit, with the reference electrode placed 1.5 to 2.0 cm below and lateral to it, and the ground electrode placed between the eyebrows. Subjects were instructed to focus on a target located 30° above the midline of their visual field, and sound was delivered to the contralateral side via insert earphones. oVEMP exhibited negative (N10 or N1) and positive (P15 or P1) waves at around 10 and 15 ms, respectively. The peak-to-peak amplitude and interaural asymmetry ratio (IAR) were calculated for both cVEMP and oVEMP measurements, where IAR = |amplitude of the right ear − amplitude of the left ear|/|amplitude of the right ear + amplitude of the left ear|. Typical waveform disappearance or an absolute value of IAR >0.29 or a ratio of amplitudes ≥1.61 indicated involvement of the otolith organ and/or vestibular nerve. cVEMP was used to examine the function of the saccule and the inferior vestibular nerve, while oVEMP was used to assess the function of the utricle and the superior vestibular nerve.
HIT examination was performed using the international auditory OtoAccess™ v.1.5 (EyeSeeCam; Interacoustics A/S, Middelfart, Denmark) head-impulse test device for 3-dimensional vHIT examination. Prior to vHIT testing, patients with a known history of severe cervical spondylosis were excluded to avoid limitations in cervical mobility. During the test, examiners confirmed adequate cervical range of motion by monitoring both the tactile feedback and the patient’s tolerance, while also verifying that each head impulse achieved sufficient angular velocity (>150°/s) and excursion on the velocity-time trace. Trials that did not meet these criteria were discarded, thereby ensuring the validity of the stimuli and the reliability of the results. Subjects were seated and instructed to focus on a target located 1.5 m directly in front of them at eye level. The operator stood behind the subject, supporting their head, and performed more than 20 high-speed, high-acceleration, small-amplitude, irregular head impulses (amplitude 10° to 15°, peak angular velocity 100° to 250°/s) in horizontal and RALP/LARP plans. Eye movement and head angular velocity were recorded, and the program automatically calculated the gain of the deviation (vHIT-G), where gain = (eye movement velocity/head movement velocity) × 100%, and the mean gain of the 6 semicircular canals was recorded. The normal range of gain for the HSC was 0.8 to 1.2, while for the anterior (ASC) and posterior (PSC) semicircular canals, it was 0.7 to 1.2. The criteria for defining abnormal vHIT results were as follows: HSC vestibulo-ocular reflex (VOR) gain <0.8, anterior or posterior semicircular canal VOR gain <0.7, and/or the presence of corrective saccades with a peak velocity >100°/s, indicating dysfunction of one or more semicircular canals.
Statistical Methods
Data analysis was performed using the SPSS 22.0 software (IBM Corporation, Armonk New York State, USA). Normality testing was conducted for measurement data, with normally distributed data presented as mean ± standard deviation and subjected to analysis of variance. Non-normally-distributed data were expressed using the median and interquartile range. Categorical data were represented as numbers and percentages. Treatment effects between groups were compared using the chi-squared test. The correlation between normal vestibular function and treatment effects was assessed through Spearman’s rank analysis. Clinical characteristics of patients were compared based on pretreatment hearing levels using either the chi-squared test or the Kruskal-Wallis H-test. The Mantel-Haenszel trend test was used to assess trends in categorical variables. Multifactorial logistic regression was used to evaluate the effect of vestibular function tests on hearing prognosis. A P-value less than .05 was considered statistically significant.
Results
Clinical Information
A total of 76 patients diagnosed with SSNHL and possessing complete datasets were included in the study. The group consisted of 32 males (42.1%) and 44 females (57.9%), with ages ranging from 19 to 75 years (47.86 ± 11.94). Among them, 45 cases presented left ear lesions (59.2%), while 31 cases exhibited right ear lesions (40.8%). Notably, 29 cases (38.2%) reported experiencing vertigo, while 47 cases (61.8%) did not. The duration from onset to consultation spanned from 1 to 14 days, with an average of 4.05 ± 3.32 days, and the mean interval between treatment and audiogram assessment was 30.25 ± 4.35 days.
Localization of Inner Ear Damage
All patients underwent baseline PTA and a comprehensive vestibular function test battery immediately after hospital admission and before the initiation of any systemic pharmacological treatment. Standard treatment was then commenced. At 1 month after treatment initiation, follow-up PTA was performed to evaluate hearing outcomes. Anomalies in caloric test and vHIT were categorized as abnormal semicircular canal function, while abnormal cVEMP indicated impaired saccular function, and abnormal oVEMP signified compromised utricular function. In this study, there were 49 cases with semicircular canal damage, 41 cases with saccular damage, and 38 cases with utricular damage. Among these, 29 cases exhibited both utricular and saccular damage, while 15 cases demonstrated normal vestibular function, indicating a predominance of vestibular organ impairment among the patients. Regarding vHIT results, the PSC was found to be the most vulnerable (18 cases), followed by the HSC with 17 cases and the ASC with 14 cases. There were no statistically-significant differences observed in the rates of abnormality among vestibular function tests for PSC, ASC, and HSC when comparing the vertigo and non-vertigo groups (P = .065). Refer to Table 1 for a detailed breakdown.
Comparative Analysis of the Abnormal Rate of Vestibular Function Results Between the 2 Groups (%, Cases).
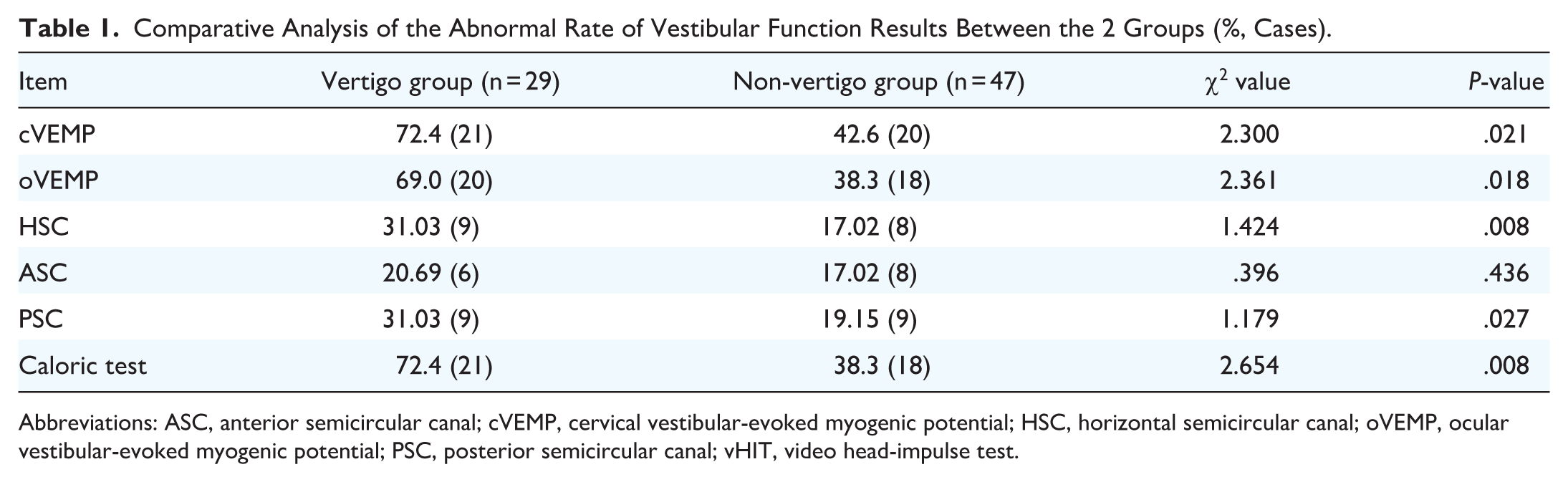
Abbreviations: ASC, anterior semicircular canal; cVEMP, cervical vestibular-evoked myogenic potential; HSC, horizontal semicircular canal; oVEMP, ocular vestibular-evoked myogenic potential; PSC, posterior semicircular canal; vHIT, video head-impulse test.
Relationship Between Hearing Prognosis and Vestibular Symptoms in Patients Diagnosed with Sudden Deafness
Patients experiencing vertigo exhibited a notably-higher mean initial PTA and posttreatment PTA than those without vertigo (67.91 ± 31.67 vs 46.10 ± 22.60 dBHL; 54.98 ± 29.03 vs 30.65 ± 20.52 dBHL). A statistically-significant difference in pretreatment hearing levels was observed between the vertigo and non-vertigo groups (P = .001). The severity of hearing loss was more pronounced in the vertigo group, with 55.2% experiencing severe hearing loss, compared with 23.4% in the non-vertigo group (P = .002). Furthermore, the treatment efficacy differed between the 2 groups, with the non-vertigo group exhibiting higher efficacy than the vertigo group (P = .003). Refer to Table 2 for detailed information.
Relationship Between Vestibular Symptoms and Efficacy in Patients Diagnosed with Sudden Deafness [% (Cases)].

Relationship Between Efficacy and Vestibular Function in Patients Diagnosed with Sudden Deafness
Hearing recovery was categorized as complete in 40.8% (31/76) of patients, partial in 22.4% (17/76), and absent in 36.8% (28/76). The association between individual vestibular test results (cVEMP, oVEMP, caloric test) and treatment efficacy is detailed in Table 3. A comparative analysis of vestibular function combinations revealed that only the co-occurrence of abnormal oVEMP and caloric test results was significantly associated with a higher rate of treatment failure (P = .007, χ2 = 7.743). In contrast, the combinations of abnormal cVEMP and oVEMP P = .991), cVEMP and caloric test (P = .570), and cVEMP, oVEMP, and caloric test (P = .826) showed no significant association with treatment outcomes.
Association Between Vestibular Test Results and Treatment Outcome.

Data are presented as number of cases (percentage). P-values were calculated using the chi-squared test to compare treatment outcomes between groups with normal and abnormal test results.
Abbreviations: cVEMP, cervical vestibular-evoked myogenic potential; oVEMP, ocular vestibular-evoked myogenic potential; vHIT, video head-impulse test.
Among patients with abnormal oVEMP and caloric test, the treatment inefficiency for sudden deafness was 65.7%. For patients with abnormal oVEMP and cVEMP, the treatment inefficiency was 51.5%, and for those with abnormal caloric test and cVEMP, the treatment inefficiency was 61.5%.
A significant correlation was identified between normal vestibular function test results and the restoration of hearing (Z = −3.961, P < .001). When the efficacy was categorized into 3 levels—recovered, effective, and ineffective—among patients with normal vestibular function test results, the effective rate reached 86.7%. Notably, as the number of abnormal vestibular function items increased, the effective rate decreased, and this difference was statistically significant (P = .009, t = 0.851). Refer to Table 4 for detailed information.
Treatment Effective Rate Stratified by the Number of Abnormal Vestibular Test Items.

Trend analysis showed that treatment efficacy significantly decreased with an increasing number of abnormal test items (P = .009).
Treatment efficacy was calculated as: (recovered + significant improvement + effective) ÷ total number of patients × 100.
Multifactorial Logistic Regression Analysis of Efficacy in Patients Diagnosed with Sudden Deafness
The construction of the multifactorial logistic regression equation incorporated caloric test, cVEMP, oVEMP, vHIT, vertigo symptoms, age, and sex. The results revealed that the absence of vertigo symptoms, normal cVEMP, and normal oVEMP were identified as independent factors and positive predictors of a favorable prognosis in patients with sudden deafness. Conversely, age, caloric test, and vHIT were not found to be significantly associated with the prognosis. Further details can be found in Table 5.
Outcomes of a Logistic Multivariate Regression Analysis.

The reference categories were normal CT, normal cVEMP, normal oVEMP, normal vHIT, no vertigo. Sex was referenced as female.
Abbreviations: CI: confidence interval; CT, hot/cold test; cVEMP, cervical vestibular-evoked myogenic potential; OR, odds ratio; oVEMP, ocular vestibular-evoked myogenic potential; vHIT, video head-impulse test.
Indicates that a difference was considered statistically significant when the P-value was less than .05.
Discussion
Numerous studies have reported abnormal vHIT results in patients with SSNHL.4,6-11 In the present study, it was observed that not all patients exhibiting varying degrees of vestibular dysfunction reported vertigo symptoms. 12 Conversely, patients presenting with vestibular symptoms did not consistently manifest abnormalities in vestibular function during instrumental testing. 13 Within the vertigo group, 86.2% of patients with sudden deafness demonstrated vestibular dysfunction, while the remaining 13.8% exhibited normal results across all vestibular function tests. This finding suggests that the presence of vertigo symptoms may not consistently correspond to detectable vestibular dysfunction at the time of testing nor fully reflect the extent of inner ear involvement, given the potential for rapid recovery, compensation, or episodic disease manifestations.
In this study, we found that not all patients with varying degrees of vestibular dysfunction reported vertigo. Conversely, patients with vestibular symptoms did not always exhibit vestibular dysfunction in instrumental tests. In the vertigo group of this study, 86.2% of sudden deafness patients had vestibular dysfunction, while the remaining 13.8% had normal results in all vestibular function tests, indicating that vertigo symptoms in sudden deafness patients do not accurately indicate the presence of vestibular dysfunction or the extent of inner ear damage. Therefore, in clinical practice, patients with sudden deafness should undergo vestibular function testing in addition to hearing assessment. Consistent with the findings of Cohen et al, 12 our results suggest that patients presenting with cochleo-vestibular symptoms should undergo a comprehensive diagnostic assessment that includes not only standard audiological testing but also dedicated vestibular function evaluations.
In this study, the comprehensive assessment of the entire inner ear function in the 76 patients involved PTA, oVEMP, cVEMP, caloric test, and vHIT. PTA assessed cochlear function, oVEMP assessed utricle function, cVEMP examined sacculus function, caloric test appraised HSC function, and vHIT scrutinized functions of all semicircular canals. These examinations collectively provided a nuanced assessment of the extent of inner ear damage in patients with sudden deafness.13,14 The findings indicated that semicircular canal damage was the most prevalent, followed by damage to saccule and utricle. In patients experiencing vertigo, caloric test and cVEMP examinations exhibited the highest percentage of abnormal vestibular function. Notably, caloric test abnormalities were significantly correlated with disease severity (P = .001). The elevated percentage of caloric test abnormalities in patients with vertigo and severe hearing loss indicated a wider range of vestibular damage, particularly semicircular canal damage. Furthermore, there was a higher likelihood of simultaneous involvement of the cochlea, otolith organ, and semicircular canal. 15 Interestingly, 38.3% of patients in the non-vertigo group also displayed abnormal caloric test, indicating the presence of semicircular canal damage. Past research has indicated that abnormal caloric test results may lead to a poor hearing prognosis, potentially attributable to microcirculatory disorders or severe, irreversible hearing loss induced by viral factors. 16 However, the capability of caloric test is limited to assessing the very low-frequency vestibulo-ocular reflex function of the HSC, whereas vHIT can assess the high-frequency vestibulo-ocular reflex function of the 3 semicircular canals.15,17 A combined approach using both tests can offer a more comprehensive assessment of semicircular canal function. Patients with sudden deafness and vertigo exhibited semicircular canal damage at both low and high frequencies, aligning with previous conclusions by Zhang et al. 18 Contrary to a meta-analysis indicating the utriculus as the most susceptible to damage in sudden deafness, results from our study indicated that the rate of abnormality in cVEMP examinations was highest in patients with sudden deafness, regardless of the presence of vertigo. 19 This was followed by caloric test and oVEMP, implying a higher likelihood of impairment in sacculus function. Anatomically, the saccule is proximate to the cochlea. We postulate that vestibular dysfunction in sudden deafness may arise from the involvement of vestibular organs in close proximity to the cochlea. Alternatively, the manifestation of sudden deafness may entail distinct patterns of damage, contingent upon underlying etiological factors. In this study, we observed that the saccule (as indicated by abnormal cVEMP responses) appeared to be more vulnerable, which differs from the conclusion of Chen et al, 20 who suggested that the utricle is most commonly affected. This discrepancy may be related to the specific characteristics of inner ear blood supply. The labyrinthine artery is the main vessel supplying the inner ear, with its branches—the anterior vestibular artery and the posterior vestibular (or vestibulocochlear) artery—supplying the upper vestibular structures (including the utricle, superior semicircular canal, and HSC) and the lower vestibular structures (including the saccule and posterior semicircular canal), respectively. Differences in the sensitivity or susceptibility of these vascular branches to ischemic events may therefore underlie the varying patterns of peripheral vestibular organ involvement. This hypothesis is supported by classical anatomical studies, which have demonstrated a clear regional distribution in the vascular supply of the inner ear.
In this study, the relationship between vestibular function damage and treatment efficacy was analyzed, revealing statistical significance for cVEMP, oVEMP, and caloric test findings. In a 2-by-2 comparative analysis, only the combination of oVEMP and caloric test testing demonstrated statistical significance for efficacy (P = .007, χ2 = 7.743). Among patients with sudden deafness exhibiting abnormalities in both oVEMP and caloric test, 65.7% experienced ineffective treatment. We hypothesize that patients displaying normal oVEMP and caloric test results are more likely to have restorable hearing. The vestibular labyrinth consists of 5 receptor structures, with the saccule being the closest to the cochlea, followed by the utriculus and the HSC. Some scholars have categorized sudden deafness into various types, including cochlea type, cochlear saccule type, cochlear utricle type, cochlea and external semicircular canal type, and different combined types. 21 We further hypothesize that the refinement of inner ear damage in sudden deafness through combined VEMP and audiometry may hold significance for hearing prognosis. A more limited extent of inner ear lesion is postulated to correspond to a better prognosis, and conversely, a more extensive lesion correlates with a poorer prognosis. The utriculus and the HSC are situated furthest from the cochlea, and simultaneous involvement of the cochlea, otolith organs, and semicircular canal is indicative of a less favorable prognosis.22,23
Patients diagnosed with sudden deafness and concurrent vertigo exhibited more severe hearing loss than those without vertigo. Multifactorial logistic regression analysis focusing on hearing recovery indicated a higher likelihood of vestibular dysfunction in patients with vertigo, particularly dysfunction of the saccule and utriculus. Among these factors, saccule dysfunction exerted the most significant impact on hearing prognosis, consistent with recent studies. 21 Conversely, sex, age, and vHIT were not identified as associated factors with hearing prognosis in sudden deafness. Notably, the lack of a correlation between age and hearing prognosis contradicts some prior research results, where age was deemed a crucial prognostic factor in sudden deafness.24,25 The divergence in results may be attributed to the relatively-limited sample size in our study. Furthermore, a correlation analysis examining the number of abnormalities in vestibular function test items and the effective rate of hearing recovery confirmed a significant association between incomplete hearing recovery and damage to vestibular receptors. 18 The group without vestibular involvement demonstrated a significantly-higher hearing recovery rate. The assessment of the vestibular system also proved valuable in predicting hearing prognosis in patients without vertigo, which is consistent with a previous study. 19
According to the vast majority of the most recent investigations,7-9,11,12 PSC represents the most-frequently-involved SC in SSNHL, in particular when acute vertigo accompanies SSNHL. The discrepancy between our findings and theirs may be attributed to differences in vestibular assessment methods. While most prior studies have primarily relied on the video head-impulse test (vHIT), our study incorporated both caloric testing and vHIT for a more comprehensive evaluation. Caloric testing is particularly sensitive to low-frequency HSC function, which may explain the higher rate of horizontal canal abnormalities observed in our cohort, suggesting that low-frequency vestibular dysfunction might be more prevalent in this patient population. Although the absolute number of horizontal canal lesions was the highest in our study, no statistically-significant differences were found among the 3 semicircular canals. This indicates that canal involvement in our cohort may have been more diffuse rather than predominantly localized to a single canal. Additionally, the relatively-limited sample size of our study may have reduced our ability to detect subtle but statistically-significant distribution patterns.
There are certain limitations to this study. Firstly, the relatively-small sample size of patients restricts the robustness of regression analysis. Secondly, the retrospective nature of the study design introduces the potential for both selection bias and information bias. Future investigations should encompass more extensive fundamental and clinical research, involving large-scale multicenter prospective studies to validate and extend the findings of this study. Lastly, despite our efforts to exclude Ménière’s disease, a 1-month follow-up may not be sufficient to fully distinguish low-frequency SSNHL from the early-stage of Ménière’s disease. Longer follow-up studies will be needed in the future to better characterize the differences between these 2 patient groups.
Conclusions
In conclusion, a combined assessment of vestibular end organ function proves valuable for providing a comprehensive assessment of inner ear damage in patients with sudden deafness, thereby enhancing the understanding of hearing prognosis. Among the various vestibular function tests employed for patients with sudden deafness, cVEMP exhibits the highest abnormality rate, followed by caloric test and oVEMP. An abnormal cVEMP test may serve as an indicator of poorer hearing recovery.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Jiaxing Science and Technology Program (2020AD30133).
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. This study was conducted with approval from the Ethics Committee of The Second Hospital Affiliated to Jiaxing College and the China Coast Guard Hospital of the Armed Police Force (Approval No.: JXEY-2022SW026, Helen 202065). A written informed consent form was obtained from all participants.