
Abstract
Importance
Dizziness/vertigo is a common symptom that can lead to falls and reduced confidence in daily activities. It can result from vestibular, non-vestibular, or unidentified etiologies. Effective treatments with minimal side effects are essential to improving patient outcomes.
Objective
To compare the efficacy and safety of Ginkgo biloba extract EGb 761® with Betahistine in patients with dizziness/vertigo of unclear etiology.
Study Design
Randomized, double-blind, controlled trial conducted from October 2022 to August 2023.
Setting
Ear, Nose, and Throat Outpatient Department at Burapha Hospital.
Participants
Eighty-six individuals aged ≥20 with dizziness/vertigo lasting >1 month without a specific etiology.
Intervention
Patients were randomized to EGb 761® (120 mg/day) or Betahistine (36 mg/day) with matched placebos for 12 weeks, assessed at weeks 2, 6, and 12.
Main Outcome Measures
Primary outcome: change in dizziness severity as assessed by the 11-Point Box Scale and Dizziness Handicap Inventory (DHI) scores. Secondary outcomes: safety.
Results
Repeated-measures ANOVA showed significant improvement over time in both groups (P < .001), with no group × time interaction, indicating comparable efficacy. For DHI, Betahistine showed a transient advantage at week 2 (P < .01, Cohen’s d = 0.96), but no significant difference between treatments was observed at week 12. Both treatments were well tolerated, with only mild gastrointestinal side effects.
Conclusion
EGb 761® and Betahistine demonstrated comparable efficacy and good safety in treating dizziness or vertigo of unclear etiology. Clinical improvement was most evident within the first 2 weeks of therapy.
Relevance
EGb 761® is a safe and effective alternative to Betahistine with comparable efficacy and good tolerability.

Keywords
Key Message
Both EGb 761® (120 mg/day) and Betahistine (36 mg/day) effectively reduced dizziness symptoms, with marked improvement within 2 weeks.
Introduction
Dizziness refers to sensations such as lightheadedness or unsteadiness, while vertigo denotes a false perception of motion, typically spinning.1,2 According to the GRACE-3 classification, acute dizziness and vertigo can be categorized into acute vestibular syndrome (AVS), spontaneous episodic vestibular syndrome (s-EVS), triggered EVS (t-EVS), and isolated dizziness. 3 The most common etiology of dizziness and vertigo is otologic (peripheral), followed by neurological (central) causes, 4 with 8.2% 5 to 22% 6 of cases having no specific diagnosis. In a 2010 Thai study of 547 ENT outpatients, 72.9% had peripheral vertigo and 26.1% had unclear etiology. 7
Management of dizziness and vertigo involves both non-pharmacological approaches, such as vestibular rehabilitation, and pharmacologic therapy. Betahistine is the most frequently prescribed drug, acting as a histamine H1-receptor partial agonist and H3-receptor antagonist in the inner ear. 8 This mechanism enhances endolymph reabsorption and lowers labyrinthine pressure, improving tinnitus and vertigo in Meniere’s disease. 9 The effectiveness of Betahistine on vertigo is good according to meta-analysis studies.10,11 Adverse effects are uncommon and generally mild, such as bloating or dyspepsia, allowing most patients to complete therapy.
EGb 761®, a standardized extract of Ginkgo biloba leaves containing 24% flavonoids, 6% triterpenes, and <5 ppm ginkgolic acid, improves cerebral and inner ear perfusion by dilating small vessels and reducing blood viscosity. 12 It also exerts neuroprotective effects13 -15 by reducing apoptotic activity, reducing oxidative stress in neuronal mitochondria,16,17 and prevention of oxidative hemolysis. 18 However, studies on the use of EGb 761® for the treatment of dizziness/vertigo are still limited, and most studies have included participants with coexisting dementia.19,20
Objectives
To evaluate the efficacy and safety of EGb 761® versus Betahistine in patients with dizziness or vertigo of unclear etiology.
Methods
Study Design and Setting
This prospective randomized double-blind controlled trial was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Burapha University, approval number, HS045/2565.
Sample Size Calculation
This non-inferiority trial compared EGb 761® with Betahistine. The sample size was calculated using the non-inferiority formula described by Chow et al. 21 The difference between mean change in dizziness/vertigo symptoms, over a 12 week period, was evaluated by an 11-point numeric analog scale in the EGb 761® group (mean = 3.5 point) 22 and Betahistine group (mean = 3.3 points), 22 with margin of error ≤1.3 points. The standard deviation was 1.8 points, 22 and significance level was 0.05 and power of test was 80%. Based on this calculation, a total of 34 subjects per group was required. To account for a potential dropout rate of 20%, the sample size was increased to 43 participants/group, resulting in a total of 86 participants.
Participants
For the inclusion criteria, patients aged 20 years and older, both male and female, presenting with dizziness/vertigo without specific etiology, with symptoms lasting longer than 1 month and severity of dizziness/vertigo symptoms before treatment, assessed using the 11-Point Box Scale, had to be >3 points, were eligible. Participants were recruited from the Department of Otorhinolaryngology, Burapha University Hospital, between October 2022 and August 2023. Exclusion criteria included identifiable causes of dizziness/vertigo such as acute stroke, cognitive impairment, gait unsteadiness, vestibular migraine, cardiac arrythmia, benign paroxysmal positional vertigo (BPPV), Ménière’s disease, vestibular neuritis, labyrinthitis, sudden sensorineural hearing loss with vertigo, drug or medication toxicity, anemia, chronic kidney disease, history of allergy to EGb 761® or Ginkgo leaves or Betahistine, gastrointestinal diseases affecting drug absorption, and severe, uncontrolled chronic diseases.
Intervention
All patients who meet the inclusion criteria and provide informed consent will undergo a comprehensive medical history review, ear, nose, and throat examination along with a neurological evaluation. Cognitive function was screened using mini-mental state examination and montreal cognitive assessment, and patients with impairment were excluded. Gait steadiness was assessed by Romberg and tandem gait tests. For patients presenting with AVS, the head impulse, nystagmus, test of skew (HINTS) exam will be performed, with an additional audiological evaluation if hearing loss is present. If a central cause is suspected, the patient will be referred to a neurologist and excluded from the study. Patients with s-EVS suspected of having vestibular migraine or Ménière’s disease will be excluded from the study. Patients with t-EVS underwent Dix-Hallpike or supine roll testing to exclude BPPV. All participants will undergo laboratory tests, including CBC, BUN, creatinine, fasting blood sugar, and EKG, to rule out other potential causes of dizziness/vertigo.
Eligible patients were randomly assigned to 2 treatment groups using computer-generated randomization. The first group will receive 120 mg of EGb 761® once daily after breakfast, along with a dummy pill (no active ingredient) identical in appearance to Betahistine, taken 3 times daily after breakfast, lunch, and dinner. The second group will receive 12 mg of Betahistine 3 times daily after breakfast, lunch, and dinner, along with a dummy pill (no active ingredient) identical in appearance to EGb 761®, taken once daily after breakfast. Both groups’ medications will be packaged in opaque sealed envelopes. This method ensures blinding for both the patients and investigators.
Outcomes were assessed using 2 validated self-report tools: (1) the 11-Point Box Scale, rating dizziness severity from 0 (no dizziness/vertigo) to 10 (the worst dizziness/vertigo imaginable), and (2) the Thai version of the Dizziness Handicap Inventory (DHI23,24), which consists of 25 questions divided into 3 categories: 9 questions assessing emotional impact, 9 questions assessing functional impact, and 7 questions assessing physical impact. The total possible score is 100 points, with the scoring as follows: “Yes” (4 points), “No” (0 point), and “Sometimes” (2 points). Higher scores indicate greater impacts of dizziness on the patient’s quality of life.
Patients were followed for 12 weeks, with assessments at baseline (week 0) and weeks 2, 6, and 12. During each follow-up visit, patients completed the 11-Point Box Scale, the DHI, the number of unscheduled emergency department (ED) visits for dizziness/vertigo, and a questionnaire on medication side effects.
Statistical Analysis
Quantitative variables (eg, age, symptom duration, number of ED visits) were summarized as mean ± SD, and categorical variables (eg, sex, diagnosis, comorbidities, drug allergies, medications, side effects) as frequencies and percentages.
Inferential analyses compared dizziness severity using the 11-Point Box Scale. Within-group differences were assessed with paired t-tests or Wilcoxon signed-rank tests, and between-group differences with unpaired t-tests or Mann-Whitney U tests. Statistical significance was set at P < .05.
DHI category changes were analyzed using Wilcoxon signed-rank tests, and end-of-study proportions were compared between groups using chi-square tests. Statistical significance was set at P < .05.
Results
Of 104 screened patients, 86 were enrolled and evenly randomized to EGb 761® and Betahistine groups (n = 43 each). One patient in the EGb 761® group was lost to follow-up without providing a reason. In the Betahistine group, a male patient aged 80 years passed away due to a coronavirus infection complicated by respiratory failure during week 8 of treatment. Notably, this patient did not report any adverse effects related to Betahistine during follow-up. The detailed study process is illustrated in the CONSORT diagram (Figure 1 and Supplemental Material).

Consolidated standards of reporting trials flowchart showing the participant enrollment, randomized allocation, follow-up, and data analysis.
A total of 84 patients completed the study (42/group). Baseline characteristics, including sex, age, duration of dizziness, allergies, and comorbidities, did not differ significantly between groups. Adverse events occurred in 4 patients (9.5%) per group: in the EGb 761® group, dyspepsia/heartburn (n = 4) and constipation (n = 1); in the Betahistine group, dyspepsia/heartburn (n = 3) and insomnia (n = 1). Unscheduled ED visits for dizziness/vertigo were significantly lower in the EGb 761® group than in the Betahistine group (2.7 ± 1.1 vs 4.5 ± 1.4; P = .03; Table 1).
Baseline Demographic and Clinical Characteristics (n = 84).

P < .05 considered statistically significant.
Chi-square test.
Unpaired t-test.
Within the experimental groups, both EGb 761® and Betahistine groups showed significant improvement in dizziness/vertigo over 12 weeks. In the EGb 761® group, the 11-Point Box Scale decreased from 6.5 ± 1.6 to 2.1 ± 1.2 (P < .01), and DHI from 63.7 ± 17.0 to 29.0 ± 18.3 (P < .01). In the Betahistine group, scores declined from 6.4 ± 1.0 to 2.2 ± 1.9 (P < .01) and from 54.3 ± 16.9 to 21.3 ± 20.2 (P < .01), respectively. The greatest reduction occurred within the first 2 weeks, followed by gradual improvement through week 12 (Table 2 and Figure 2A and B).
Within-Group Comparison of 11-Point Box Scale and DHI Scores at Weeks 0, 2, 6, and 12.

P < .05 considered statistically significant.
Abbreviation: DHI, Dizziness Handicap Inventory.
Mean ± SD.
Wilcoxon signed-rank test.

Within-group changes in dizziness outcomes over 12 weeks of treatment. (A) 11-Point Box Scale scores in the EGb 761® and Betahistine groups. (B) DHI scores in the EGb 761® and Betahistine groups. DHI, Dizziness Handicap Inventory.
Between-group comparison showed no significant differences in 11-Point Box Scale scores. DHI scores were significantly higher in the EGb 761® group at weeks 0, 2, and 6, but not at week 12 (Table 3). However, mean changes in the 11-Point Box Scale and DHI scores showed no significant differences between the EGb 761® and Betahistine groups at weeks 2, 6, and 12 (Table 4).
Between-Group Comparison of 11-Point Box Scale and DHI Scores at Weeks 0, 2, 6, and 12.
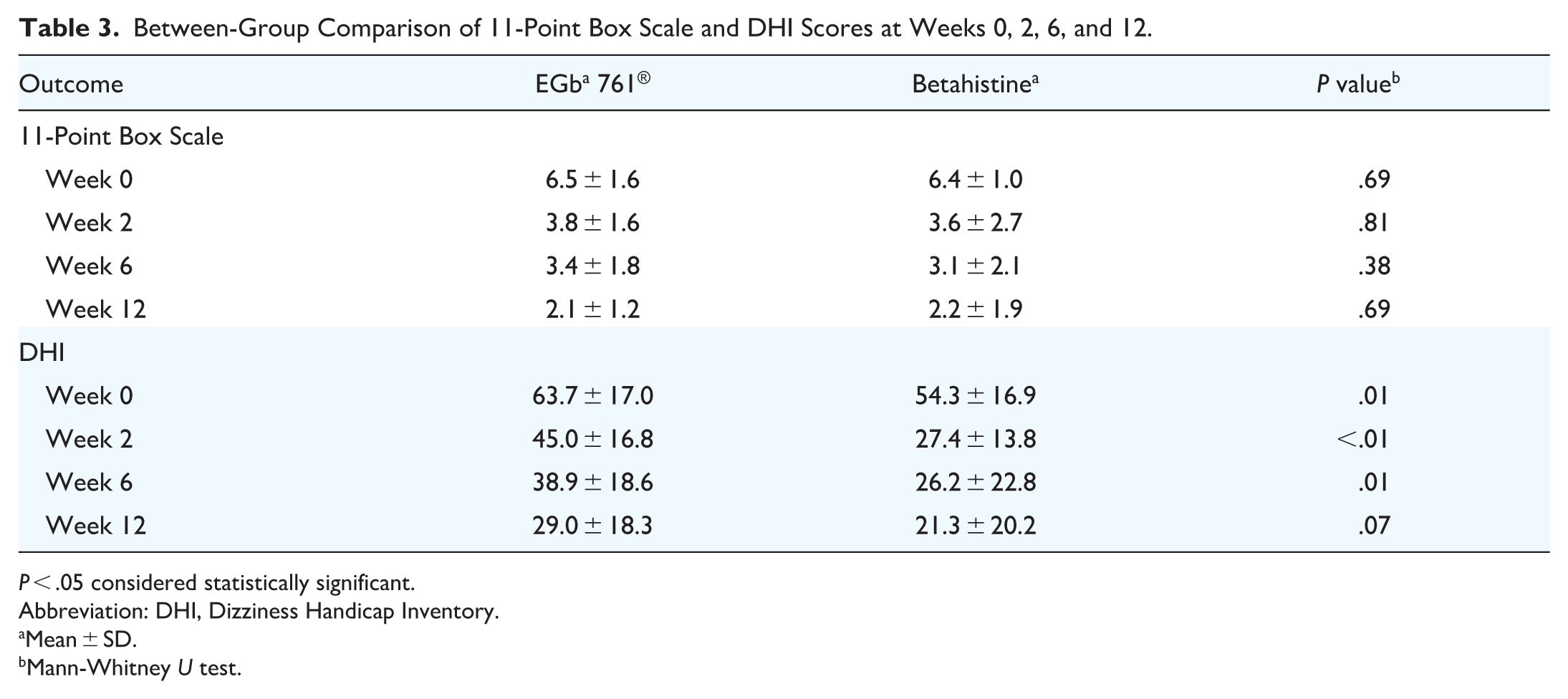
P < .05 considered statistically significant.
Abbreviation: DHI, Dizziness Handicap Inventory.
Mean ± SD.
Mann-Whitney U test.
Mean Differences in 11-Point Box Scale and DHI Scores Between EGb 761® and Betahistine at Weeks 2, 6, and 12.
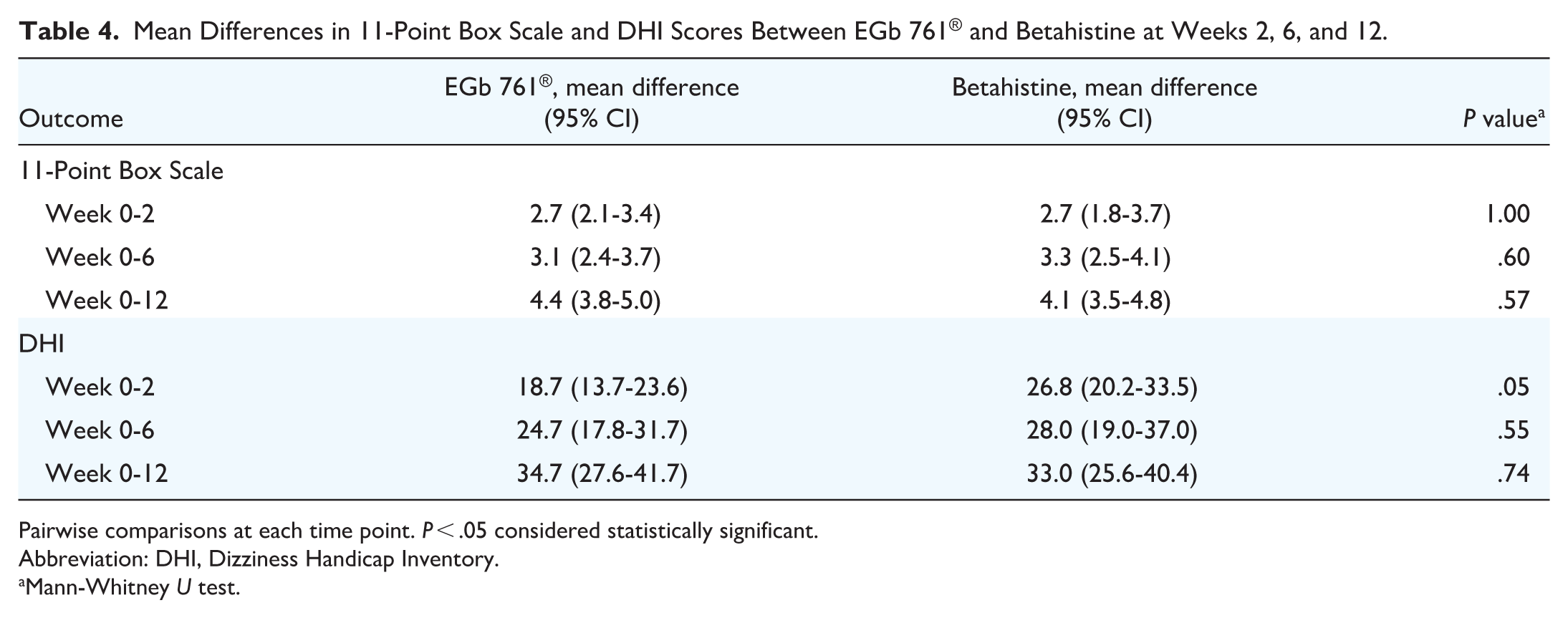
Pairwise comparisons at each time point. P < .05 considered statistically significant.
Abbreviation: DHI, Dizziness Handicap Inventory.
Mann-Whitney U test.
Because baseline DHI scores differed between groups, repeated-measures ANOVA was used across 4 time points (weeks 0, 2, 6, and 12) to adjust for baseline imbalance and assess treatment effects over time.
For 11-Point Box Scale, a significant main effect of time was observed [eta squared (η2) = 0.58, 95% CI 0.51-0.64, P < .01], indicating progressive improvement over 12 weeks in both groups. Neither the group effect nor the group × time interaction was significant (P = .67 and .76), suggesting comparable efficacy between Betahistine and EGb 761®. For DHI, significant main effects were observed for both group (η2 = 0.17, 95% CI 0.05-0.31, P < .01) and time (η2 = 0.51, 95% CI 0.42-0.58, P < .01), while the group × time interaction was not significant (η2 = 0.02, 95% CI 0.00-0.06, P = .13). These findings indicate that DHI scores improved significantly over time in both groups, with an overall greater reduction in the Betahistine group compared with the EGb 761® group (Table 5).
Repeated-Measures ANOVA for 11-Point Box Scale and DHI Scores.

The effect sizes are reported as partial η2. P < .05 considered statistically significant.
Abbreviation: DHI, Dizziness Handicap Inventory; η2, eta squared.
Post hoc pairwise comparisons using Bonferroni correction demonstrated that, at baseline (week 0), the mean DHI did not differ significantly between groups (Cohen’s d = 0.51, 95% CI −0.15 to 1.18; P = .36). A statistically significant difference emerged at week 2, favoring Betahistine (Cohen’s d = 0.96, 95% CI 0.32-1.60; P < .01), while no significant between-group differences were observed at week 6 or 12. These results suggest that Betahistine produced a faster early response, but both treatments achieved comparable improvement by week 12.
Discussion
This randomized controlled trial demonstrated that both EGb 761® and Betahistine effectively improved dizziness and vertigo of unclear etiology, with no significant difference in efficacy over 12 weeks. These results are consistent with previous randomized trials. Sokolova et al 22 demonstrated comparable efficacy between EGb 761® and Betahistine across multiple clinical endpoints in patients with vertigo of various etiologies, with EGb 761® showing slightly better tolerability. Similarly, Cesarani et al 25 and Park et al 26 reported comparable improvement between EGb 761® and Betahistine after 12 weeks, with no significant difference in vertigo control or DHI reduction. Moreover, meta-analyses have supported the modest but clinically meaningful efficacy of both EGb 27 761® and Betahistine27,28 compared with placebo, particularly in reducing the frequency and severity of vertigo episodes.
Unlike most previous trials that assessed outcomes only at 12 weeks, this study included follow-ups at 2, 6, and 12 weeks, providing a clearer trajectory of improvement. Both EGb 761® and Betahistine groups showed significant symptom reduction, most pronounced within the first 2 weeks and continuing gradually thereafter. These findings suggest if patients with dizziness/vertigo of unclear etiology do not show improvement within 2 weeks of treatment with either EGb 761® or Betahistine, the diagnosis or treatment approach should be reconsidered.
Although baseline 11-Point Box Scale scores were higher in the EGb 761® group, they became lower than those of the Betahistine group by week 12, without statistical significance on repeated-measures ANOVA or post hoc analyses. This trend may suggest a potential long-term advantage of EGb 761®, which could become significant with extended treatment.
Previous studies have used EGb 761® for treating dizziness/vertigo dose ranging from 120 22 to 240 mg/day.19,25,29,30 Trials with 240 mg/day generally included older patients (mean age 58-65 years) with comorbid dementia or neuropsychiatric disorders. EGb 761® exerts antioxidant and neuroprotective effects by reducing mitochondrial apoptosis, enhancing mitochondrial function, and improving cognition in mild cognitive impairment.15,16,31,32 Such patients may therefore experience both reduced dizziness and improved neurological function. In this study, the mean patient age was 58.1 years, with no cognitive impairment. The 120 mg/day dose of EGb 761® was still highly effective in reducing dizziness and vertigo, suggesting that this lower dose may be appropriate as first-line therapy for patients under 60 years without dementia or neuropsychiatric comorbidities.
The dosage of Betahistine used in this study (36 mg/day) was found to effectively reduce dizziness and vertigo symptoms. This is consistent with evidence from a Cochrane systematic review, which reported that most clinical trials demonstrating therapeutic benefit employed daily doses between 24 and 48 mg. 28
In this study, both medications were well tolerated with similar side-effect profiles. Mild gastrointestinal disturbances were the most common adverse events, and most patients completed the 12 week treatment without interruption. One patient in the Betahistine group died from coronavirus infection at week 8, but no drug-related adverse effects were reported at earlier follow-ups. Consistent with previous studies, the most common adverse events associated with EGb 761® were gastrointestinal symptoms, followed by headache, sleep disturbances, dizziness, and, rarely, bleeding events.31,32 Nevertheless, Koch 33 demonstrated that PAF-induced platelet aggregation was inhibited only at ginkgolide concentrations exceeding those achieved after oral administration of EGb 761® by more than 100-fold at therapeutic doses (120-240 mg/day). Since PAF is a weak platelet activator and not essential for primary hemostasis, these findings indicate that the PAF-antagonistic activity of ginkgolides is unlikely to pose a clinically relevant bleeding risk. Collectively, these results support the favorable safety and tolerability of both EGb 761® and Betahistine in patients with chronic dizziness.
Limitations
A key limitation of this study is the absence of a placebo control group, making it difficult to distinguish the pharmacologic effects of Betahistine or EGb 761® from the natural course of dizziness, regression to the mean. Previous vertigo trials have demonstrated considerable placebo responses, sometimes approaching the magnitude of active treatments (eg, ~52.5% responders in placebo arms of Meniere’s trials). 34 Thus, while our findings support the efficacy of both agents, the true effect sizes relative to placebo remain uncertain and should be confirmed in future 3-arm randomized controlled trials including a placebo group. Nevertheless, given that the participants in our study had chronic dizziness or vertigo lasting more than 6 months, and that significant clinical improvement was already observed within 2 weeks of treatment initiation, it is reasonable to infer that the improvement observed is predominantly attributable to the pharmacologic interventions rather than a placebo effect.
Another limitation of this study is the relatively small sample size, as it was conducted at a single institution. This may have affected the data distribution and contributed to the baseline difference in DHI scores between the EGb 761® and Betahistine groups. However, additional analyses using repeated-measures ANOVA and post hoc pairwise comparisons demonstrated consistent longitudinal improvement in both groups and confirmed that the observed difference at baseline did not alter the overall treatment effect. These findings support the robustness of our results, indicating that both agents were effective in reducing dizziness-related handicap over time. In addition, as this was a single-center study with a relatively small sample size, the generalizability of our findings to other clinical settings or populations may be limited. Nevertheless, the inclusion criteria and patient characteristics were representative of those commonly encountered in ENT outpatient clinics, suggesting that the results may be applicable to similar clinical contexts.
A further weakness of this study is the reliance on self-reported outcomes, with data limited to subjective measures such as the number of unscheduled ED visits. The inclusion of objective balance tests, such as computerized dynamic posturography, could further clarify the effects of EGb 761® and Betahistine on vestibular function and postural control. Future studies should consider integrating objective measures alongside self-reported scales to strengthen the validity of the results and provide a more holistic evaluation of treatment efficacy.
Conclusion
This study confirms the efficacy and safety of both EGb 761® and Betahistine in managing dizziness/vertigo without specific etiology. Clinical improvement was evident within the first 2 weeks of treatment, suggesting that early assessment of therapeutic response may guide timely management decisions.
Supplemental Material
sj-doc-1-ohn-10.1177_19160216251407927 – Supplemental material for Efficacy of EGb 761® and Betahistine in Treatment of Dizziness/Vertigo: A Randomized Double-Blind Controlled Trial
Supplemental material, sj-doc-1-ohn-10.1177_19160216251407927 for Efficacy of EGb 761® and Betahistine in Treatment of Dizziness/Vertigo: A Randomized Double-Blind Controlled Trial by Narit Jianbunjongkit, Wipan Nattarangsi and Penmas Teeravanittrakul in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Acknowledgements
The authors are grateful for the insightful cooperation of the staff at the Outpatient Department of Otolaryngology, Burapha University Hospital, Chonburi, Thailand. The authors sincerely thank Dr Wallop Jaidee for his valuable statistical consultation.
Author Contributions
Narit Jianbunjongkit: conceptualization, funding acquisition, study design, data collection, data interpretation, writing, editing, revising manuscript. Wipan Nattarangsi: study design, data collection, critical review manuscript. Penmas Teeravanittrakul: supervision, study design, data collection, critical review manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Faculty of Medicine, Burapha University, Grant Number 010/2565.
Ethical Considerations
This prospective randomized double-blind controlled trial was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Burapha University (approval number, HS045/2565) on August 30, 2022.
Consent to Participate
All participants provided written informed consent prior to participating.
Consent for Publication
Not applicable.
Data Availability Statement
The authors consent to share our research data in a relevant public data repository and to cite this data in our research.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.