
Abstract
Importance
Expanding the appropriate use of ambulatory surgical care may improve operating room (OR) efficiency.
Objective
To demonstrate that pediatric adenoidectomy with laryngeal mask airway (LMA) for select patients in the minor procedure room (MPR) is comparable in safety but more efficient than OR adenoidectomy in a pilot study of 20 patients from July to November 2023.
Design
The Institute for Healthcare Improvement Model for Improvement guided this quality improvement project. Safety and efficiency outcomes were prospectively collected for adenoidectomies with LMA in the MPR and compared with retrospective data from similar OR cases with LMA or endotracheal intubation (ETT).
Setting
A single tertiary referral center.
Participants
Pediatric patients who underwent adenoidectomy from July to November 2023.
Interventions
The intervention involved adenoidectomy in the MPR with LMA, as opposed to traditional OR settings.
Main Outcome Measures
The main outcome measures included safety (perioperative respiratory adverse events, conversion from LMA to ETT), efficiency (length of hospital stay, wait time for surgery), and patient/provider satisfaction.
Results
Final analysis included 55 patients [20 (36%) MPR, 35 (64%) OR]. In the OR, 16 (46%) patients used LMA, the rest used ETT. The median [interquartile range (IQR)] age was 5.5 (3.7-7.3) years, and 22 (41%) patients were female. No major respiratory adverse events occurred in the MPR compared to 1 (3%) event in the OR. One (5%) MPR patient required conversion from LMA to ETT due to limited surgical access. Time-based measures were superior in the MPR, with median hospital stay 91 minutes shorter (158.0; IQR: 143.0-204.0 vs 249.0; IQR: 210.0-278.0). Patient and provider satisfaction were highly rated in the MPR.
Conclusions
Pediatric adenoidectomy for select patients in the MPR is a safe and time-efficient alternative to the OR.
Relevance
Further exploration of suitable procedures for the MPR may enhance OR resource allocation.
Level of Evidence. 3

Key Messages
Performing pediatric adenoidectomy for select patients in the minor procedure room (MPR) may offer a safe, time-efficient alternative to the traditional operating room (OR) setting.
In the MPR, there were no major respiratory adverse events, a shorter length of stay in hospital than the OR, and both patients and providers reported high levels of satisfaction with the care provided.
Further exploration of suitable procedures for the MPR and other ambulatory surgical care settings may improve resource allocation in the OR.
Introduction
The operating room (OR) is universally recognized as one of the most expensive and resource-intensive areas in the hospital. 1 The mismatch between supply and demand for OR time results in lengthy wait times, contributing to financial losses and inferior patient outcomes. In 2018, the Fraser Institute reported a $2.1 billion loss in wages in Canada due to surgical wait times. 2 Concerningly, recent data by the Canadian Broadcasting Corporation in January 2023 showed that nearly 12 000 children were on surgical wait lists in Ontario with 50% waiting beyond clinically recommended wait times. 3
The minor procedure room (MPR) is a publicly funded hospital-based outpatient procedure department established in 2015 at the Children’s Hospital at London Health Sciences Centre (CH-LHSC) to accommodate minor pediatric procedures requiring general anesthesia outside of the main OR setting. The prevalence of ambulatory surgical care has been rising in Canada due to its established safety, efficiency, and potential to alleviate lengthy surgical wait times.4,5 Similar to the OR, the MPR team consists of a pediatric surgeon, pediatric anesthesiologist, anesthesia assistants when appropriate, and nursing personnel. However, the MPR nurses are from the Pediatric Medical Day Unit, unlike the specialized OR nurses. The objective of the MPR was to ease the OR burden and increase accessibility for pediatric patients awaiting surgery. A study by Davidson et al showed that bilateral myringotomy with tube insertions was more time and cost-efficient when performed in the MPR versus the OR. 6 Notably, the median length of time in room was 11 minutes shorter, length of hospital stay was 2.3 hours shorter, and patient turnover time was 8 minutes shorter. Compared to the OR, patients in the MPR check-in closer to their surgery start time, recover in a less resource-intensive area than the post-anesthesia care unit (PACU), and are discharged sooner due to nursing and patient discharge streaming capabilities. 6
Pediatric adenoidectomy is a common surgical procedure that may benefit from a transition to the MPR environment. 7 This operation involves the removal of the adenoids, which are proliferations of lymphoid tissue along the posterior wall of the nasopharynx. 8 There are numerous indications for an adenoidectomy in children, with the most common including chronic adenoiditis, otitis media with effusion (OME), and obstructive sleep apnea. 9 Although pediatric adenoidectomies are traditionally performed with endotracheal intubation (ETT), laryngeal mask airway (LMA) has become an accepted alternative that may improve OR efficiency. 10 In recent years, there has been increased usage of LMA versus ETT in children due to the relative ease of insertion and removal, minimal disturbances in the cardiorespiratory system, and diminished risk of perioperative airway injury.11 –13
Although the use of LMA in oropharyngeal surgery may be limited by surgical access or kinking causing ventilation issues that require conversion to ETT, a meta-analysis by Khoury et al demonstrated that LMA is a safe alternative to ETT. Furthermore, LMA was associated with decreased operative time for adenotonsillectomy.14,15 The established success of LMA and the MPR supports a trial of adenoidectomy with LMA in the MPR.
The widening discrepancy between demand for surgical procedures and OR availability points to the need for hospital-wide quality improvement initiatives. 6 By establishing the safety and efficiency of pediatric adenoidectomy in the MPR, it may be possible to provide patients with a decreased length of stay, increase OR availability for more intensive procedures, and decrease hospital-related costs.
Materials and Methods
Problem Characterization
At CH-LHSC, the standardized onboarding process for new surgical procedures in the MPR includes a trial period to ensure that the MPR and its staff can accommodate new procedures. In July 2023, a trial approval was granted to perform twenty pediatric adenoidectomies in the MPR. The approval process occurred independently of this quality improvement project, which aims to demonstrate that pediatric adenoidectomy with LMA for select patients in the MPR is comparable in safety but more efficient than OR adenoidectomy in a pilot study of 20 patients from July to November 2023. A driver diagram (Figure 1) was constructed to highlight the relationships between the aim of the project and the various drivers and change ideas needed to achieve our objective. Based on the driver diagram, several change ideas were implemented, including various educational initiatives (June 2023), a staff training simulation (July 2023), and a trial of adenoidectomies with LMA in the MPR (July-November 2023).

Driver diagram. LMA, laryngeal mask airway; MPR, minor procedure room.
Stakeholder Involvement
A multidisciplinary team of stakeholders was identified early, from leadership to in-house staff. This included pediatric otolaryngologists, pediatric anesthesiologists, anesthesia assistants, a Pediatric Medical Day Unit nurse educator and nurses, an OR charge nurse, and clinical managers.
Project Design and Implementation Strategy
The Institute for Healthcare Improvement’s Model for Improvement was used to frame the quality improvement strategy (Table 1). 16 An observational case–control design was used, with cases being adenoidectomies performed in the MPR collected prospectively, and controls being adenoidectomies performed in the OR collected retrospectively. Data collected included demographic information, safety measures, time-based measures, and patient and provider satisfaction. In order to compare sustained hypoxic events, data were extracted from the anesthesia documentation for both patients in the OR and MPR. These data account for the average oxygen saturation in a 15-minute interval. In the OR, the decision to use LMA versus ETT was at the discretion of the attending surgeon and anesthesiologist.
Institute for Healthcare Improvement’s Model for Improvement.

Abbreviations: ETT, endotracheal intubation; LMA, laryngeal mask airway; MPR, minor procedure room; OR, operating room.
Setting and Participants
The project was conducted within the Otolaryngology—Head and Neck Surgery (OHNS) Department at CH-LHSC, London, ON, Canada. The initiative was given a research ethics board exemption as a quality improvement project. The reporting of this investigation is consistent with SQUIRE 2.0 guidelines. 17 Patients and families were informed about the similarities and differences between the MPR and OR environments before surgical consent was obtained. Patients were included if they were under 18 years old at the time of adenoidectomy. The team included 4 pediatric otolaryngologists, 10 pediatric anesthesiologists, and a team of residents and nurses.
Minor Procedure Room
Clinical information was prospectively collected on 20 patients who underwent adenoidectomy with LMA in the MPR, from July to November 2023. Patients deemed appropriate for the MPR setting were generally healthy with an American Society of Anesthesiologists’ (ASA) classification of 1 or 2, non-syndromic, non-obese, 3 years of age or older, without a history of difficult airway, and did not have sleep-disordered breathing. The primary indications for adenoidectomy in this cohort were adenoid hypertrophy associated with OME, OME requiring additional sets of tympanostomy tubes, and chronic adenoiditis. A custom data collection sheet developed a priori was concurrently completed by staff, and a patient satisfaction questionnaire was filled out by parents prior to departure.
Operating Room
Patients were identified through patient scheduling on 4 pediatric otolaryngologists’ electronic medical records (EMR). Clinical information was retrospectively collected on 35 eligible patients who underwent adenoidectomy ± ear tubes with LMA or ETT in the OR, from July to October 2023. Patients in the OR cohort had an ASA classification between 1 and 3, were non-obese, and 2 years of age or older. Patient charts were reviewed through their EMR at LHSC. The patients chosen were treated by the same group of pediatric otolaryngologists and anesthesiologists. They were not matched for demographic characteristics.
Procedure and Patient Flow
In both the MPR and OR, adenoidectomies were scheduled for 1 hour. In the MPR, patients checked in 1 hour prior to surgery versus 2 hours prior to surgery in the OR. Post-operatively, patients in the MPR were transferred to a less resource-intensive recovery area in Day Surgery, whereas patients in the OR were transferred to the PACU.
Measures
Primary Outcome Measures
The incidence of perioperative respiratory adverse events (PRAEs), operationally defined as: apnea, bronchospasm, laryngospasm, and sustained hypoxia (<85% average oxygen saturation over 15 minutes).
Secondary Outcome Measures
The conversion rate from LMA to ETT (%), transient hypoxia (<85% oxygen saturation for >10 seconds), post-operative complications including desaturation (<95%), nausea/vomiting, and pain (persistent despite pre-operative acetaminophen and ibuprofen, and routine intraoperative analgesia), wait time for surgery, and patient satisfaction post-surgery. Other intraoperative complications were included, such as gagging, stridor, and kinking issues or obstruction from mouth gag insertion with the use of LMA.
Process Measures
Time from registration to MPR/OR, time to intubate, total length of surgery, adenoidectomy duration, duration with LMA, time to extubate, duration in MPR/OR, time from end of surgery to recovery bay, length of time out of MPR/OR to discharge, and total length of hospital stay.
Balancing Measures
Care provider comfort level was assessed to determine whether our proposed changes introduced problems elsewhere in the system.
Data Analysis
Descriptive statistics were used to characterize the patients undergoing surgery in both the OR and the MPR. Differences between groups were reported as absolute values and percentages without formal statistical analysis, in alignment with the Quality Improvement design of this study. Patients in the MPR group were selected based on predefined criteria, resulting in a cohort that was older, non-syndromic, and generally healthier. These inherent differences precluded the feasibility of formal statistical comparisons between groups. All data analyses were completed using SAS Software (Version 9.4; SAS Institute, Inc, Cary, NC, USA).
Results
Demographics
The final analysis included 55 patients, with 20 (36%) in the MPR group and 35 (64%) in the OR group (16 LMA, 19 ETT). Overall, the median age was 5.5 years [interquartile range (IQR): 3.7-7.3], and 22 (41%) patients were female (Table 2). The median ASA classification was 2.0 (IQR: 2.0-3.0). The MPR group was older (median: 6.1 years; IQR: 5.2-8.4 vs 5.0 years; IQR: 3.1-6.5), and weighed more at the time of surgery (median: 25.0 kg; IQR: 19.1-31.7 vs 20.5 kg; IQR: 15.6-25.1) than the OR group.
Patient Demographics.
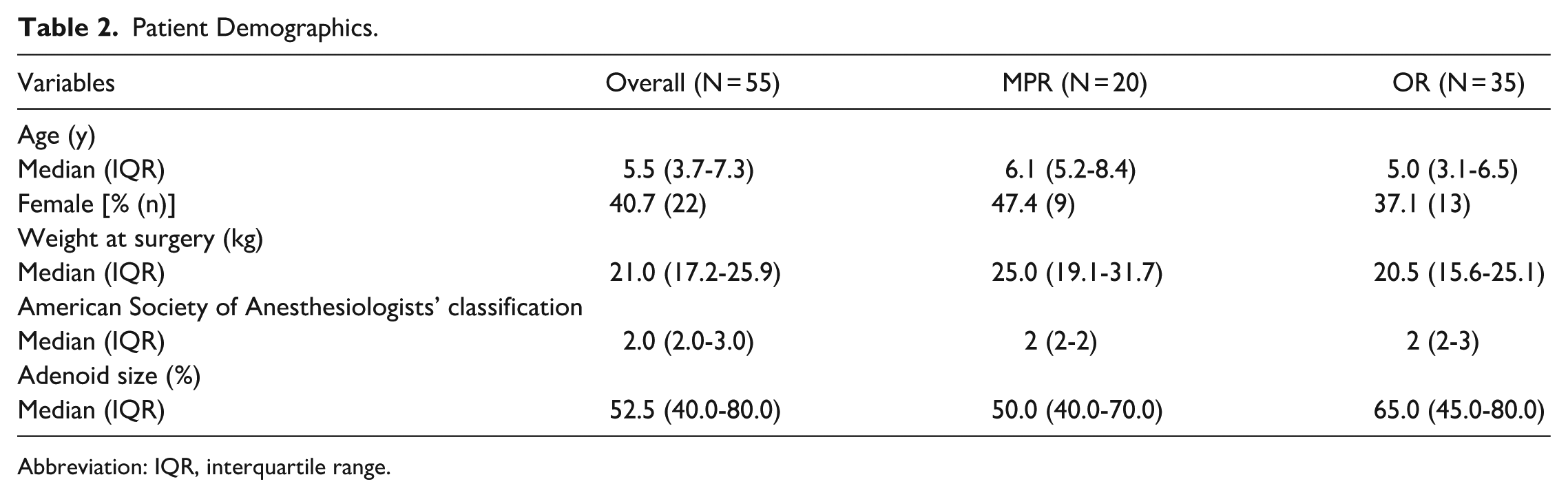
Abbreviation: IQR, interquartile range.
Safety Measures
In the MPR, there were no PRAEs, 3 (15%) transient hypoxic events, and 1 (5%) conversion from LMA to ETT for poor surgical access (Table 3). There were 2 (10%) post-operative desaturations, 3 (16%) patients with post-operative nausea/vomiting, and 5 (26%) patients with post-operative pain. By contrast, 1 (3%) patient in the OR using LMA experienced a sustained hypoxic event. Data pertaining to transient hypoxic events and post-operative complications were unavailable for the OR group. Intraoperative bleeding was minimal in both groups.
Safety and Efficiency Measures for Pediatric Adenoidectomy in the MPR Using LMA Compared to the OR Using LMA or ETT.

Abbreviations: ETT, endotracheal intubation; IQR, interquartile range; LMA, laryngeal mask airway; MPR, minor procedure room; OR, operating room; PACU, post-anesthesia care unit.
Time-Based Measures
There was a decrease in surgical wait times for the MPR compared to the OR (116.0 days; IQR: 93.0-133.0 vs 136.0 days; IQR: 108.0-163.0). Notably, there was a difference in hospital length of stay, with median time in the hospital being 91 minutes shorter in the MPR (158.0 minutes; IQR: 143.0-204.0) compared to the OR (249.0 minutes; IQR: 210.0-278.0). The MPR group had a shorter length of time from registration to room (60.5 minutes; IQR: 34.0-73.0 vs 113.0 minutes; IQR: 91.0-128.0), shorter length of time in room (37.5 minutes; IQR: 30.0-44.0 vs 45.0 minutes; IQR: 38.0-55.0), and shorter length of time from end of surgery to the recovery bay (5.0 minutes; IQR: 4.0-6.0 vs 12.0 minutes; IQR: 9.0-19.0). Patients in the OR who underwent LMA had a shorter length of time from end of surgery to the PACU than those who underwent ETT (9.0 minutes; IQR: 6.5-12.5 vs 14.0 minutes; IQR: 12.0-19.0; Table 4). All cases in the MPR included a concomitant minor procedure, whereas 89% of cases in the OR included a concomitant minor procedure. In the MPR, concomitant minor procedures included tympanostomy tube insertion, inferior turbinate reduction, or cauterization of nasal septum. In addition to the aforementioned procedures, concomitant minor procedures in the OR included tooth extraction, foreign body removal, and tongue tie release.
Safety and Efficiency Measures for Pediatric Adenoidectomy in the OR Using LMA Compared to ETT.

Abbreviations: ETT, endotracheal intubation; IQR, interquartile range; LMA, laryngeal mask airway; OR, operating room; PACU, post-anesthesia care unit.
Patient and Provider Satisfaction
Based on the patient satisfaction questionnaire for the MPR (Table A1), all patients/families felt involved in treatment decisions, all patients/families were satisfied with their care, and the median rating of the overall experience at CH-LHSC was 10/10 (IQR: 10-10).
Overall, care providers felt confident with LMA in the MPR, with a median surgical exposure rating of 5/5 (IQR: 4.0-5.0) and median anesthesiologist rating of 4.5/5 (IQR: 3.5-5.0). To calculate these values, clinicians were asked to provide ratings based on their satisfaction with different aspects of the procedure. Surgeons described their satisfaction with visualization of the surgical field, and anesthesiologists evaluated their satisfaction with airway management. During each post-operative briefing session, all surgeons, anesthesiologists, and pre- and post-operative nurses reported feeling comfortable providing care to the patient. All care providers commented that adenoidectomy should be offered in the MPR with the exception of 2 anesthesiologists, one who reported “no comment,” and the other who reported they were “not keen on it.”
Discussion
Using a quality improvement approach, we have demonstrated that adenoidectomy with LMA in the MPR for select pediatric patients is comparable in safety but more efficient than the same procedure in the OR in a pilot study of 20 patients from July to November 2023. Selection criteria ensured a suitable patient cohort, facilitating the successful introduction of this procedure into the MPR.
The safety of pediatric adenoidectomy with LMA in the MPR is supported by the similar incidence of major adverse events, defined as PRAEs, when compared to the OR group. There was a similar rate of sustained hypoxic events, and 2 of the 3 transient hypoxic events in the MPR occurred prior to LMA placement. There was 1 MPR case that required conversion to ETT due to inadequate surgical exposure. As the mouth gag was opened to improve access, difficulties in ventilation occurred, prompting conversion. Notably, this was only the second adenoidectomy in the trial of twenty. After this case, the OHNS team inquired among colleagues in an international pediatric otolaryngology chat group and learned that it would be superior to avoid taping the LMA in place. Following this procedural change, no additional cases required conversion to ETT. To further enhance safety, and at the request of the pediatric anesthesiologists, MPR nurses, a nurse educator, and an anesthesia assistant were added to the team to ensure additional airway support was available if needed.
The observed decrease in surgical wait times for the MPR group may indicate increased surgical accessibility in this setting. It is crucial to frame this comparison within the context of OR time allocation at our center. In early 2023, our Pediatric Otolaryngology division had the lengthiest surgical waitlist of all pediatric specialties, prompting incremental OR catch-up time over the course of this project. Thus, an analysis of wait times at a different point in time may have more strongly favored the MPR. The local trends at CH-LHSC align with national trends, as the Canadian Pediatric Surgical Wait Times Project found that the surgical wait list for pediatric otolaryngology was longer than all other subspecialties. 18
Patients undergoing adenoidectomy in the MPR experienced a shorter length of stay in hospital and improved time-based process measures. The decreased length of stay may reflect changes applied to routine post-operative monitoring. Instead of the standard 3-hour post-operative monitoring period followed in the OR, patients in the MPR were discharged upon meeting established discharge criteria. Additional improvements in time efficiency may be attributed to streamlined patient flow processes in the MPR. Importantly, several of these administrative changes, including criteria-based discharge, could be implemented in the OR setting, and additional optimization of perioperative protocols may further enhance efficiency and resource utilization. Furthermore, the shorter time from surgery to PACU observed in OR patients with LMA compared to ETT likely reflects literature-supported efficiency advantages, including easier insertion and removal, ability to remove the device in the PACU, reduced anesthetic and neuromuscular blocker requirements, decreased physiologic stress, and overall improved quality of recovery.19 –21 Following the conclusion of prospective data collection for this project, efficiency in the MPR continued to improve as pediatric adenoidectomies in the MPR were scheduled for 45-minute intervals instead of the 1-hour interval required previously, which continues to exist in the OR.
Patient satisfaction was rated highly across a diverse range of variables. Directly assessing patient satisfaction is essential, as the subjective patient experience is a complex model that revolves around surgical expectations and individual personality traits.22 –26 A patient satisfaction survey was utilized with the input of multidisciplinary stakeholders to minimize bias as previous studies evaluating satisfaction in pediatric patients using large value-based medicine questionnaires raised concerns regarding their veracity. 22 The high degree of provider comfort level indicates minimal issues arose elsewhere in the system.
The project’s success was facilitated by instituting an iterative approach to change, as described by Kotter. 27 A sense of urgency was created in response to the systemic crisis of lengthy pediatric surgery wait times. The early establishment of a multidisciplinary leadership team was crucial, with champions in pediatric OHNS, pediatric anesthesia, nursing, and clinical management leading this project. In particular, the study highlighting the increased time and cost efficiency of bilateral myringotomy in the MPR, along with preliminary results from the meta-analysis demonstrating the safety and time efficiency of LMA, were pivotal in securing stakeholder engagement.6,15 Development of the quality improvement methodology led to a strong guiding vision with a detailed characterization of the problem. Leaders engaged in regular meetings and post-operative debriefing sessions to maintain a steady flow of communication, celebrate short-term successes, and review potential obstacles. For instance, after the LMA to ETT conversion, discussion among the pediatric otolaryngologists led to improvement of the LMA process. The final stage of quality improvement, cultural integration, is the most challenging and remains an ongoing process involving continuous performance review, feedback, and communication.
The use of prospectively collected MPR data alongside retrospectively collected OR data introduced several limitations. Firstly, our analysis was limited to sustained hypoxic events because OR charts represented oxygen saturation values in 15-minute intervals and did not include transient hypoxic events. Secondly, data pertaining to post-operative complications, patient satisfaction, and provider comfort level were unavailable in the OR. Thirdly, adenoidectomy procedure time was not isolated in the OR, so the total surgery length was used for comparison, which may be confounded by concomitant procedures. However, this limitation was mitigated by similar rates of concomitant procedures across both settings. Another constraint was the demographic differences between the MPR and OR group. Patients in the MPR group were intentionally selected to be older (age 3 and older), and thus weighed more, had no history of sleep disordered breathing, and were also selected to have a lower ASA status (ASA 1 or 2 only), as more complex patients were scheduled to the OR for airway safety. Since sleep disordered breathing patients represent a substantial portion of adenoidectomies, their exclusion from the MPR may limit the generalizability of our findings. Future studies may explore the inclusion of these patients in the MPR with appropriate safeguards and training personnel. A final limitation was the individual-focused change ideas in the hierarchy of effectiveness for quality improvement interventions. 28 Individual-focused interventions such as education and training are generally less effective than systems-focused interventions such as forcing functions and automation. However, our project implemented active educational interventions such as a staff training simulation in addition to passive strategies, which are known to achieve better results.
Overall, there were several key lessons derived from this PDSA cycle that will be adapted for the next PDSA cycle. Firstly, it is essential to avoid taping the LMA in place and maintain ongoing support by nursing personnel and an anesthesia assistant for airway management. Although the addition of an anesthesia assistant introduces an additional expense, the total cost of this procedure remains lower in the MPR than in the main OR. This is supported by previous findings, which demonstrated cost savings of $279.15 for each case of bilateral myringotomy with tube insertions performed in the MPR setting compared to the main OR. 6 Future studies incorporating a formal cost analysis with a larger patient cohort would provide valuable insights. The inclusion criteria for the MPR will be upheld to ensure patients with increased complexity are appropriately directed to the OR setting. These criteria include ASA classification of 1 or 2, non-syndromic, non-obese, 3 years of age or older, no history of difficult airway, and absence of sleep-disordered breathing. Additionally, time allotted to adenoidectomy cases will be 45 instead of 60 minutes. Finally, implementing dynamic educational initiatives and consistent communication with stakeholders are crucial for fostering balanced quality improvement efforts.
After the successful trial of 20 adenoidectomies in the MPR, this approach has been incorporated into the available standard of care for appropriate patients at CH-LHSC. Over a 1-year period, 51 adenoidectomies have been completed in the MPR, which is the equivalent of 51 hours diverted from the main OR, or more than 7 OR days saved. Alongside improvements in OR efficiency, this approach offers co-benefits, such as a decreased carbon footprint and a positive impact on planetary health by reducing resource consumption and waste generation typically associated with main OR procedures. By integrating environmental sustainability into procedural choices, this initiative aligns with broader goals of responsible resource stewardship in healthcare.
Conclusion
In conclusion, this quality improvement project demonstrated that performing pediatric adenoidectomy in the MPR for select patients is a safe, time-efficient alternative to the traditional OR, with positive feedback from both patients and care providers. Exploring research into the suitability of additional procedures for the MPR has the potential to further alleviate the surgical burden on the OR, contributing to more efficient use of healthcare resources.
Footnotes
Appendix
Patient Satisfaction Questionnaire Responses for Pediatric Surgery in MPR.

| Category | Sub-Category | Very satisfied | Satisfied | Neutral | Unsatisfied | Very unsatisfied | N/A |
|---|---|---|---|---|---|---|---|
| Arriving for Surgery [% (n)] | Parking (if applicable) | 62.5 (10) | 18.8 (3) | 12.5 (2) | 0 | 0 | 6.25 (1) |
| Getting around the hospital (eg, signage, accessibility) | 68.8 (11) | 25 (4) | 6.25 (1) | 0 | 0 | 0 | |
| Registration process (eg, explanations, ease of process) | 62.5 (10) | 25 (4) | 12.5 (2) | 0 | 0 | 0 | |
| Wait times/updates on delays (eg, tracking board) | 56.3 (9) | 43.8 (7) | 0 | 0 | 0 | 0 | |
| Level of Preparedness [% (n)] | Before surgery based on the information provided by doctor’s office | 68.8 (11) | 25 (4) | 6.25 (1) | 0 | 0 | 0 |
| Before surgery based on the information provided by pre-admit clinic (phone or visit) | 62.5 (10) | 31.3 (5) | 6.25 (1) | 0 | 0 | 0 | |
| Comfort with caring for yourself/your child after surgery based on information provided by doctor(s) | 81.3 (13) | 18.8 (3) | 0 | 0 | 0 | 0 | |
| Comfort with caring for yourself/your child after surgery based on information provided by nurses (eg, discharge instructions) | 75 (12) | 25 (4) | 0 | 0 | 0 | 0 | |
| Staff (eg, communication, care, empathy) [% (n)] | Reception | 62.5 (10) | 37.5 (6) | 0 | 0 | 0 | 0 |
| Nurses before surgery | 93.8 (15) | 6.25 (1) | 0 | 0 | 0 | 0 | |
| Nurses after surgery | 93.8 (15) | 6.25 (1) | 0 | 0 | 0 | 0 | |
| Surgeons | 93.8 (15) | 6.25 (1) | 0 | 0 | 0 | 0 | |
| Anesthesiologists | 93.8 (15) | 6.25 (1) | 0 | 0 | 0 | 0 | |
| Child life specialists (eg, PPI Program) | 93.8 (15) | 6.25 (1) | 0 | 0 | 0 | 0 | |
| Volunteers | 68.8 (11) | 6.25 (1) | 25 (4) | 0 | 0 | 0 | |
| Environment (eg, comfort, cleanliness) [% (n)] | Waiting area (eg, registration, day surgery) | 50 (8) | 43.8 (7) | 6.25 (1) | 0 | 0 | 0 |
| Playroom | 37.5 (6) | 0 | 0 | 0 | 0 | 62.5 (10) | |
| MPR | 75 (12) | 18.8 (3) | 0 | 0 | 0 | 6.25 (1) | |
| Recovery bay | 81.3 (13) | 18.8 (3) | 0 | 0 | 0 | 0 | |
| Privacy and confidentiality | 68.8 (11) | 25 (4) | 6.25 (1) | 0 | 0 | 0 | |
| Overall satisfaction | |||||||
| Patients/families that always felt involved as much as they wanted to be in decisions about their/their child’s care and treatment [% (n)] | 100 (16) | ||||||
| Patients satisfied with the care they/their child received [% (n)] | 100 (16) | ||||||
| Rating (1-10) of their/their child’s overall experience at CH-LHSC [median (IQR)] | 10 (IQR: 10-10) | ||||||
Abbreviations: CH-LHSC, Children’s Hospital at London Health Sciences Centre; MPR, minor procedure room; PPI, parental presence at induction of anesthesia.
Acknowledgements
Special thanks to Dr Karan Gandhi for the development of the patient satisfaction questionnaire and Molly Fitzgerald for the creation of the updated adenoidectomy patient information pamphlet. We would like to acknowledge all physicians, nursing staff, and clinical managers from London Health Sciences Centre in London, ON, Canada.
Author Contributions
Ram Patel: design, conduct, analysis, presentation. Sami Khoury: design, conduct, analysis, presentation. Jacob Davidson: design, conduct, analysis, presentation. Peng You: design, conduct, analysis, presentation. M. Elise Graham: design, conduct, analysis, presentation. Murad Husein: design, conduct, analysis, presentation. Raju Poolacherla: design, conduct, analysis, presentation. Gopakumar Nair: design, conduct, analysis, presentation. Abhijit Biswas: design, conduct, analysis, presentation. Catherine Delaney: design, conduct, analysis, presentation. Julie E. Strychowsky: design, conduct, analysis, presentation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Given the quality improvement design, an institutional review board exemption was obtained from the Health Sciences Research Ethics Board (HEREB) at Western University, London, ON, Canada.
Data Availability Statement
Data may be available upon request to the corresponding author.