
Abstract
Importance:
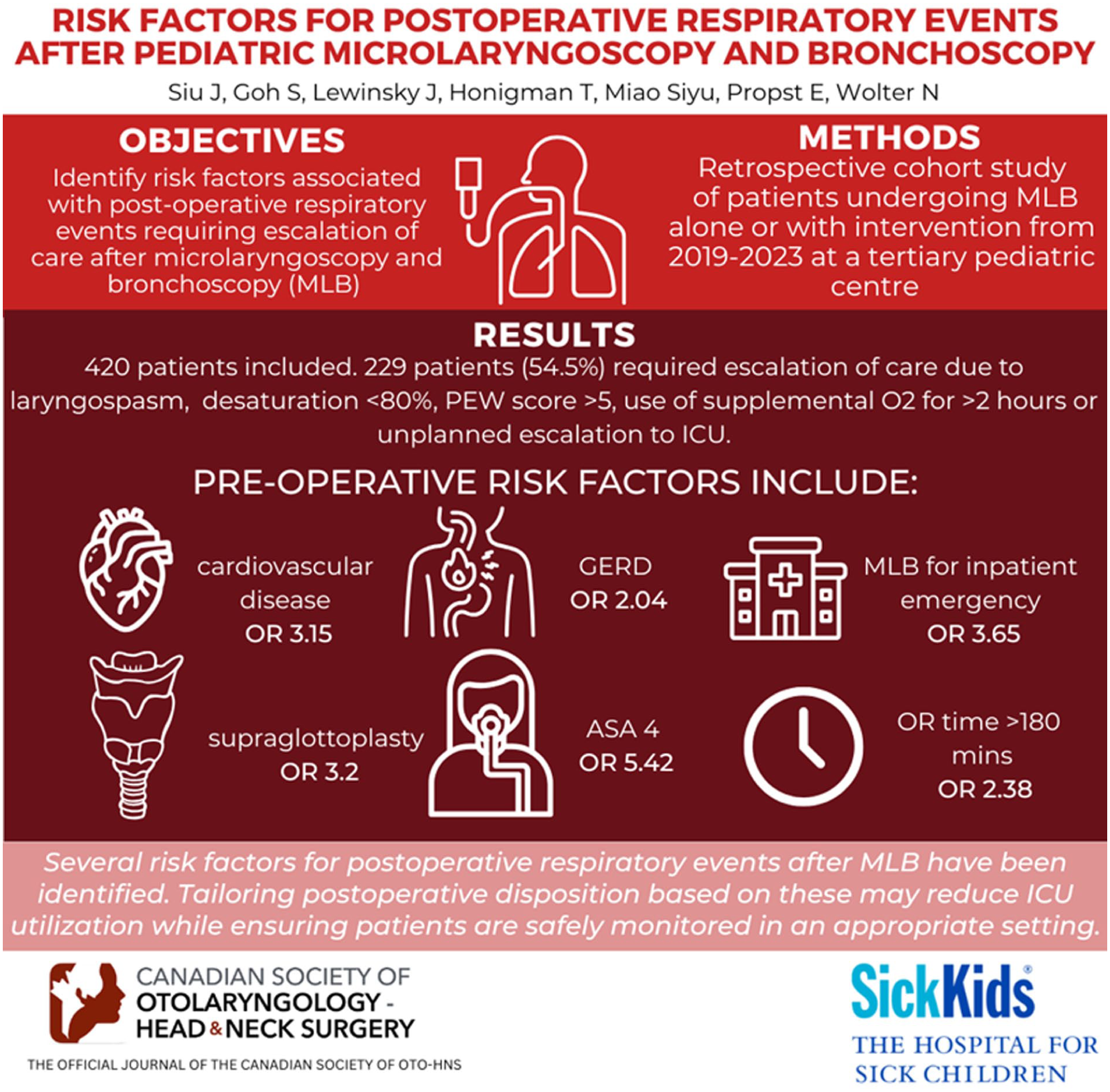
Preoperative risk factors can guide appropriate postoperative disposition location to a ward bed, intermediate care, or intensive care unit after pediatric microlaryngoscopy and bronchoscopy (MLB), resulting in optimization of resource use and costs.
Objective:
Identify risk factors associated with postoperative respiratory events requiring escalation of care after MLB to identify a subpopulation of high-risk patients.
Design:
Retrospective cohort study.
Setting:
Tertiary pediatric center.
Participants:
Patients undergoing MLB alone or with intervention from 2017 to 2023.
Intervention:
MLB alone or with intervention.
Main Outcome Measures:
Primary outcome was postoperative respiratory events requiring escalation of nursing care: escalation of oxygen supplementation for >2 hours, laryngospasm, bronchospasm, unplanned escalation of care to ICU, O2 desaturation <80% and Pediatric Early Warning Score (PEW score) >5. Multivariate logistic regression was performed to identify risk factors for postoperative respiratory events.
Results:
420 patients were included. The mean age was 39.4 months and 41% were female. Overall, 229 patients (54.5%) had events that required escalation of care. Five patients (1.2%) had laryngospasm, 5 (1.2%) desaturated below 80%, and 15 (3.6%) required an unplanned escalation of care to the ICU. 157 (37.4%) required escalation of care based on a PEW score >5, and 148 (35.2%) required supplemental O2 for >2 hours. Multivariate analysis identified independent risk factors for postoperative respiratory events including age 1 to 2 years (OR 2.47, P = .037), cardiovascular disease (OR 2.96, P = .0066), GERD (OR 1.89, P = .042), ASA IV (OR 5.76, P = .0032), MLB with supraglottoplasty (OR 4.34, P = .0081), inpatient surgery (OR 4.68, P < .0001), and operative time ≥180 minutes (OR 2.16, P = .05).
Conclusion:
Risk factors for postoperative respiratory events after MLB include age 1 to 2 years, CVD, GERD, ASA 4, MLB with supraglottoplasty, inpatient emergency, OR time >180 minutes. Tailoring postoperative disposition based on these preoperative risk factors may result in a reduction in ICU utilization while ensuring patients are safely monitored in an appropriate setting.
Level of Evidence:
Level 3
Key message
Risk factors for postoperative respiratory events after MLB include CVD, GERD, ASA 4, ML with supraglottoplasty, and OR time >180.
Introduction
Microlaryngoscopy and rigid bronchoscopy (MLB), with and without intervention, is one of the most common procedures performed in a pediatric otolaryngology program.1,2 Even though MLB is invaluable for diagnosing and treating various airway conditions, it carries inherent risks and potential complications. Respiratory events account for 75% of all critical perioperative events in children undergoing anesthesia for any procedure and can range from mild respiratory distress to severe respiratory failure.3–6 Rigid bronchoscopy in particular carries the risks of bronchospasm and oxygen desaturation, which occur in 8% to 17% of endoscopies.7,8 These events can lead to increased hospital length of stay, hospital costs, and worse patient outcomes.3–6
Disposition location following MLB is essential for providing the appropriate level of monitoring, given the possibility of adverse respiratory events. Disposition options range considerably in terms of level of monitoring and resource utilization, from low-intensity standard ward (1:4 nursing, $2,672 CAD/night), stepdown (1:2 nursing, $4,593 CAD/night), and intensive care unit (ICU) (1:1 nursing, $8,446 CAD/night) (6, 9). Postoperative disposition after MLB varies across institutions and surgeons, and there is a sparsity of data supporting any decisions. This may result in more resource-intensive, higher-acuity settings than necessary. This is suboptimal in the current healthcare environment, where optimizing resource allocation is crucial to providing value-based care.
The primary aim of this study was to identify predictors of postoperative respiratory events following MLB, to determine which patients are at high risk and would benefit from more highly monitored settings than a standard ward bed.
Methods
This study was approved by the Hospital for Sick Children Institutional Review Board (2023-04-28T13-56-13). Data were collected from all rigid MLBs in patients under 18 years of age at our pediatric tertiary care institution from 2017 to 2023. Patients were included if they underwent MLB alone or with an intervention. Chronically ventilated patients were not included in the analysis. All MLBs were performed or supervised by an experienced pediatric otolaryngologist in the operating room under general anesthesia administered by an experienced pediatric anesthesiologist, with the child spontaneously breathing. Supplemental oxygen was used to avoid desaturations. Lidocaine 2% (maximum 2 mg/kg) was applied to the vocal cords at the beginning of each case to prevent laryngospasm. Procedures were performed with a 2.9 mm or 4.0 mm 0-degree rigid telescope (Karl Storz, Germany) and a ventilating rigid bronchoscope, where needed. Disposition for all patients in this study was either to a stepdown unit with 1:2 nursing care or the ICU with 1:1 nursing care. Differences in postoperative monitoring and care capabilities vary widely across hospitals. Therefore, we have clearly defined inpatient care settings based on the level of care intensity at our institution. ICUs in our hospital are capable of delivering high-acuity interventions, such as invasive mechanical ventilation, new initiation of continuous positive airway pressure (CPAP), and high-flow nasal cannula (HFNC) at high-flow settings. Stepdown units at our institution function as intermediate care areas, typically providing non-invasive respiratory support for patients who are clinically stable but still require close monitoring. This includes modalities such as low-to-moderate HFNC, ongoing CPAP, and continuous pulse oximetry. While not all hospitals have designated stepdown units, at our institution, they serve as a bridge between ICU and standard ward care. Finally, our standard inpatient wards are considered low-intensity care settings, though, upon special circumstances, they can be equipped with continuous pulse oximetry monitoring. These operational definitions were used consistently throughout this study.
Clinical data were obtained from patient charts, discharge letters, bronchoscopy documentation, and anesthesiology records. Data collection included demographic data, associated medical comorbidities, ASA status, indication for bronchoscopy, operative details, intervention(s), duration of anesthesia, and postoperative respiratory events. The following baseline demographic data were utilized in this study: age at time of bronchoscopy, weight, and medical comorbidities (Table 1). Procedure setting was categorized as elective outpatient, emergency foreign body removal, or urgent inpatient procedure. Procedure type was categorized into pragmatic clinical groupings that could be anticipated preoperatively to guide postoperative disposition planning. Cases were classified as MLB alone, MLB with foreign body removal, MLB with additional intervention (eg, balloon dilation, cyst/mass removal, and laryngeal cleft repair), MLB with supraglottoplasty, and MLB with adenotonsillectomy. These groupings were chosen to balance the limitations of sample size with clinical relevance, rather than based on a formal sample size calculation. We acknowledge that there is variability in procedural complexity within each category, which may influence postoperative recovery and outcomes. ASA was categorized on a scale of 1 to 4 as documented by the anesthesiologist.
Baseline Characteristics of Patients Undergoing Rigid Bronchoscopy and Frequency of Patient-Specific Factors Among Those With and Without a Perioperative Respiratory Adverse Event.

cyst removal, laryngeal cleft repair, dilation and steroid injection, etc.) ¥ including asthma, BPD **including T21, CP.
GERD = gastroesophageal reflux disease; URTI = upper respiratory tract infection; ASA = American Society of Anesthesiology; FB = foreign body; MLB = microlaryngoscopy and rigid bronchoscopy; PACU = post-anesthetic care unit.
Occurrence of postoperative respiratory events after MLB.

CCRT = critical care response team; ICU = intensive care unit; PEWS = pediatric early warning score.
Results
Overall Characteristics of the Study Population
Overall, 420 patients with a mean (SD) age at time of bronchoscopy of 39.4 (53.78) months were included in the study (Table 1). Of these, 172 (41%) were female. The most common underlying medical comorbidity was gastroesophageal reflux disease (GERD) (212, 50.5%), followed by prematurity (132, 31.4%), developmental delay (108, 25.7%), and cardiovascular disease (76, 18.1%). Most patients were ASA 3 (197, 46.9%) or ASA 4 (124, 29.5%). Indications for bronchoscopy were diagnostic alone (206, 49.0%), MLB plus interventions (112, 26.7%), MLB + supraglottoplasty (38, 9.0%), MLB + adenotonsillectomy (21, 5.0%), MLB + FB removal (43, 10.2%).
A description of significant postoperative respiratory events requiring escalation of care can be found in Table 2. Overall, 229 (54.5%) of patients had a significant postoperative respiratory event requiring escalation of care. Five patients (1.2%) had postoperative laryngospasm or bronchospasm in the PACU or ward, and 5 (1.2%) patients desaturated below 80% postoperatively. Fifteen patients (3.6%) required an unplanned assessment by the CCRT or escalation of care from the ward to the ICU. In terms of oxygen supplementation, 58 patients (13.8%) were admitted directly to the ICU for ventilatory requirements. Thirteen patients (3.1%) required oxygen by face mask, and 42 patients (10%) required heated high-flow.
Risk Factors for Postoperative Respiratory Events:
Of the 420 patients included in the analysis, several variables were found to be significantly associated with the postoperative respiratory events in multivariable logistic regression:
Figures 1 and 2 demonstrate the frequency of postoperative respiratory events for patients whose disposition was to a stepdown unit or ICU. Of those who were admitted to a stepdown unit, the frequency of postoperative respiratory events requiring escalation of care was greater than 50% for patients undergoing outpatient MLB + supraglottoplasty (53.5% n=8/15), inpatient MLB + supraglottoplasty (100% n=1/1), inpatient MLB alone (54.2% n=13/24), inpatient MLB + intervention (58.3% n=7/12), and outpatient MLB + intervention (51.5% n=34/67).
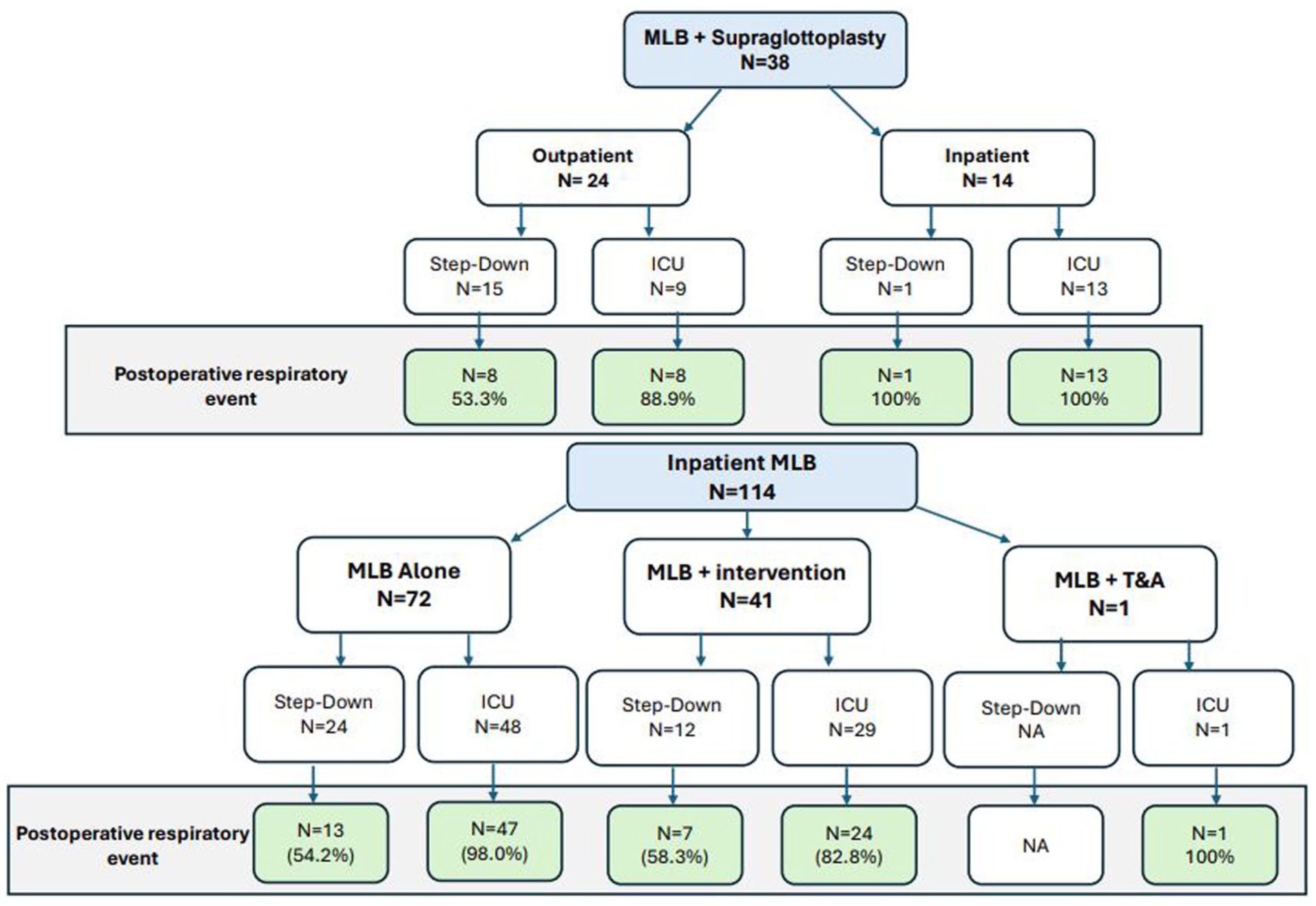
Postoperative disposition and respiratory events after MLB + supraglottoplasty and inpatient MLB. Green: >50% events.

Postoperative disposition and respiratory events after FB emergencies and outpatient elective MLB. Green: >50% events. Pink:<50% events
The frequency of postoperative respiratory events was less than 50% for patients in stepdown units who underwent MLB for a FB emergency (29%), outpatient elective MLB alone (31.3%), and MLB + T&A (33.3%) (Figure 2).
Separate multivariable logistic regression analysis limited to the subgroup of patients who underwent MLB alone (n=201) is demonstrated in Table 3 and identified male sex (OR 2.37, P = .04), prematurity (OR 0.20, P = .03), inpatient surgery (OR 5.66, p<0.01), and operative time ≥3 hours (OR 3.86, P = .02) as significant independent predictors of postoperative respiratory events.
Multivariate Logistic Regression Analysis Showing Odds Ratios Associated With Risk of Having A Major Respiratory Adverse Event for all MLB Procedures.

P < 0.05.
Discussion
Many institutions require patients to be admitted postoperatively following MLB to either a stepdown unit with 1:2 nursing or the ICU with 1:1 nursing. This can place a strain on systems with limited resources, but it may not be necessary. The present study demonstrated that patients undergoing MLB had a higher risk of having a postoperative respiratory event requiring escalation of care if they were between ages 1-2, had an underlying cardiovascular disease, GERD, medical complexity, including an ASA score of 4, undergoing MLB with supraglottoplasty, MLB as an emergency inpatient procedure or had an operative duration greater than 180 minutes. These higher-risk patients are appropriately suitable for a stepdown unit or ICU, while lower-risk patients could likely have safe deescalation to a standard ward bed.
MLB with supraglottoplasty, MLB + intervention, and inpatient MLB were associated with an increased risk of having a postoperative respiratory event requiring escalation of care. This is consistent with the literature, where MLB with supraglottoplasty has been shown to be associated with increased postoperative respiratory events and longer hospital length of stay. 9 The impact of supraglottoplasty on an infant’s postoperative course is dependent on both surgical and patient factors. At our institution, we employ a conservative surgical management strategy for laryngomalacia, which is reserved for patients in the very severe symptomatic range who have failure to thrive despite conservative feeding and nutritional supplementation strategies and a trial of medical management, usually consisting of proton pump inhibition. A survey of supraglottoplasty practice patterns in the United States, Canada, and the UK reported that 53% of surgeons routinely admit children to the ICU postoperatively. 10 Others have advocated for a stepdown unit with constant monitoring or admission directly to the ward. 11 Results from our study support initial routine postoperative admission to a stepdown unit and selective postoperative ICU admission, as previously described by Kang et al 9 who showed a significant reduction in ICU admission by 45% without increased morbidity or postoperative issues.
We identified an association between cardiovascular disease and a higher rate of postoperative complications following MLB, which has been previously described.4–6 Possible reasons for this association include smaller pulmonary reserve, lower residual volume, increased airway resistance, and nearly exclusive diaphragmatic breathing. These factors can all contribute to unique challenges when developing an appropriate and optimal anesthetic plan. More than 75% of our study population had an ASA class greater than 3, indicating a high degree of severe systemic disease and medical complexity in the studied population, potentially putting them at higher risk for intraoperative and postoperative respiratory complications than the general pediatric surgical population.
MLB with longer operative times was associated with an increased risk of postoperative complications. Longer operative time has been associated with a higher likelihood of postoperative reintubation in patients undergoing lung resection, and each 20-minute increase in operative time has been associated with a 24% increased risk of any complication following arthroplasty.12,13 Determinants of operative time are multifactorial, ranging from patient-specific and disease-specific factors (age, medical complexity, surgical anatomy) to center-specific or surgeon-specific factors (expertise of the surgeon, trainee participation). Results from our study indicate that operative time should be factored into the consideration for postoperative disposition.
Our findings indicate that age may be an important risk factor for postoperative respiratory events in this population. Specifically, children aged 1 to 2 years had significantly higher odds of adverse events (OR 2.47, 95% CI 1.06-5.84, P = .037), suggesting this developmental stage may confer unique vulnerability due to anatomical and physiological factors such as smaller airway caliber and increased airway reactivity. Although children aged 6 months to 1 year also had increased odds of adverse events (OR 1.97, 95% CI 0.83-4.76), this association did not reach statistical significance. No significant association was observed in children over 2 years of age. These findings underscore the importance of incorporating age-specific considerations into clinical assessment, perioperative planning, and risk stratification.
The decision to admit a patient after removal of an airway FB varies across institutions, and hospital mortality after bronchoscopy and FB retrieval has been reported as being 0.3%. 14 Andreoli et al found that 30/31 (96.7%) of patients who were extubated in the operating room returned to room air oxygenation within 2 hours of surgery and concluded that PACU observation and discharge are feasible in select children following airway foreign body extraction. 15 In our cohort, the 10 patients who experienced postoperative respiratory events after extubation primarily required only low-level respiratory support such as blow-by oxygen or heated high flow oxygen for more than 2 hours. These interventions reflect relatively mild respiratory events that did not necessitate reintubation or prolonged escalation of care.
Optimizing healthcare resources and expenditures is crucial. ICUs are high-intensity resources with significant costs, making their reduction desirable. Furthermore, a child’s admission to the ICU is a stressful event for parents and families. Transitioning to a less intensive environment may help alleviate some of this stress and anxiety. This study shows that the majority of patients can have the intensity of their care deescalated safely to a standard ward bed or stepdown unit, while still allowing selective ICU admission for patients with certain comorbidities, procedures, and underlying conditions. At our institution, the cost of a low-intensity standard ward (1:4 nursing) is $2,672 CAD/night, the cost of a stepdown unit (1:2 nursing) is $4,593 CAD/night, and the cost of the ICU (1:1 nursing) is $8,446 CAD/night.6,9 In our study, only 31.3% of patients undergoing MLB alone and 33.3% undergoing MLB with concurrent adenotonsillectomy experienced postoperative respiratory events, suggesting that a proportion of these patients are low-risk and could have been safely deescalated (Figure 2). In our study, among patients undergoing MLB alone, prematurity, inpatient emergencies, and procedures >180 minutes were independent risk factors for postoperative respiratory events. If these patients were identified as higher risk and allocated a stepdown unit postoperatively, and the remaining patients were allocated to a standard ward bed, 61 patients would have had their care deescalated. This would have freed up postoperative beds for other patients and resulted in a cost savings of $117,181.
To further optimize resource utilization, one consideration is same-day discharge for patients undergoing MLB without risk factors. In this study’s cohort, a substantial number of patients did not experience postoperative respiratory events. Prior studies on foreign body removal suggest that PACU monitoring followed by same-day discharge may be feasible and safe in specific pediatric patients, depending on risk factors. 15 Similarly, in low-risk MLB patients who do not have a history of cardiovascular disease, who did not undergo supraglottoplasty, have an ASA less than or equal to 3, and a duration of operation under 180 minutes, a similar same-day discharge protocol could be implemented. Same-day discharge in low-risk patients could yield additional cost savings and reduce inpatient unit burden. However, evaluating the efficacy of same-day discharge would require stringent patient selection criteria, adequate PACU monitoring, and patient follow-up.
A limitation of this study is that it is retrospective and reviewed patients in a single institution. As such, generalizability is limited by differences in the available postoperative care settings and practices at other institutions. Furthermore, because definitions and capabilities of these units may vary significantly across institutions, this may limit the interpretation of our results. Differences in resource availability, monitoring capacity, and respiratory support capabilities across settings should be considered when applying our findings to other contexts. The data does, however, illustrate the safe management of the majority of postoperative MLB patients outside of an ICU setting. Another limitation of this study is the broad categorization of procedures, particularly within the “MLB with endoscopic intervention” group, which encompasses a range of interventions with varying levels of complexity and risk. For example, cleft repair and balloon dilation differ significantly in duration, instrumentation, and perioperative risk, including the use of lasers that may increase the risk of airway fire. Similarly, foreign body removal via rigid bronchoscopy differs meaningfully from standard MLB. Procedures such as MLB combined with adenotonsillectomy may also skew disposition outcomes due to comorbid conditions like elevated AHI in patients with obstructive sleep apnea. While these groupings may mask important clinical heterogeneity, they were necessary to ensure adequate sample sizes and were aligned with institutional goals of developing broader, tiered postoperative care protocols. This trade-off between clinical granularity and practical utility should be considered when interpreting the findings and applying them to other settings. We focused this review on preoperative risk factors rather than intraoperative factors. Factors such as intraoperative desaturation, anesthetic type, and other intraoperative events may also increase the risk of postoperative complications. Whether the increased rate of postoperative events was related to the procedure itself or to the patient’s underlying condition could not be differentiated in our study, given the retrospective nature. We acknowledge that the inclusion of blow-by oxygen for ≥2 hours as a subclassification may introduce variability, as the actual oxygen delivery can differ depending on the distance of the mask from the patient’s face. We included it to capture the sustained need for respiratory support as a clinically relevant event. This limitation highlights the challenges of capturing precise oxygen supplementation retrospectively and may contribute to some heterogeneity in our primary outcome. Our study included postoperative respiratory events during emergence, in the PACU, and in the stepdown/ICU, recognizing that not all events equally influence ward versus stepdown and ICU disposition. 16 PACU and emergence events were included as markers of patient vulnerability that often guide clinical decisions. We intentionally kept the outcome definition broad to allow proactive allocation of higher-intensity beds rather than reacting on the day of surgery. While this may overestimate events relevant to ward disposition, it provides a comprehensive view of respiratory instability risk. Our findings identify predictors of postoperative events, but further prospective studies are needed to determine which events truly necessitate higher-acuity monitoring. Future research could stratify outcomes by timing to better identify factors predicting events that persist beyond initial anesthetic recovery.
Conclusion
Approximately one-half of patients following MLB had a postoperative respiratory event requiring an escalation in nursing care. This was more common in patients with CVD, GERD, ASA 4, MLB with supraglottoplasty, inpatient emergency, OR time >180 minutes. Tailoring postoperative disposition based on preoperative risk factors may result in a reduction in ICU utilization while ensuring patients are safely monitored in an appropriate setting.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.