
Abstract
Importance
A predictive formula for pediatric nasopharyngeal depth (ND) could tailor nasopharyngeal swabbing technique to individual anatomy and reduce the incidence of false negatives.
Objective
To provide a formula predicting ND based on surface anatomy measurements in children.
Study Design
Prospective pilot study.
Setting
British Columbia Children’s Hospital Pediatric Otolaryngology Clinic (Canada) between June 2022 to May 2024.
Participants
Children receiving flexible nasal endoscopy at a tertiary otolaryngology clinic.
Intervention and Main Outcome Measures
Predictor variables collected were sex, age, height, weight, curved nasal ala-tragus distance, finger lengths, and history of adenoidectomy. The outcome variable of ND was measured from the nasal nares to the posterior nasopharyngeal wall during routine nasal endoscopy. Relationships between predictor and outcome variables were analyzed. A predictive formula for ND was generated using stepwise linear regression, formula simplification, and model validation.
Results
Sixty-three pediatric patients were included (67% male, average age 6.4 years, range 3 weeks-18 years). ND differed by age: average ND for age <2 was 5.4 ± 0.8 cm, ages 2 to 10 was 7.4 ± 1.1 cm, and ages >10 was 9 ± 1.1 cm. Stepwise linear regression resulted in the formula: ND (cm) = ⅔ (pinky length) + ⅓ (ala-tragus distance) + 1 (if history of adenoidectomy) + 1. R2 was .78 with an average error of estimation ±0.81 cm.
Conclusion
Pediatric ND varies with age and surface anatomy dimensions. ND can be predicted in children using simple bedside measurements of pinky length, curved ala-tragus distance, and history of adenoidectomy using the equation ND (cm) = ⅔ (pinky length) + ⅓ (ala-tragus distance) + 1 (if history of adenoidectomy) + 1.
Relevance
Future studies are required to further validate the proposed predictive formula to ultimately improve accuracy in procedures involving blind instrumentation of the nasal cavity, such as nasopharyngeal swabs and posterior nasal packing.

Key Messages
Average nasopharyngeal depth (ND) for children of age <2 was 5.4 ± 0.8 cm, ages 2 to 10 was 7.4 ± 1.1 cm, and ages >10 was 9 ± 1.1 cm.
ND can be predicted with an R2 of .78 using the equation ND (cm) = ⅔ (pinky length) + ⅓ (ala-tragus distance) + 1 (if history of adenoidectomy) + 1.
Future studies can further validate this formula to provide an individually-tailored estimate of ND and improve accuracy in procedures involving blind instrumentation of the nasal cavity, such as nasopharyngeal swabs and posterior nasal packing.
Introduction
Nasopharyngeal depth (ND) is an important clinical measure in numerous clinical settings involving blind instrumentation of the nasal cavity. ND estimation is implicated in nasopharyngeal (NP) swabs, one of the most commonly used modalities to diagnose upper respiratory infections.1 -4 Proper NP swabbing technique with appropriate anatomical knowledge is needed to obtain a viable NP sample while minimizing discomfort and variability.5,6 Shallow depth of swab insertion has been associated with false negative results, 7 and deep swab insertion potentially increases the risk of rare complications.8 -14 Further, nasal packing for posterior epistaxis relies on appropriate NP placement to compress vessels while minimizing mucosal trauma, airway obstruction and the need for more invasive therapies. 15
Previous cadaver and radiographic studies have reported the average ND in adult and pediatric populations,16 -19 but to the best of our knowledge, Dickie et al is the only study to have created a formula predicting an individual’s ND based on unique anatomic measurements: ND (cm) = 0.73*(straight distance from tragus to philtrum) + 2.334. 20 However, no such formula has been validated for pediatric populations whose craniofacial proportions continue to change. 21 Children have low procedural tolerance and cooperation, making accurate predictions of ND is especially important to limit discomfort and reduce the need to repeat instrumentation.
The validation of a simple formula predicting ND could tailor NP instrumentation techniques based on individual anatomy, decrease discomfort, and reduce the incidence of false negative results for NP swabs. This pilot study thus seeks to establish proof of concept that external surface anatomy measurements can predict internal ND in a pediatric population despite disproportional body growth as children age. Secondarily, this study seeks to formulate an equation that can predict ND using demographic information and external measurements of the face and fingers.
Methods
Setting and Participants
This was a prospective, single-center pilot study conducted from June 2022 to May 2024. Informed consent was obtained from all patients, and the project was approved by the University of British Columbia Research Ethics Board (H22-01097). Participants were children aged 18 and under who received flexible nasal endoscopy as part of their care at BC Children’s Hospital Pediatric Otolaryngology Clinic. Patients were excluded if they could not complete the flexible endoscopy examination, had craniofacial syndromes (including trisomy 21), or if their families did not speak English for verbal consent.
Participant sex, age, ethnicity, history of adenoidectomy, and indication for flexible endoscopy were documented. Sex was based on the participant’s designation at birth. Patients’ height (cm), weight (kg), ala-tragus distance (cm), finger lengths (cm), and ND (cm) were collected. Ala-tragus distance was measured using a flexible measuring tape placed flush along the facial curvature from the alar rim of the nose to the tragus of the ear (Figure 1A). Finger length was measured from the fingertip to the palmar digital crease for all fingers of the right or left hand, excluding the thumb (Figure 1B). ND was measured from the nasal nares to the posterior NP wall during routine nasal endoscopy: a straightened flexible nasal endoscope was advanced along the nasal floor into the NP until camera guidance confirmed contact with the posterior NP wall. We then marked the endoscope at the nasal nares, removed the endoscope from the nasopharynx, and measured the endoscope length from end to marking.
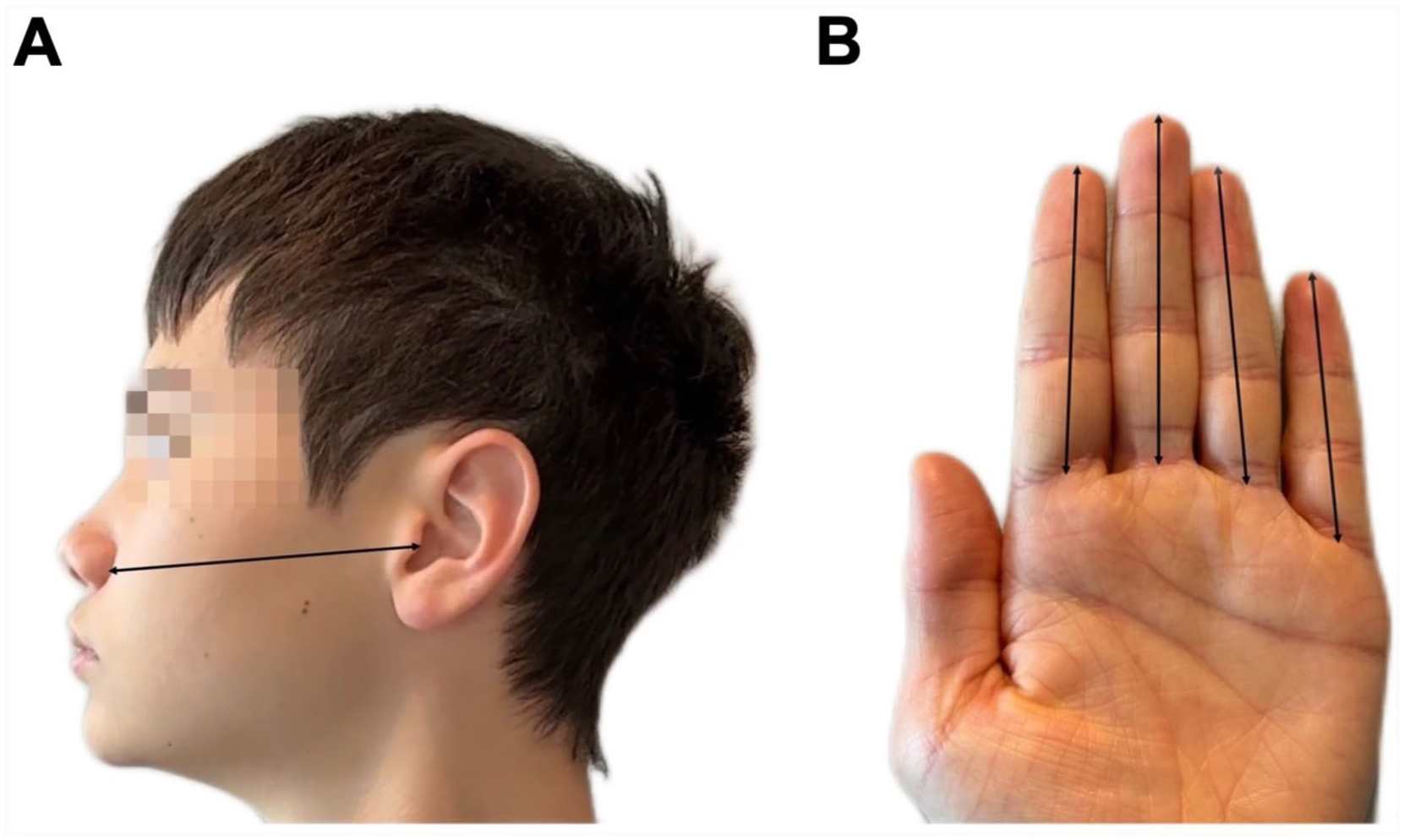
Anatomical measurements used to predict nasopharyngeal depth. (A) Ala-tragus distance and (B) Index, middle, ring, and pinky finger lengths.
Statistical Analysis
Patient demographics were summarized using descriptive statistics. Categorical variables were presented as counts and percentages. Continuous variables were presented as means and standard deviations (SD) where a normal distribution was assumed.
Six key stages were involved in generating an ND predictive equation:
The data was verified to meet the criteria for linear regression.
The data was split into randomized training subset and testing subset; this was repeated randomly 100 times.
Stepwise linear regression was performed with the training subsets.
The best model from step 3 was identified by highest R2.
The model from step 4 was simplified and rounded for convenience of use at bedside.
The rounded model was validated by comparing the root mean square error (RMSE) of the training and testing subsets.
The following criteria must be met for linear regression: the relationship between predictor and outcome variables must be linear, and there must be an absence of both multicolline-arity and high correlation between predictor variables. Multicollinearity was predefined as a variance inflation factor (VIF) exceeding 5. High correlation was defined as r ≥.70. 22
To separate the data for training and testing the model, we randomly generated 100 unique training and testing subsets. Seventy-five percent of the data was partitioned for the training subset, and 25% for the testing subset. We performed steps 3 to 6 on 100 training subsets and then calculated the average result across all subsets.
The best model generated by stepwise linear regression was identified via adjusted R2. The model with the highest adjusted R2 was simplified for ease of bedside use by rounding the coefficients and intercept.
Finally, we validated the simplified model by comparing the RMSE of training and testing subsets. A comparable RMSE indicated a generalizable equation for new incoming data. 22 All statistical analysis was carried out in R version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient Characteristics
A total of 63 children were included in this study (67% male, mean age 6.4 years, SD 5.3 years, range 3 weeks to 18 years). Six patients had a history of adenoidectomy. The average ND of all patients was 7.2 cm (range 3.4-10.7, SD 1.8). Average ND for age <2 was 5.4 ± 0.8 cm, ages 2 to 10 were 7.4 ± 1.1 cm, and ages >10 were 9 ± 1.1 cm. Patient characteristics are summarized in Table 1.
Patient Demographics.
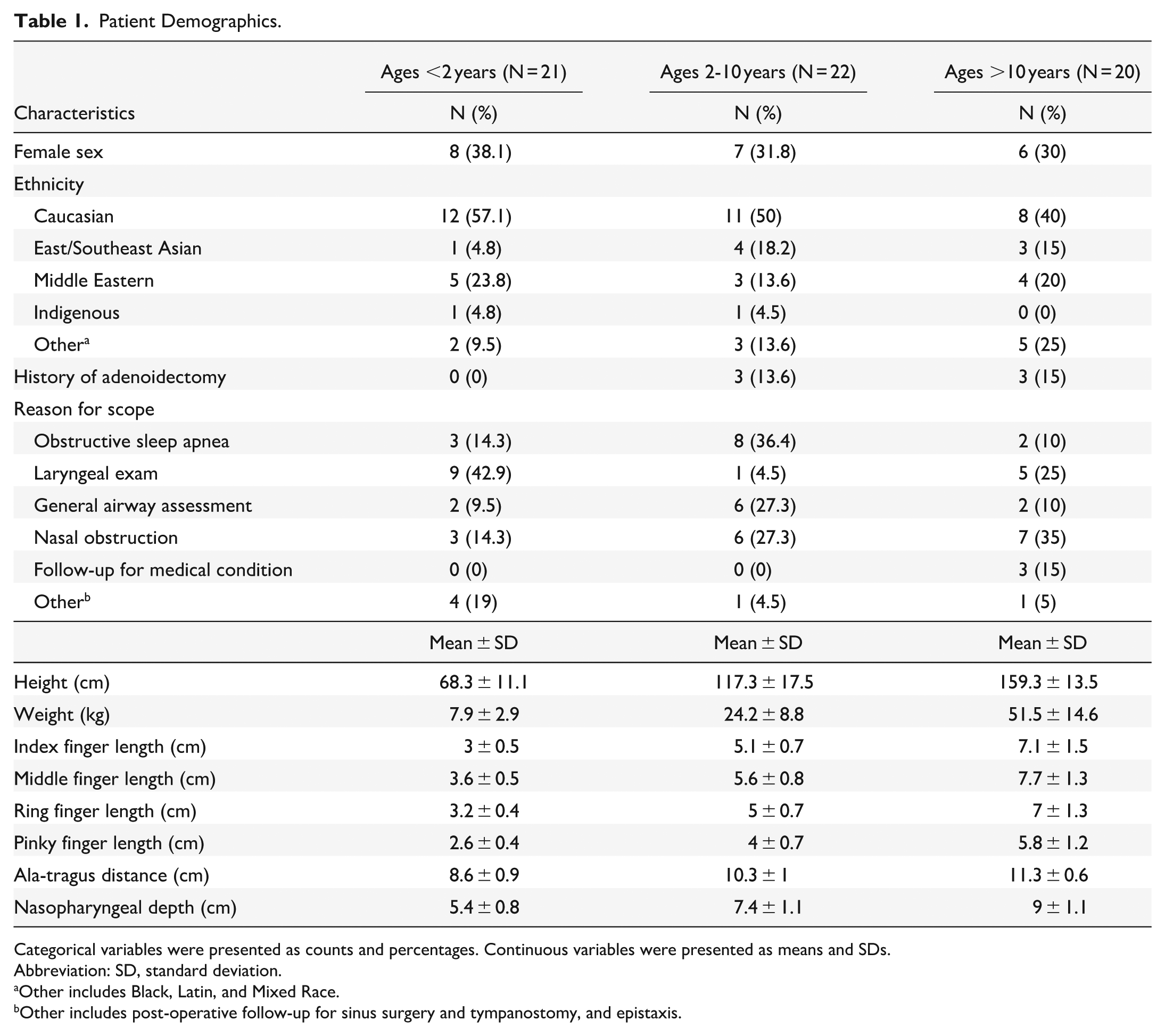
Categorical variables were presented as counts and percentages. Continuous variables were presented as means and SDs.
Abbreviation: SD, standard deviation.
Other includes Black, Latin, and Mixed Race.
Other includes post-operative follow-up for sinus surgery and tympanostomy, and epistaxis.
Model Creation
The statistical workflow is shown in Figure 2. The following predictor variables were considered for model creation: age, sex, height, weight, history of adenoidectomy, index, middle, ring and pinky finger lengths. The numeric predictor variables exhibited a linear relationship with ND, fulfilling one criterion for their use in linear regression modeling. Multicollinearity with VIF >5 and correlation r ≥.70 was detected for age (VIF 32.4), height (VIF 41.3), weight (VIF 10.2), index finger length (VIF 59.1), middle finger length (VIF 49.0), ring finger length (VIF 109.5), and pinky finger length (VIF 27.8). These 7 multicollinear predictor variables were independently input into stepwise linear regression, while the remaining non-multicollinear (VIF <5) predictor variables (ala-tragus distance, sex, history of adenoidectomy) remained constant. Stepwise linear regression using 100 training subsets on these 7 variable combinations resulted in 700 models.

Statistical overview of model generation steps. Hx Adeno, history of adenoidectomy; Index, length of second digit (cm); Middle, length of third digit (cm); Ring, length of fourth digit (cm); Pinky, length of fifth digit (cm); AT, ala-tragus distance(cm); VIF, variance inflation factor; ND, nasopharyngeal depth (cm); RMSE, root mean squared error.
Determining the Best Model
Between 70% and 80% of the models generated by linear regression for each of the 7 variable combinations excluded the predictor variable of sex. This demonstrated that including the sex variable was suboptimal for the majority of randomized training subsets, so these models were discarded. The best variable combination was determined by adjusted R2, with the highest adjusted R2 being for the combination that included the pinky variable. Using coefficients averaged from the training subsets, we arrived at the equation: “ND (cm) = 0.68 (pinky) + 0.36 (ala-tragus distance) + 1.25 (history of adenoidectomy) + 0.70” (adjusted R2 = .79). The average R2 values for models from other variable combinations are shown in Figure 2.
Model Simplification
We arbitrarily simplified the formula to “ND (cm) = ⅔ (pinky length) + ⅓ (ala-tragus distance) + 1 (if history of adenoidectomy) + 1” to attempt to make it more practical to administer. This modification was then tested, and the adjusted R2 was .78. Therefore, the R2 for the simplified model was deemed very comparable to that of the original model (R2 = .78 vs .79, respectively), indicating that this fit was maintained after the simplification.
Model Validation
To visually confirm model fit, we plotted measured ND versus predicted ND for the original (Figure 3A) and simplified models (Figure 3B). In both plots, the points lie along a straight line with a slope of 1, indicating a good model fit. The standardized residuals of both the original and simplified models are randomly distributed around zero, further indicating a good model fit.

(A) Nasopharyngeal depth (cm) measured by flexible nasal endoscopy (“actual value for ND”) versus predicted nasopharyngeal depth using the unrounded equation, “ND (cm) = 0.68 (pinky length) + 0.36 (ala-tragus distance) + 1.25 (history of adenoidectomy) + 0.70.” (B) Standardized differences between predicted and actual ND values using the unsimplified equation. Each dot represents a residual value. Residuals near zero indicate accurate predictions. (C) Nasopharyngeal depth (cm) measured by flexible nasal endoscopy (“actual value for ND”) versus predicted nasopharyngeal depth using the simplified equation, “ND (cm) = ⅔ (pinky length) + ⅓ (ala-tragus distance) + 1 (if history of adenoidectomy) + 1.” (D) Standardized differences between predicted and actual ND values using the simplified equation. Each dot represents a residual value. Residuals near zero indicate accurate predictions. ND, nasopharyngeal depth.
Finally, we found that the average RMSEs of the training and testing subsets were highly comparable (RMSE = 0.81 vs 0.83, respectively), signifying the model’s generalizability to new data. Since RMSE indicates error in the same units as the outcome variable, an RMSE of 0.81 means the simplified formula predicts ND with an error of ±0.81 cm.
Discussion
The results of this pilot study showed that pediatric ND varies with age and can be predicted using surface body dimension measurements. The average ND for age <2 was 5.4 ± 0.8 cm, ages 2 to 10 were 7.4 ± 1.1 cm, and ages >10 were 9 ± 1.1 cm. Among the 10 predictor variables analyzed in this study, a combination of 3 measurements predicted ND in children using the equation “ND (cm) = ⅔ (pinky length) + ⅓ (ala-tragus distance) + 1 (if history of adenoidectomy) + 1.”
The NDs found in the current pilot study are in agreement with those found by Goracci et al who used lateral skull x-ray measurements and reported a mean ND of 5.7 cm for children of age <4, ages 5 to 9 was 7.1 cm for ages 5 to 9, and 8.0 cm for ages 10 to 14. 19 The comparability between our clinically-measured data and Goraci et al’s radiographically-measured data offers criterion validity for the measurement of nasopharyngeal dimensions.
A novel predictor variable tested in the current pilot study is the history of adenoidectomy, a relatively prevalent procedure in pediatric populations. Our findings indicate that the history of adenoidectomy influences ND prediction, with a difference of approximately 1 cm observed between individuals with and without a history of adenoidectomy. This finding is consistent with the average size of enlarged adenoids, which measures approximately 1.12 cm, 23 aligning well with the “+1 cm if history of adenoidectomy” parameter used in our predictive formula. However, this pilot study included a limited number of children with a history of adenoidectomy, which may restrict the generalizability of the findings.
The predictor variable of finger length has been studied in previous studies for the estimation of upper airway dimensions. Finger length has been validated to predict tracheal tube insertion depth24,25 and assess maxillary and mandibular dimensions for orthodontic procedures.26 -31 These studies offer convergent validity that external measurements can be utilized to estimate the internal dimensions of the head and neck without the need for radiographic data.
Our pilot ND model for pediatric populations is comparable to past studies investigating clinical predictors of ND among adults. Dickie et al proposed the equation “ND (cm) = 0.73*(straight distance from tragus to philtrum) + 2.334,” with an average error of estimation of ±0.03 cm and R2 of .64. 20 ND was measured using the same method as our study via flexible nasal endoscopy. They found that ND had a stronger correlation with the straight, tangential distance from the philtrum to the tragus (r = .775) than the curved distance along the facial margin from the nasal ala to the tragus (r = .598). Our study employed the latter curved distance from the nasal ala to tragus, given the procedural difficulty of accurately measuring a tangent on a moving child. Our final model also obtained a higher R2 of .78 compared to the R2 of .64 obtained by Dickie et al. It is possible that the larger number of predictor variables tested for formula development in the current study (10 variables tested vs 4 tested by Dickie et al) offered greater accuracy of predictions. In addition, since the study from Dickie et al is based on an adult population, their findings may not be generalizable to a pediatric population, as it is unlikely to account for changing craniofacial ratios in growing children.
A particularly relevant clinical application of this pilot study’s ND equation is in improving diagnostic accuracy of NP swabs by guiding depth of swab insertion. The current study found that ND changes with age and external body dimensions; therefore, the depth of NP swab insertion should be tailored to the diverse sizes of pediatric patients to ensure viable sample collection and reduction of false negative results.
This is especially relevant given that current NP swab insertion guidelines are vague and heterogeneous across health authorities. The Ontario, Canadian, and American Centers for Disease Control recommend inserting an NP swab “until it reaches the nasopharynx and/or resistance is met.”32,33 However, resistance may be encountered due to contact with internal nasal structures other than the posterior NP wall, such as turbinates or a deviated nasal septum, which could decrease the sensitivity of the swabs.8,16 Meanwhile, the BC Provincial Health Authority recommends approximating NP swab depth as the distance from the nostril to the ear in children. 34 However, it does not specify the specific part of the ear or nose to landmark measurements, nor does it detail whether the measurement is the curved distance along the facial margin or the straight tangential distance across the face. These ambiguities limit the sensitivity of NP swabs, and improper swabbing technique has been identified as a pervasive cause for false negative results. 8
To test how our model compares to the BC pediatric NP swabbing guideline, 34 let us apply the 2 models on a theoretical patient whose dimensions are equal to our sample average: ND (cm) = 7.2 cm, pinky length = 4.1 cm, distance from nasal ala to tragus = 10.0 cm, and no history of adenoidectomy. Our model states that “ND (cm) = ⅔ (pinky length) + ⅓ (ala-tragus) + 1 (if history of adenoidectomy) + 1,” resulting in a predicted ND of ⅔ (4.11) + ⅓ (10.0) + 0 + 1 = 7 cm for this theoretical patient. In contrast, ND per BC guidelines is “ND = ala-tragus distance,” resulting in a predicted ND of 10 cm. The BC guidelines overestimated ND by 3 cm, while our model differed from the actual depth by only 0.2 cm for this hypothetical patient.
To make the current study’s ND formula user-friendly in the busy clinical setting, we integrated the formula into a web calculator https://tinyurl.com/bp9nndtn created using ActiveCalculator.com. The website prompts inputs of pinky length, ala-tragus distance measure with measuring tape, and history of adenoidectomy to output ND. Future integration of this algorithm with established medical calculator apps could further support the clinical practicality of this study’s ND formula.
Limitations and Future Directions
Given that this is a pilot study, the current findings are intended to offer proof of concept and are limited in generalizability. The findings should not be applied to children with craniofacial syndromes, as this group was excluded from our study. The racial heterogeneity of our sample reflects the diversity of Vancouver, British Columbia, Canada, which precluded the evaluation of relationships between race and ND as described in previous studies.16 -18 Larger sample size is needed to validate the formula and potentially expand the scope of variables evaluated, in addition to expanding the study population to encompass greater ethnic diversity and individuals with craniofacial syndromes.
In addition, our sample trended younger in age, with many participants being of ages 0 to 4 years, which could limit generalizability in older pediatric patients. However, this could be serendipitously appropriate since a point-of-care ND prediction would be most useful for younger children with lower tolerance for clinical procedures.35 -37
Conclusions
Pediatric ND varies with age and surface anatomy dimensions. Simple bedside measurements can be sufficient in predicting ND with an R2 of .78 using the equation ND (cm) = ⅔ (pinky length) + ⅓ (ala-tragus distance) + 1 (if history of adenoidectomy) + 1. Future studies can further validate this pilot predictive formula to provide an individually-tailored estimate of ND and ultimately improve accuracy in procedures involving blind instrumentation of the nasal cavity, such as nasopharyngeal swabs and posterior nasal packing.
Footnotes
Acknowledgements
We would like to thank Dr. Juan-Carlos Hernaiz Leonardo for his statistical recommendations and Ms. Julie Pauwels for her administrative support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The project was approved by the University of British Columbia Research Ethics Board (H22-01097).
Consent to Participate
Informed verbal consent was obtained from all patients prior to enrollment.
Consent for Publication
Informed verbal consent was obtained from all patients for publication.
Data Availability Statement
Data is available from the corresponding author on request.