
Abstract
Importance
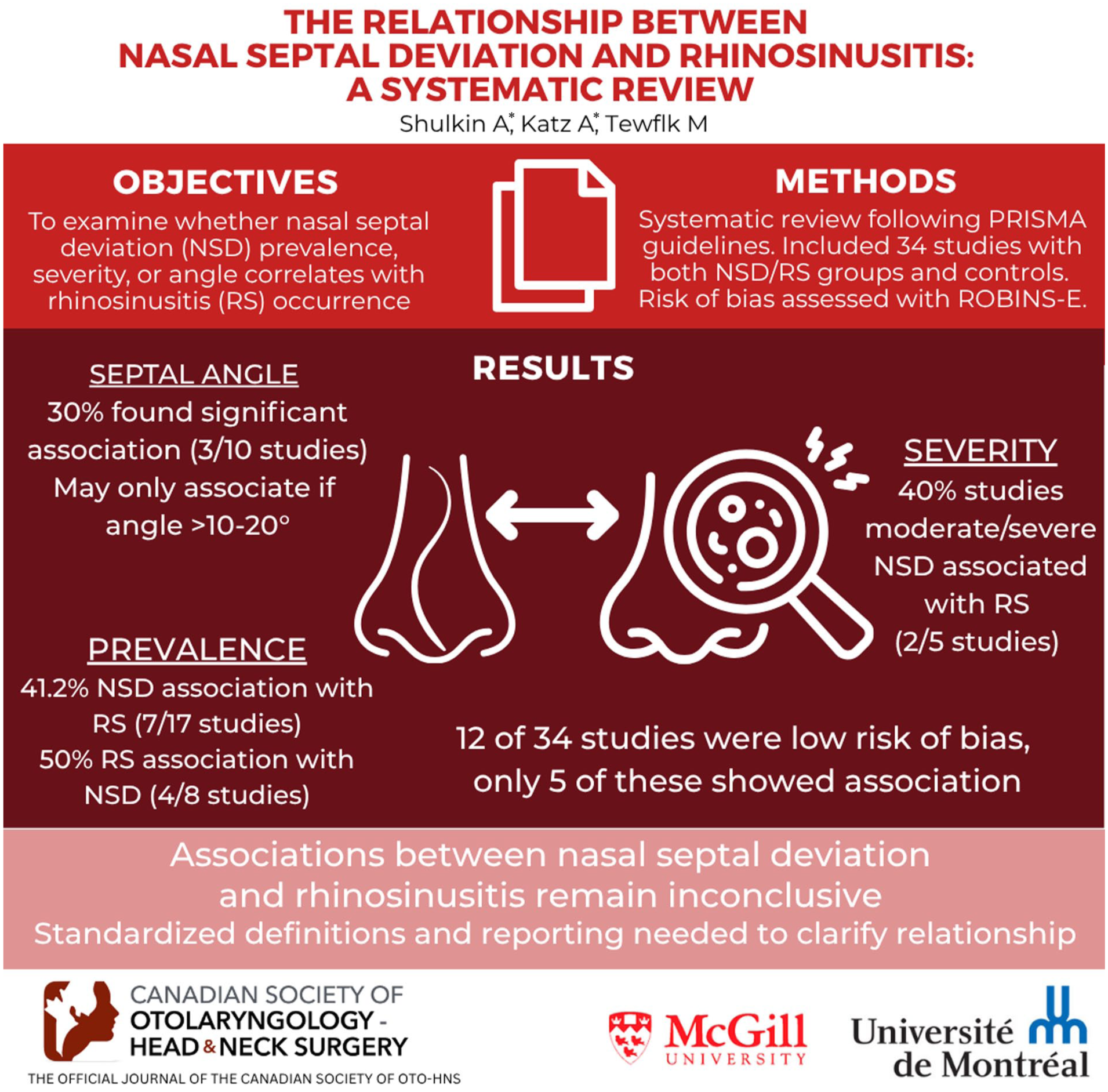
Nasal septal deviation (NSD) and rhinosinusitis (RS) are common conditions with overlapping symptoms, yet they require distinct treatment approaches. Clarifying their relationship is essential to guide preventative management strategies.
Objective
To examine the association between NSD and RS.
Design
Systematic review following the PRISMA guidelines. Embase, MEDLINE, and Web of Science were searched from inception to January 2025.
Participants
Studies were included if participants were adults (≥18 years); studies conducted exclusively in pediatric populations were excluded.
Main Outcome Measures
Association between NSD and RS based on prevalence, NSD severity, and mean nasal septal angle (NSA), as well as overall study quality and risk of bias.
Results
A total of 34 studies were included, of which 26 reported NSD and 8 reported RS as their primary outcome. Among the studies reporting on NSD, 17 assessed prevalence, of which 7 (41.2%) demonstrated an association with RS; 5 assessed severity, of which 2 (40.0%) demonstrated an association between moderate/severe NSD and RS; and 10 assessed mean NSA, of which 3 (30.0%) demonstrated an association with RS. All studies reporting on RS assessed prevalence, of which 4 (50.0%) demonstrated an association with NSD. Overall, 16/40 (40.0%) individual outcome measures indicated an association between NSD and RS. A risk of bias analysis identified 12/34 (35.3%) studies as low risk. Of these, 5/17 (29.4%) individual outcomes measures demonstrated an association between NSD and RS.
Conclusion
The current body of evidence reveals an inconclusive relationship between NSD and RS. Variability in definitions, diagnostic criteria, and outcome measures, combined with insufficient control for bias, limit the ability to draw definitive conclusions.
Relevance:
We propose standardized reporting guidelines to ensure consistency across studies and enable more meaningful comparisons. Implementing this framework may ultimately support the development of preventative strategies to optimize patient outcomes.
PROSPERO registration number
CRD42024514049.
Key Message
- Current evidence demonstrates an unclear association between nasal septal deviation and rhinosinusitis.
- Heterogeneity in definitions, diagnostic criteria, and outcome measures, along with limited bias control, hinder the ability to draw definitive conclusions.
- We propose a standardized reporting framework to ensure consistency across studies and facilitate more reliable comparisons of findings.
Introduction
Nasal obstruction is among the most frequent reasons for patients to seek treatment from primary care physicians, otolaryngologists, and allergists. 1 While some clinicians interpret it as a physical blockage within the nasal cavity, it is more frequently understood as a sensation of inadequate airflow through the nose. 2 This symptom can be indicative of various common conditions, such as nasal septal deviation (NSD) and rhinosinusitis (RS).
RS is characterized by inflammation of the paranasal sinuses and nasal cavity mucosa. According to the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS) criteria, 3 RS is defined by the presence of two or more symptoms, including nasal blockage, obstruction, congestion, or nasal discharge, facial pain/pressure and hyposmia/anosmia. Endoscopic signs and/or computed tomography (CT) findings must be present to confirm a diagnosis. Endoscopic signs include nasal polyps, mucopurulent discharge, and edema/mucosal obstruction. CT findings include mucosal thickening/opacification within the ostiomeatal complex and paranasal sinuses.
The nasal septum, an osseocartilaginous structure that divides the nasal cavities, is lined with mucosa composed of a basement membrane, lamina propria, and ciliated columnar cells. 4 It is vital for maintaining proper nasal airflow and overall respiratory health. 5 Minor NSD is common, typically asymptomatic, and considered a normal anatomical variation. In contrast, severe NSD can cause nasal obstruction and lead to symptoms that overlap with those of RS. 6
Treatment approaches differ markedly: NSD is often managed surgically with procedures such as septoplasty, while RS treatment focuses on addressing its underlying cause, typically with nasal saline, decongestants, corticosteroids, antibiotics, or biological agents.7 -10 Endoscopic sinus surgery (ESS) can also improve the symptoms of RS for more severe or refractory cases. 11 Furthermore, evidence suggests that performing septoplasty concurrently with ESS is associated with a significantly reduced 5-year revision rate, 12 highlighting the potential benefits of addressing NSD during surgical interventions for RS.
A potential relationship between NSD and RS has been suggested in the literature. A systematic review by Orlandi in 2010 13 found a relationship between the 2 conditions, suggesting that NSD may contribute to the development or exacerbation of RS. However, a literature review conducted by Collet et al in 2001 14 found no significant link between the 2 pathologies. More recent studies have yielded conflicting results, highlighting the complexity of this relationship.
Establishing whether a true association exists is important, as it could inform preventive strategies in individuals with NSD to reduce their risk of developing RS, whether it be acute or chronic. Conversely, if no such association is present, interventions such as septoplasty should be reserved for symptomatic NSD, thereby avoiding unnecessary procedures and their associated risks. Thus, in this systematic review, we sought to clarify the relationship between NSD and RS to elucidate underlying mechanisms, optimize clinical management, and ultimately improve patient outcomes.
Methods
Protocol and Registration
A protocol for this systematic review was published on PROSPERO (registration number: CRD42024514049) in February 2024.
Search Strategy
Our review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. 15 We searched 3 electronic databases, namely, Embase, MEDLINE, and Web of Science initially on February 24, 2024, which was updated on January 6, 2025. The search terms included permutations of “nasal septal deviation” and “sinusitis.” Studies published from inception were included. The search strategy was reviewed and validated by an experienced health sciences librarian. A detailed search strategy for each database is provided in Supplemental Appendix I.
Inclusion and Exclusion Criteria
Studies were included if they met the following criteria: (1) published in English or French; (2) full-text availability; (3) randomized controlled trials, cohort studies, case-control studies, observational studies, or cross-sectional studies; (4) included a study group with NSD or RS and a control group; (5) analyzed the relationship between NSD and RS. Studies were included if most participants were adults (≥18 years), while those conducted exclusively in pediatric populations were excluded. The search was restricted to studies involving human subjects. Studies were excluded if they were reviews, meta-analyses, case reports or case series.
Study Selection
Two reviewers (A.S., A.K.) independently screened and selected eligible studies using Covidence. 16 Following the removal of duplicates and a title/abstract review, full-text manuscripts of potentially-relevant studies were retrieved and assessed based on inclusion/exclusion criteria. Any disagreements were reconciled by a third independent reviewer (M.A.T.). Reviewers contacted eligible study authors if they lacked necessary information, full text or required clarifications. If no response was received after 2 e-mails were sent, the article was omitted. Two reviewers (A.S., A.K.) manually searched the bibliographic references of all included articles to ensure all eligible articles were included.
Data Extraction
Two reviewers (A.S., A.K.) independently performed data extraction in duplicate, employing a standardized data collection form designed a priori on Microsoft Excel. 17 Any disagreements were reconciled by a third independent reviewer (M.A.T.). In selected studies, study characteristics, participant demographics, clinical findings, interventions, outcomes, outcome measures, and classification systems were extracted and summarized. Studies were grouped according to their primary outcome: NSD or RS. These studies were further categorized according to their reported outcome measure(s). Sub-analyses were conducted to separately assess the studies that reported a nasal septal angle (NSA) ≥10°, included subjects with chronic rhinosinusitis (CRS), and were classified as low risk of bias.
Bias Assessment
Two reviewers (A.S., A.K.) independently appraised the included articles using the Risk of Bias in Non-Randomized Studies - of Exposure (ROBINS-E) tool. 18 Any disagreements were reconciled by a third independent reviewer (M.A.T.).
Results
Study Selection
In total, 2551 references were identified, retrieved, and exported to Covidence. 16 Duplicates were eliminated, followed by an initial screening of 1600 article titles/abstracts. The remaining 266 articles were reviewed in full, and inclusion/exclusion criteria were applied. Overall, 34 studies were included in the review. A detailed flow diagram of the article selection process is provided in Figure 1.

Flow diagram of the article selection process.
Study Characteristics
Studies were categorized based on their primary outcome, with 26 reporting on NSD and 8 on RS.
Among those assessing NSD, participants frequently presented with CRS (n = 8, 30.8%) or unspecified RS (n = 8, 30.8%). Diagnosis was most often based on clinical manifestations combined with imaging or endoscopic findings (n = 19, 73.1%). Control groups were typically defined by the absence of both clinical and imaging/endoscopic findings (n = 10, 38.5%) or by the absence of clinical symptoms alone (n = 9, 34.6%). Confirmation and measurement of NSD were usually performed with a CT scan (n = 24, 92.3%). Studies were further grouped according to their reported outcome measure(s). Mean NSA was the most common (n = 10, 31.3%), followed by undefined NSD prevalence (n = 9, 28.1%), defined NSD prevalence (n = 8, 25.0%) and NSD severity (n = 5, 15.6%).
Among those assessing RS, participants were typically diagnosed with NSD using a CT scan (n = 7, 87.5%). NSD was undefined, or reported without explicit criteria, in half of the studies (n = 4, 50.0%). Control groups consisted of individuals without NSD, as confirmed by imaging (n = 7, 87.5%). All studies reported RS in terms of prevalence (n = 8, 100.0%), including subtypes such as CRS, unspecified RS, maxillary sinusitis, and pansinusitis. This was usually determined by the presence of clinical manifestations and imaging/endoscopy findings (n = 5, 62.5%).
An overview of study characteristics is provided in Table 1.
Study Characteristics.

Abbreviations: AIFR, acute invasive fungal rhinosinusitis; CRS, chronic rhinosinusitis; MSFB, maxillary sinus fungal ball; NSA, nasal septal angle; NSD, nasal septal deviation; RARS, recurrent acute rhinosinusitis; RS, rhinosinusitis.
CRS and MSFB (n = 1), CRS and RARS (n = 1).
Certain studies included multiple outcome measures.
Defined NSD refers to the use of explicit diagnostic criteria (eg, NSA cutoff).
CRS (n = 2), unspecified RS (n = 2), maxillary sinusitis (n = 1), pansinusitis (n = 1), undefined (n = 2).
Outcomes
Studies reporting NSD as primary outcome
Studies reporting NSD as the primary outcome were divided into 4 categories based on the specific outcome measure(s) applied: (a) prevalence of undefined NSD, (b) prevalence of defined NSD, (c) prevalence of NSD by severity, and (d) mean NSA. These outcome measures were obtained from cohorts stratified by the presence or absence of RS.
Prevalence of undefined NSD
The prevalence of NSD without clearly defined criteria was assessed in 9 studies. Of these, 5 studies found no association (55.6%),19 -23 while 4 did (44.4%).24 -27 Individual study characteristics and findings are provided in Table 2.
Prevalence of Undefined NSD Based on Presence/Absence of RS.

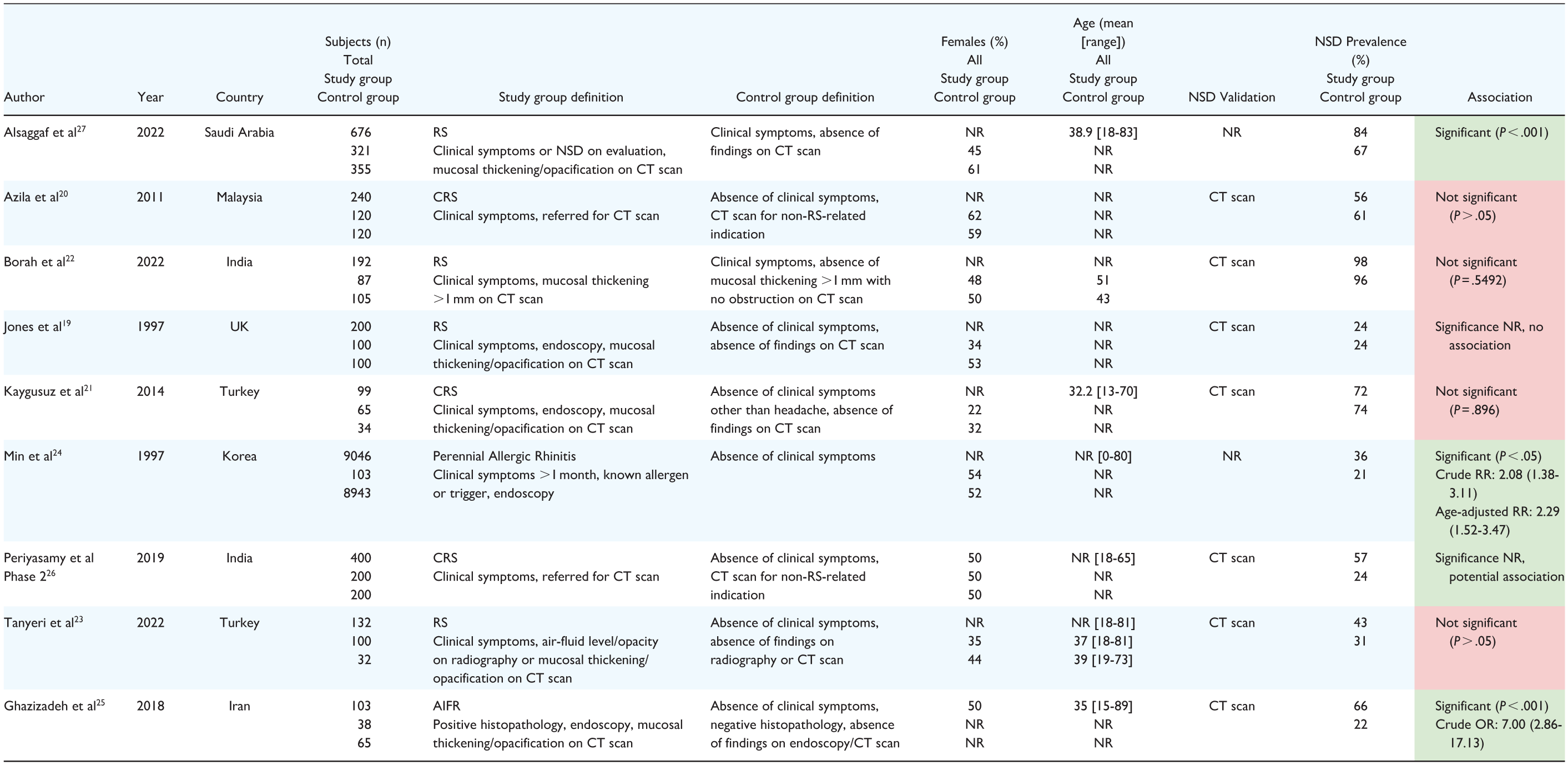
Green represents that the article found a significant association between NSD and RS, whereas red represents that there was no association found or that it was not reported.
Abbreviations: AIFR, acute invasive fungal rhinosinusitis; CRS, chronic rhinosinusitis; CT, computed tomography; NR, not reported; NSD, nasal septal deviation; RS, rhinosinusitis; UK, United Kingdom.
Prevalence of defined NSD
Eight studies evaluated the prevalence of NSD with clearly defined criteria. Four studies used an NSA cutoff, 2 used a millimetric cutoff, and 2 defined NSD based on the extent of nasal cavity obstruction. Of these, 5 studies found no association (62.5%),28,29,31,33,34 while 3 did (37.5%).30,32,35 Individual study characteristics and findings are provided in Table 3.
Prevalence of Defined NSD Based on the Presence/Absence of RS.
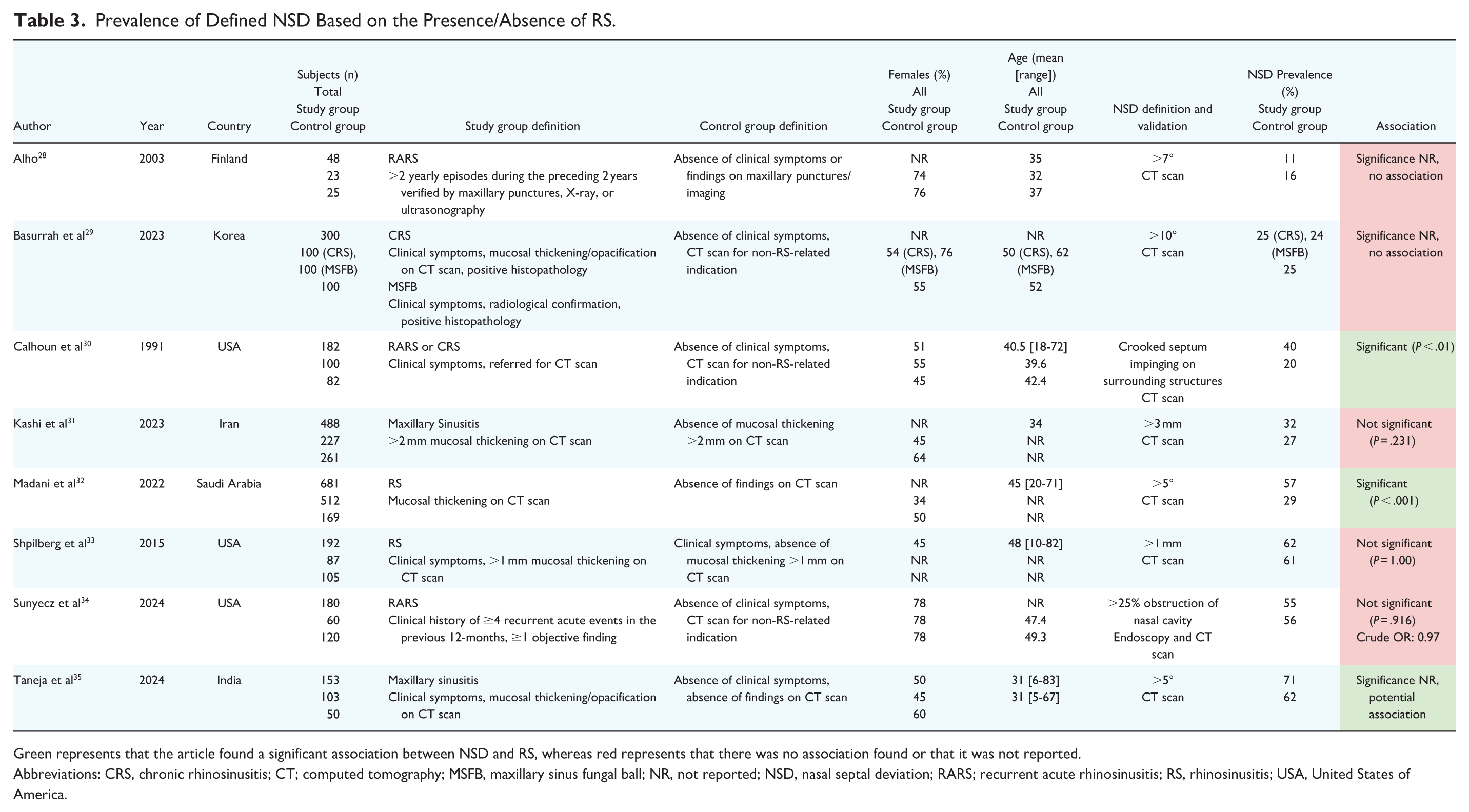

Green represents that the article found a significant association between NSD and RS, whereas red represents that there was no association found or that it was not reported.
Abbreviations: CRS, chronic rhinosinusitis; CT; computed tomography; MSFB, maxillary sinus fungal ball; NR, not reported; NSD, nasal septal deviation; RARS; recurrent acute rhinosinusitis; RS, rhinosinusitis; USA, United States of America.
Prevalence of NSD by severity
Five studies assessed the prevalence of NSD based on severity. Of these, 2 studies (40.0%) found that moderate and severe NSDs were more prevalent in CRS patients than in controls.37,40 Three studies (60.0%) demonstrated no such association.26,36,38 Individual study characteristics and findings are provided in Table 4.
Prevalence of NSD Severity Based on the Presence/Absence of RS.


Green represents that the article found a significant association between NSD and RS, whereas red represents that there was no association found or that it was not reported.
Abbreviations: CRS, chronic rhinosinusitis; CT, computed tomography; EPOS, European Position Paper on Rhinosinusitis and Nasal Polyps; NR, not reported; NSD, nasal septal deviation; RS, rhinosinusitis; RSTF, rhinosinusitis task force.
Mean NSA
Ten studies evaluated the mean NSA between groups. Seven studies (70.0%) found no association,36,37,38,41,42,44,45 while 3 (30.0%) did.35,40,43 Individual study characteristics and findings are provided in Table 5.
Mean NSA Based on the Presence/Absence of RS.


Green represents that the article found a significant association between NSD and RS, whereas red represents that there was no association found or that it was not reported.
Abbreviations: CRS, chronic rhinosinusitis; CT, computed tomography; EPOS, European Position Paper on Rhinosinusitis and Nasal Polyps; NR, not reported; MSFB, maxillary sinus fungal ball; NSA, nasal septal angle; NSD, nasal septal deviation; RS, rhinosinusitis; RSTF, rhinosinusitis task force; UK, United Kingdom; USA, United States of America.
Studies reporting RS as primary outcome
All studies reporting RS as the primary outcome used prevalence as their outcome measure.
Prevalence of RS
Seven studies assessed the prevalence of RS in cohorts stratified by the presence or absence of NSD. Of these, 4 studies (57.1%) found no difference between the study and control groups,46 -49 while 3 studies (42.9%) reported an association.50 -52 One study examined the prevalence of RS in relation to NSD severity. 53 The only statistically-significant finding was in individuals with severe NSD (>20°) when compared to the control group (56% vs 33%, P = .035). Individual study characteristics and findings are provided in Tables 6 and 7.
Prevalence of RS Based on the Presence/Absence of NSD.


Green represents that the article found a significant association between NSD and RS, whereas red represents that there was no association found or that it was not reported.
Abbreviations: CRS, chronic rhinosinusitis; CT, computed tomography; NR, not reported; NSA, nasal septal angle; NSD, nasal septal deviation; PNS, paranasal sinus; RS, rhinosinusitis; USA, United States of America.
Prevalence of RS Based on NSD Severity.


Green represents that the article found a significant association between NSD and RS.
Abbreviations: CT, computed tomography; NR, not reported; NSD, nasal septal deviation; RS, rhinosinusitis.
Studies reporting an NSA ≥10°
Of the included studies, 10 (29.4%) reported or subdivided subjects based on an NSA ≥10°.26,29,35,37,40,38,36,41,44,53 Among them, researchers evaluated 11 individual outcome measures. Four (36.4%) demonstrated an association in those with an NSA ≥10°, while one (9.1%) demonstrated an association in those with an NSA >20°.
Elahi et al, 37 Nikkerdar et al, 40 Cho et al, 36 and Greguric et al 38 stratified patients into mild (0-9°), moderate (10-15°), and severe (>15°) NSD groups. This categorization was applied to individuals with a diagnosis of CRS based on clinical manifestations and imaging/endoscopic findings, and controls without signs/symptoms. Two of these studies found a considerably higher prevalence of moderate-to-severe NSD among CRS cases,37,40 whereas two did not.36,38 Periyasamy et al 26 used similar stratification methods in individuals with CRS based on clinical manifestations alone and asymptomatic controls. However, there were no marked differences between groups.
Basurrah et al 29 applied an NSD cutoff of >10°. The study included individuals with CRS and maxillary sinus fungal ball (MSFB), diagnosed based on clinical manifestations and imaging/endoscopic findings, and controls without signs/symptoms. There was minimal variation in NSD prevalence across the groups, suggesting no significant association.
Alkire et al, 41 Nikkerdar et al, 40 Sadr et al, 44 and Taneja et al 35 analyzed the mean NSA in individuals with recurrent acute rhinosinusitis (RARS), CRS, unspecified RS, and maxillary sinusitis, respectively. These diagnoses were made based on the presence of clinical manifestations and imaging/endoscopy findings, whereas controls were asymptomatic. Although Alkire et al 41 and Sadr et al 44 demonstrated mean NSAs of >10° in the study groups, when compared to the control groups, these differences were not statistically significant. In contrast, Nikkerdar et al 40 and Taneja et al 35 found significantly larger mean NSAs (>10°) in study subjects.
Lastly, Yasan et al 53 compared subjects with and without NSD based on imaging confirmation. They reported that only patients with severe NSD (>20°) had a significantly higher prevalence of RS, although precise diagnostic criteria were not defined.
Chronic rhinosinusitis
Among the studies identified, 11 (32.4%) reported specifically on subjects with CRS.20,21,26,29,37,30,38,36,42,48,50 Within these studies, researchers evaluated 16 individual outcome measures. Five (40.0%) demonstrated an association.
Azila et al 20 and Periyasamy et al, 26 in its second phase, compared the prevalence of NSD in subjects with clinical manifestations of CRS to asymptomatic controls. Azila et al 20 demonstrated no significant association, whereas Periyasamy et al 26 revealed a significant relationship. Kaygusuz et al 21 conducted the same study design, but instead enrolled subjects with both clinical manifestations and imaging/endoscopy findings of CRS. They revealed no significant difference between the study and healthy control groups. It is worth noting that for these studies, explicit NSD diagnostic criteria were not provided. In contrast, Basurrah et al, 29 as previously described, implemented an NSD cutoff of >10°. Nonetheless, no association was revealed between those with CRS and asymptomatic controls.
As outlined earlier, Elahi et al 37 and Nikkerdar et al 40 found a considerably higher prevalence of moderate-to-severe NSD among CRS cases when compared to healthy controls. However, this association was not observed in Cho et al 36 and Greguric et al, 38 although a similar study design was implemented. In its first phase, Periyasamy et al 26 was the only study in this group that did not use imaging to confirm the diagnosis of CRS. Based on clinical manifestations alone, no marked differences were observed between the study and asymptomatic control groups.
Cho et al, 36 Elahi et al, 37 Greguric et al, 38 and Nikkerdar et al 40 also documented the mean NSA between the study and control groups. In the first three, no considerable differences were observed. Conversely, Nikkerdar et al 40 revealed a slight, but significant association. Harar et al 42 adopted a similar study design, but instead stratified findings based on the direction of NSD. No significant difference was reported between groups on either side of the nasal septum.
In a large-scale study by Kim et al, 50 subjects with NSD were compared to those without the condition, however, precise diagnostic criteria were not defined. CRS was then confirmed by means of clinical manifestations and imaging/endoscopy findings. Those with NSD had a significantly higher prevalence of CRS when compared to controls. Utilizing the same study design, Lee et al 48 observed no significant difference between groups.
Bias assessment
The risk of bias was assessed for each study in Table 8. Of the 34 studies, 12 (35.3%) were judged to be low risk of bias.21,28,29,34 -38,40,41,44,45
Risk of Bias Assessment.


Domain 1: Risk of bias due to confounding; Domain 2: Risk of bias due to measurement of the exposure; Domain 3: Risk of bias due to selection of participants; Domain 4: Risk of bias due to post-exposure interventions; Domain 5: Risk of bias due to missing data; Domain 6: Risk of bias due to measurement of the outcome; Domain 7: Risk of bias due to selection of the reported result.

Among the studies that reported NSD as their primary outcome, 12 out of 26 (46.2%) were considered low risk of bias. Three studies did not confirm the diagnosis of RS using imaging or endoscopy. In 5 studies, both the study and comparison groups were referred for RS symptoms, while in 2 studies, patients were referred for unrelated reasons. Additionally, 9 studies failed to provide a clear definition of NSD, 2 had missing data, and 7 did not report information regarding statistical analyses.
In contrast, none of the 8 (0%) studies that reported RS as their primary outcome were considered low risk of bias. Seven of these studies did not provide a clear definition of NSD, and in 4 studies, both the study and control groups were referred for RS symptoms. Three studies failed to define RS clearly, and one did not report statistical analyses. Very few studies corrected for confounding variables, and in those that did, only age was considered.
Among the low risk of bias studies, researchers evaluated 17 individual outcome measures. Of these, only 5 (29.4%) demonstrated a correlation between NSD and RS.
Outcomes and outcome measures are summarized in Figures 2 and 3.

Relationship between NSD and RS by outcome measure: association versus no association. NSA, nasal septal angle; NSD, nasal septal deviation; RS, rhinosinusitis.

Relationship between NSD and RS by sub-analysis: association versus no association. CRS, chronic rhinosinusitis; NSA, nasal septal angle; NSD, nasal septal deviation; RS, rhinosinusitis.
Discussion
Challenges in the Current Evidence Base and Future Directives
The current body of evidence on the relationship between NSD and RS is inconsistent, largely due to high risk of bias, variability in study design, and suboptimal methodology. Many of the studies included in our review exhibited a relatively high degree of bias due to the lack of standardized definitions for NSD and the inconsistent application of recognized criteria for diagnosing RS, such as the EPOS guidelines. 3 Additionally, almost none of the studies accounted for potential confounders, moderators, or mediators despite the multiple possible etiologies of RS and various risk factors such as smoking. 54 Furthermore, many of the included studies did not report a measure of statistical significance, complicating the synthesis of their results and the ability to draw firm conclusions. To address these limitations, we propose a standardized reporting framework to guide future research, which is presented in Table 9.
Recommended Framework for Reporting and Analyzing the Relationship Between NSD and RS.

Abbreviations: AIFR, acute invasive fungal rhinosinusitis; ARS, acute rhinosinusitis; CRS, chronic rhinosinusitis; CT, computed tomography; EPOS, European Position Paper on Rhinosinusitis and Nasal Polyps; MSFB, maxillary sinus fungal ball; NSA, nasal septal angle; NSD, nasal septal deviation; RARS, recurrent acute rhinosinusitis; RS, rhinosinusitis.
A classification system for NSD type/shape is proposed by Mladina et al. 55
RS diagnosis criteria are provided in the EPOS guidelines, published by Fokkens et al. 3
A classification system for NSD severity is proposed by Periyasamy et al. 26
Mixed Findings in High-Quality Studies
Despite these challenges, among the studies categorized as low risk of bias, 5/17 (29.4%) individual outcome measures suggested an association between NSD and RS. Taneja et al 35 demonstrated that subjects with maxillary sinusitis had a considerably higher prevalence of NSD >5° when compared to healthy control subjects, although no statistical significance was provided. Nonetheless, they also demonstrated that study subjects had a significantly greater mean NSA. This finding was also documented in Nikkerdar et al, 40 in which individuals diagnosed with CRS had a significantly greater mean NSA than healthy control subjects. The authors reinforced these results by demonstrating that those with CRS had a significantly higher prevalence of moderate (10-15°) and severe (>15°) NSD. Elahi et al 37 reported a similar trend, but no statistical analysis was conducted.
Although several high quality studies suggest a possible association, the evidence remains inconclusive. This mirrors the findings of a review by Collet et al, 14 in which they did not find sufficient evidence to establish a robust relationship.
NSD Severity as a Potential Contributor to RS
Conversely, a systematic analysis by Orlandi 13 found a statistically significant association between NSD and RS, particularly in patients with a NSA of ≥10°. Among our included studies, 10 evaluated NSAs exceeding this threshold. Only 4/11 (36.4%) individual outcome measures supported such an association, with one study finding it only in subjects with an NSA >20°. This suggests that an association with RS may only exist in more severe cases of NSD. However, the limited number of studies assessing higher degrees of NSD restricts the strength of this conclusion and highlights the need for further research to clarify whether severity truly modulates the relationship with RS. Orlandi’s analysis 13 represents an important contribution to the field. However, further clarification regarding potential sources of bias, the chosen methodology, and the rationale behind the exclusion of certain articles could provide additional insights and enhance the robustness of their findings.
Strengths and Limitations
A significant limitation of our study was the inability to access full-text articles for several foundational studies, such as Elahi et al, 56 Yousem et al, 57 and Hamdan et al.58,59 Additionally, only studies published in English and French were included. This limited our ability to perform a complete analysis and may have impacted the robustness of our findings. Furthermore, data regarding the specific morphological patterns of NSD were not extracted, nor was information on whether RS occurred ipsilaterally, contralaterally, or bilaterally in relation to the affected side of the nasal cavity. This may be important, as the study by Moorthy et al, 60 which employed the Mladina classification system to assess septal shapes, 55 and the study by Gencer et al, 61 which examined the affected sides of RS, identified significant independent associations. Future research should explore these factors to offer a more comprehensive understanding, as proposed in our standardized reporting framework.
To our knowledge, this is the most comprehensive review of the association between NSD and RS conducted to date. Our systematic review's strengths include a thorough search strategy, rigorous methodology, and the inclusion of a diverse range of studies, allowing us to capture a broad spectrum of data on the association between NSD and RS. Furthermore, only studies with a control group were included to mitigate the risk of confounding variables. Finally, we conducted sub-analyses alongside the use of critical appraisal tools to assess study quality, which enhanced the reliability of our findings.
Conclusion
Overall, the current body of evidence demonstrates an unclear relationship between NSD and RS. While some studies suggest a potential association, the lack of standardization and comprehensive reporting hinders the ability to draw definitive conclusions. This is attributable to heterogeneity in definitions, diagnostic criteria, and outcome measures, as well as insufficient control for bias. To ensure consistency across studies and enable more reliable comparisons, we propose a standardized reporting framework for future research. Such efforts may enhance clinical understanding and guide the development of more effective preventative treatment strategies.
Supplemental Material
sj-docx-1-ohn-10.1177_19160216251390316 – Supplemental material for The Relationship Between Nasal Septal Deviation and Rhinosinusitis: A Systematic Review
Supplemental material, sj-docx-1-ohn-10.1177_19160216251390316 for The Relationship Between Nasal Septal Deviation and Rhinosinusitis: A Systematic Review by Aidan Shulkin, Alexandra Katz and Marc A. Tewfik in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Acknowledgements
The authors would like to thank the librarian Amy Bergeron for validating our methodology and aiding in the development of our search terms.
Author Contributions
A.S. and A.K. contributed equally to this project and shared responsibility for the integrity of the data and the accuracy of the data analysis. A.S.: Conceptualization, methodology, protocol—original draft, protocol—review and editing, formal analysis, visualization, writing—original draft, writing—review and editing. A.K.: Conceptualization, methodology, project administration, protocol—original draft, protocol—review and editing, formal analysis, visualization, writing—original draft, writing—review and editing. M.A.T.: Conceptualization, protocol—review and editing, writing—review and editing, supervision.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.