
Abstract
Importance
Intraoperative narrow-band imaging (NBI) has been used to improve superficial (mucosal) resection margin clearance in oral squamous cell carcinoma (OSCC). However, no study has been conducted in a randomized controlled trial comparing OSCC resection using NBI and standard white light (WL).
Objective
To compare the rate of pathological margin clearance between NBI-guided and WL-guided resection in OSCC patients.
Design
Parallel-design, single-center, randomized controlled trial.
Setting
Tertiary care center, Department of Otolaryngology.
Participants
One hundred and four OSCC patients undergoing surgical resection were included in the study.
Intervention
Patients were randomly assigned to have either NBI-guided (n = 52) or WL-guided (n = 52) resection.
Main Outcome Measures
Final pathological margin status and clinical outcomes, including type of defect reconstruction and functional outcomes (persisting tracheostomy and tube feeding), were compared between the 2 groups.
Results
A significantly higher rate of clear superficial margin was achieved in patients in the NBI group than in the WL group (96.2% and 80.8%, respectively, P = .014). The locoregional or free flap reconstruction rates between the 2 groups were indistinguishable. Oral tongue and floor of the mouth primaries were detected more frequently in the NBI group, which may affect the postoperative deglutition function, leading to insignificantly higher rates of persistent tracheostomy and feeding tube (11.5% vs 5.8%, P = .488, and 19.2% vs 13.5%, P = .597, respectively).
Conclusions and Relevance
The study demonstrated that intraoperative NBI-guided resection in OSCC resulted in a more precise definition of superficial tumor margin than the standard WL-guided resection. In addition, the reconstruction method and functional outcomes were comparable between the 2 groups.

Introduction
Oral cavity cancer is the most common head and neck cancer, with an incidence of 377,713 new cases and 177,757 new deaths reported globally. 1 The predominant malignant cell type of this cancer is oral squamous cell carcinoma (OSCC), accounting for more than 90% of cases.2,3 Surgery with adequate margins is the mainstay of treatment in both early and locally advanced stages of disease. Local recurrence rates of 11% to 44% have been reported after surgical resection under conventional white light (WL) inspection and palpation, recurrence being related to either microscopic residual disease from incomplete tumor resection or field cancerization.2,3 According to a systematic review, to achieve the completeness of resection, intraoperative margin assessment, including pathological techniques (frozen section, Mohs surgery, and molecular analysis), wide-field analysis (fluorescent dyes, non-fluorescent dyes, autofluorescent imaging, and narrow-band imaging), and narrow-field analysis (spectroscopy and optical coherence tomography) have been developed. However, each technique has its strengths and limitations. 4
Narrow-band imaging (NBI) is an endoscopic video imaging technique with specific light source bands of 400 to 430 nm (center at 415 nm) and 525 to 555 nm (center at 540 nm) to target hemoglobin as an endogenous chromophore. 4 Blue light absorbed by hemoglobin emphasizes the contrast of the capillary bed and intrapapillary capillary loop (IPCL) pattern in the superficial mucosa by making them appear brown. Meanwhile, thicker blood vessels in the deep mucosa and submucosa are enhanced by green light and appear cyan. 5 These filtered wavelengths intensify the microvascular abnormalities associated with the premalignant and malignant changes in the mucosal lining of the upper aerodigestive tract.6,7 Therefore, visualization of IPCL alterations surrounding lesions helps establish the surgical margin. 8
Previous studies demonstrated that NBI-guided resection reduced the rate of positive superficial margins compared with historical data using conventional WL in oral and oropharyngeal cancers.6,9 In contrast, a prospective cohort study showed that NBI was not superior to WL in delineating oral mucosal tumor borders. 10 However, no randomized controlled trials comparing surgical resection with and without NBI have been performed.
The main aim of this study is to compare the pathological superficial (mucosal) margin clearance rate between narrow-band imaging-guided resection and standard white light-guided resection in OSCC. The secondary objective is to investigate the type of defect reconstruction and functional outcomes, including the rates of persisting tracheostomy and tube feeding.
Materials and Methods
Study Design
This prospective randomized controlled trial complied with the guidelines for Good Clinical Practice and the Declaration of Helsinki and was approved by the Ethics Committee of the Faculty of Medicine, Chiang Mai University. The reference identification number is ENT-2564-08564. The study has been reported by the Consolidated Standards of Reporting Trials (CONSORT) Guidelines. 11
Participants
Patients were recruited at the Department of Otolaryngology between June 2022 and February 2024. A multidisciplinary team discussed patients’ treatment. All patients who agreed to participate in the study signed an informed consent form before enrollment. The inclusion criteria were OSCC patients aged more than 18 years with Eastern Cooperative Oncology Group performance status 0 to 1 who were due to undergo surgical treatment. Patients were excluded from the study if they had undergone previous head and neck surgery or irradiation, had extensive lesions resulting in the inability to define mucosal resection margins around the tumor (for example, a bulky or exophytic oral tongue lesion precluding an endoscopic view of the posterior tumor border), had distant metastatic disease, or had cancer in other parts of the body.
Sample Size
The sample size was calculated with the program statulator.com, using the results of a previous study where the percentage of negative superficial resection margins from NBI-guided resection was 88%, while from WL examination and palpation in our historical data was 65% which is also aligned with that of the previous study (64%). 6 To detect an increased negative margin rate to 23% incorporating the effect of NBI-guided resection and assuming an alpha level of 5% with a power of 80%, 51 participants were required in each group. With an expected approximate dropout rate of 5%, we planned to recruit 108 participants (54 per group).
Randomization
Participants were randomly assigned into 2 groups using computer-generated random numbers (www.sealedenvelope.com) with a block size of 4 and an equal assignment probability to receive either WL or NBI-guided resection.
Blinding
The participants, the investigator who randomized them, and the pathologist were blinded to the intervention.
Interventions
White light group
After general anesthesia and surgical field preparation, and before any surgical action involving bleeding, the resection margins were outlined by a single surgeon with a fine-tip electric cautery and using a ruler to help maintain a distance of 1.5 cm from the gross tumor boundaries defined visually under surgical lights and headlamps for ulcerative, exophytic, leukoplakia, and erythroplakia lesions and by palpation for endophytic lesion.
NBI-guided group
Under WL visualization and palpation, a 1.5 cm distance of normal appearing mucosa from gross tumor margins was carefully outlined with a fine-tip electric cautery. Meticulous hemostasis was maintained, as blood staining alters light penetration and impairs NBI evaluation. The NBI, Visera Elite OTV-S190 video processor and CLV-S190 light source, CH-S190-XZ HDTV camera, and OEV261H 26" LCD HD monitor (Olympus Medical Systems Corp, Tokyo, Japan) with a flexible endoscope were used to redefine the margins. A charge-coupled device captures the 2 specific wavelength lights at the tip of the videoendoscope, and the image is then reconstructed, displaying the mucosal vessels in brown and submucosal vessels in cyan, increasing the contrast between vasculature and surrounding mucosa. The scope tip was placed at a distance of approximately 20 mm from the lesion to evaluate the tumor border, then at a distance of 3 to 5 mm for close observation of the mucosal surface around the tumor border. IPCL alterations, including pattern dilation and crossing, pattern elongation and meandering, pattern destruction and angiogenesis, and brown dots, were considered NBI-positive, and a 1.5 cm distance margin from these abnormal findings was outlined. Then the lights were turned back on. The conventional surgical resection is based on visual inspection and palpation. Although NBI could provide a more precise definition of the superficial extension, it may miss the palpable submucosal or deep tumor. Therefore, in the case of different distances between the 2 outlines, the wider one was regarded as the resection margin to achieve the optimal tumor clearance (Figure 1).
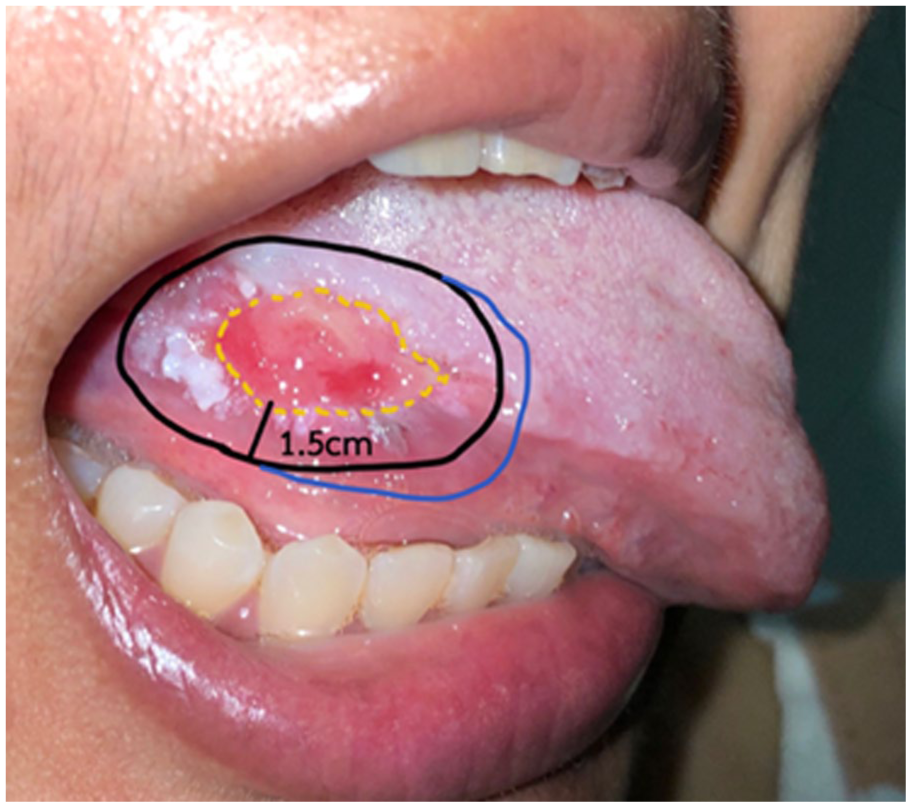
Outlined tumor.
Clinical Assessment
Preoperative evaluation with computed tomography or magnetic resonance imaging and clinical staging (cTNM) in accordance with the 8th AJCC TNM staging was obtained. Preoperative data collection included age, gender, history of smoking and alcohol drinking, primary tumor subsite, and clinical tumor staging.
A single surgeon defined resection margins for both groups. Following resection, the specimen was marked and orientated for pathological examination. Tumor margins were frozen-sectioned; if malignancy was detected, the resection was promptly expanded. A single pathologist reviewed and made the final decision on all resected specimens for final evaluation. Pathological margins were defined as “clear or sufficient” when >3 mm and “insufficient” when <3 mm distance between the resection edge and the border of neoplastic cells.2,3 Definitive pathology and margin status were collected for both superficial (mucosal) and deep (soft tissue) margins. However, the superficial margin was the primary outcome to evaluate the impact of NBI on the rate of margin clearance in comparison to the conventional WL method. Other collected data included other pathological results, the type of defect reconstruction, and functional outcomes (persisting tracheostomy and tube feeding at 6 months after surgery).
Statistical Analysis
Statistical analysis was performed by using STATA 16.0(STATACorp LLC., TX, USA) statistical software package. Categorical variables were presented as frequencies. Continuous variables were presented as mean + standard deviation if normally distributed or as median (interquartile range) if not. Pearson’s chi-squared or Fisher’s exact tests were used to compare categorical variables with frequencies larger than 5 or smaller than 5, respectively. A student’s t-test was employed to compare continuous variables that were normally distributed, and a Mann-Whitney U test was used to compare continuous variables with a nonnormal distribution. A linear or logistic regression model was outlined using a stepwise forward method to test the significant variables using univariate and multivariate analysis. The risk measure was the mean difference or odds ratio (OR) and 95% CI. A P-value less than .05 was considered statistically significant for all statistical analyses.
Results
One hundred and nineteen patients were assessed for eligibility for inclusion in the study. Patient flow through the trial is summarized in the CONSORT diagram (Figure 2). Fifteen patients were excluded: 13 had previous head and neck surgery or radiation, and 2 had extensive lesions in which it was not possible to define the whole tumor surface margin. One hundred and four patients were eligible for inclusion and were randomized. All were included in the analysis. There were 52 patients in the NBI-guided group and 52 in the WL-guided group.

CONSORT.
Patients’ Baseline Characteristics
Patient and tumor characteristics between the 2 groups are shown in Table 1. There were no differences in baseline characteristics between the 2 groups (P > .05). The majority of the primary tumor sites in both groups were the tongue (55.8% in the NBI group and 40.4% in the WL group). The majority of cases were in the advanced stages (T3-T4) of primary cancer (86.6% in the NBI group and 94.2% in the WL group, without significant difference between the 2 groups, P = .122).
Baseline Characteristics of the Analyzed Patients.

Abbreviation: NBI, narrow-band imaging.
Pathological Outcomes
Regarding pathological results, clear superficial margins were achieved in 50 patients (96.2%) in the NBI group and 42 (80.8%) in the WL group. These results showed a statistically significant improvement in resection effectiveness using intraoperative NBI (P = .014). In addition, patients in the NBI group had slightly higher rates of clear deep and overall (combining superficial and deep margins) resection margins than those in the WL group (53.8% vs 46.2%, P = .278 and 53.8% vs 44.2%, P = .433, respectively) (Table 2).
Pathological and Clinical Outcomes of Patients in the NBI-Guided Resection Group and the WL-Guided Resection Group.

Abbreviations: NBI, narrow-band imaging; WL, white light.
Factors Predicting the Insufficient Deep Margin
Logistic regression analysis was used to evaluate possible factors affecting the insufficient deep margin, including primary site, T staging, tumor differentiation, lymphovascular invasion, perineural invasion, and depth of invasion (DOI). Only DOI >1 cm was associated with the risk of an insufficient pathological deep margin in the univariable analysis (OR: 2.63, 95% CI: 1.08-6.37, P = .033). In addition, when the multivariable analysis was applied, DOI was still the only significant risk factor for an increase in the rate of insufficient deep margin (OR: 2.51, 95% CI: 1.01-6.26, P = .048).
Factors Predicting the Insufficient Superficial Margin
Logistic regression analysis was used to evaluate possible factors affecting the insufficient superficial margin, including primary site, T staging, tumor differentiation, lymphovascular invasion, and perineural invasion. No factor affecting the insufficient superficial margin was demonstrated in univariable and multivariable analyses. In subgroup analysis, primary sites at the tongue and alveolar ridge compared with buccal mucosa were associated with the risks of an insufficient pathological superficial margin in the univariable analysis (OR: 14.0, 95% CI: 1.12-175.35, P = .041 and OR: 13.6, 95% CI: 1.48-124.59, P = .021, respectively) in the NBI group. However, when the multivariable analysis was applied, no significant risk factor was detected. On the other hand, no factors were associated with the risk of an insufficient pathological superficial margin in the univariable and multivariable analyses in the WL group.
Methods of Tissue Reconstruction and Functional Outcomes
Eleven patients (21.2%) undergoing NBI-guided resection were able to have primary closure of the defect following tumor resection. Locoregional flap reconstruction was required in 24 patients (46.2%), and microvascular free flap reconstruction was performed in 17 patients (32.7%). However, primary closure was achieved in 7 patients (13.5%) receiving WL-guided resection following tumor excision. Seventeen patients (32.7%) in this group required locoregional flap reconstruction, and 28 (53.8%) necessitated microvascular free flap reconstruction. Notably, there were no differences in the frequency of the type of reconstruction between the 2 groups (P = .098) (Table 2).
Regarding functional outcomes at 6 months after the surgery, patients in the NBI group had slightly higher rates of persisting tracheostomy and feeding tube without statistical significance (11.5% vs 5.8%, P = .488, and 19.2% vs 13.5%, P = .597, respectively) (Table 2).
Discussion
The present study revealed that resection of OSCC guided by NBI resulted in a significantly higher rate of clear superficial margins (96.2%) than resection with conventional WL guidance (80.8%). In addition, the results are better compared with those of previous studies, which reported a negative superficial margin of 80.3% to 88.5% in the NBI group and 64.6% in the WL group.6,9 These discordant rates may be because we strictly followed the 1.5 cm gross resection margins around the tumor.
The deep margin clearance rate was comparable between the 2 groups (53.8% in the NBI group and 46.2% in the WL group, P = .287). It is noteworthy that NBI has a limited tissue penetration of 240 μm, enhancing visualization of the new abnormal blood vessels in the mucosa. Therefore, it is appropriate for mucosal margin delineation but fails to detect submucosal extension and deep margin assessment. 12 Although the overall margin clearance rate in the NBI group was higher than that in the WL group (53.8% and 44.2%), no statistical difference was detected. These rates are lower than the previous report of 73.1% in the NBI group and 56.8% in the WL group. 6 This is explained by the higher number of T3 to T4 tumors with the possibility of deeper tumor invasion in our study (86.6% in the NBI group and 94.2% in the WL group) in comparison with those of the previous study (50% and 22.8%, respectively). 6 In addition, the present study demonstrated that DOI >1 cm was the only factor affecting an insufficiently deep pathological margin in the multivariable analysis. Therefore, we recommend a wider deep-margin resection in tumors with a DOI >1 cm.
In the NBI group, the oral tongue and alveolar ridge primaries were associated with the risk of an insufficient pathological superficial margin in the univariable regression analysis but not in the multivariable analysis. These results could be because the IPCL may not be well visualized in areas with thick mucosa, such as these primary sites. Therefore, careful delineation of the tumor borders should be considered in these anatomical areas.
NBI-guided resection may result in additional margins due to molecular-level abnormality that has not yet appeared in histopathology. 12 However, the present study showed that the locoregional and microvascular free flap reconstruction rates in the NBI group (78.9%) and the WL group (86.5%) were indistinguishable. Therefore, NBI-guided resection leads to a more precise definition of the superficial tumor margin without affecting the reconstruction method. Although persistent tracheostomy and feeding tube were slightly higher in the NBI group, the differences did not reach statistical significance. This could be explained by the finding that there were more patients with oral tongue (55.8%) and floor of mouth (21.2%) primaries in the NBI group compared with the WL group (40.4% and 15.4%, respectively),and surgical resection of these primary sites commonly affects deglutition function, requiring feeding tube and tracheostomy for airway protection.
Other optical imaging techniques have been studied in the last decade to improve intraoperative resection margin control in OSCC.12-16 A multicenter randomized clinical trial used intraoperative fluorescence visualization (FV) compared with WL to define resection margins. The study showed no significant differences in positive overall margin between the 2 groups (30% in the FV group and 30.1% in the WL group), both of which are lower than our study (46.2% in the NBI group and 55.8% in the WL group). Notably, only patients with high-grade lesions (severe dysplasia or carcinoma in situ) and T1 to T2 carcinomas were included in the study. 16 De Wit et al conducted a study comparing fluorescence molecular imaging (FMI) using cetuximab-800CW as a tracer and NBI to assess the mucosal tumor margins in 16 OSCC patients. The results showed that FMI was more accurate in defining mucosal and deep margins than NBI. 12 However, NBI is less expensive and does not require the administration of tracers. In addition, with a limited number of patients, further studies comparing these 2 techniques are required.
Although this is the first prospective randomized controlled study comparing the effect of NBI-guided and WL-guided resection on achieving clear surgical margins in OSCC, there are some limitations. First, NBI helps detect abnormal mucosal microvascular organization, improving mucosal resection margin clearance. It is ineffective in defining submucosal and deep resection margins. Therefore, the extent of deep-margin resection should be carefully evaluated with direct vision and palpation, particularly in advanced T-staged tumors. Second, the morphological change of the IPCL may not be well visualized in an area with thick mucosa, such as the tongue dorsum and alveolar ridge, or in a keratotic lesion, such as leukoplakia. Accurate delineation of the tumor borders requires a well-trained and experienced surgeon. Third, extensive lesions in which it was not possible to define the whole tumor surface margin may not be beneficial for using NBI. Furthermore, survival outcome analysis, which is crucial for assessing the effectiveness of the surgery and patient prognosis, was not performed because of the inadequate follow-up time. Therefore, studies into the use of a wider deep-margin resection, particularly in tumors with DOI >1 cm, and a multicenter study with an extended follow-up time are warranted.
Conclusion
This prospective randomized controlled study demonstrated that intraoperative NBI-guided resection in OSCC resulted in a secure superficial resection margin in a higher proportion of patients than the standard WL-guided resection. In addition, the extent of resection, determined by the type of reconstruction, and the rates of persistent tracheostomy and feeding tube were comparable between the 2 groups. Due to the limitation of NBI in the deep margin assessment, a comprehensive evaluation to delineate deep margin resection, particularly in tumors with DOI >1 cm, should be considered.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
P.S.: conceptualization, methodology, investigation, formal analysis, and writing—original draft. T.B.: conceptualization, formal analysis, writing—review, and editing. D.R.: conceptualization, investigation, writing—review, and editing. S.C.: investigation, writing—review, and editing. T.A.: investigation and data curation. W.W.: investigation and data curation. H.K.: conceptualization, methodology, investigation, formal analysis, writing—review, and editing.
Ethical Approval
The study protocol was approved by the Ethics Committee of the Faculty of Medicine, Chiang Mai University. The reference identification number is ENT-2564-08564.
Consent to Participate
All patients who agreed to participate in the study signed an informed consent form before enrollment.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Trial Registration
Thai Clinical Trial Registry: TCTR 20240427008.