
Abstract
Importance
Perioperative efficiency is an increasingly important consideration in head and neck surgery, yet comparative evaluations of surgical techniques for benign parotid tumors remain limited.
Objective
To evaluate the perioperative efficiency of extracapsular dissection (ECD) compared to superficial parotidectomy (SP) for benign parotid tumors.
Design
Systematic review and meta-analysis following Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Setting
Studies retrieved from PubMed, Embase, and the Cochrane Library.
Participants
Patients with benign parotid tumors who underwent either ECD or SP. Fifteen studies encompassing 2399 patients were included.
Interventions
ECD and SP as primary surgical techniques for the removal of benign parotid tumors.
Main Outcome Measures
Parameters related to perioperative efficiency were defined in this study as operative time, anesthesia time, duration of drain placement, length of hospital stay (LOS), and medical costs. Tumor size was also included as a comparative parameter.
Results
ECD was associated with significantly shorter operative time [mean difference (MD), −48.95 minutes; 95% confidence interval (CI), −66.40 to −31.50], anesthesia time (MD, −73.17 minutes; 95% CI, −81.61 to −64.73), drain placement duration (MD, −2.10 days; 95% CI, −3.82 to −0.38), and LOS (MD, −0.91 days; 95% CI, −1.34 to −0.48) compared to SP. Tumor size did not significantly differ between groups (MD, −0.14 cm; 95% CI, −0.33 to 0.05).
Conclusions
ECD demonstrates superior perioperative efficiency compared to SP.
Relevance
These findings support the use of ECD as a more efficient surgical option for benign parotid tumors in appropriately selected patients.

Highlights
This systematic review and meta-analysis compared extracapsular dissection (ECD) and superficial parotidectomy (SP) for benign parotid tumors, focusing on perioperative efficiency, an area that has been relatively understudied.
The findings showed that ECD was associated with significantly shorter operative time, anesthesia time, drain placement duration, and length of hospital stay compared to SP, while tumor size was comparable between the 2 procedures.
ECD appears to offer better perioperative efficiency than SP and may be a suitable surgical option for appropriately selected patients.
Introduction
Among parotid gland tumors, ~70% to 80% are benign, with pleomorphic adenoma and Warthin’s tumor being the most prevalent. Surgical excision remains the primary treatment for these benign tumors.1 -3 Studies on advances in parotidectomy have been consistently published, reflecting its significance in medical practice and relevance to clinicians.4 -6 Superficial parotidectomy (SP) has been one of the standard surgical approaches for these benign tumors, ensuring complete tumor removal along with the superficial lobe of the parotid gland through facial nerve (FN) dissection. 7 While SP remains a standard approach, extracapsular dissection (ECD) has emerged as an alternative technique that removes the tumor with a thin layer of normal parotid tissue, avoiding routine FN identification and dissection.8 -10
Several published reviews have compared ECD and SP, primarily focusing on recurrence rates, complication rates, and functional outcomes.11 -14 However, efficiency-related parameters, such as operative time, anesthesia time, duration of drain placement, and length of hospital stay (LOS), have not been specifically discussed. While ECD appears to involve less tissue trauma and manipulation, only 1 review has examined differences in operative duration between the 2 procedures, relying on data from just 3 studies. 15 With more studies on these efficiency parameters being published in recent years, our study aims to fill this knowledge gap by systematically reviewing the literature and conducting a meta-analysis comparing ECD and SP with respect to perioperative efficiency.
Materials and Methods
Literature Search
This systematic review and meta-analysis were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 16 Two independent researchers systematically searched PubMed, Embase, and the Cochrane Library for relevant studies published up to February 15, 2025 (Y.-C.L. and T.-Y.T.). The search strategy included the keywords “extracapsular” and “superficial parotidectomy.” In addition, the reference lists of included articles were manually screened to identify other potentially relevant studies.
Study Selection
The selection of studies followed the Population, Intervention, Comparison, Outcome framework. Population: Patients who underwent parotid surgery for benign parotid tumors. Intervention: Use of ECD for tumor removal. Comparison: Use of SP for tumor removal. Outcomes: Parameters related to perioperative efficiency, defined in this study as operative time, anesthesia time, duration of drain placement, LOS, and medical costs. Tumor size was also included as a comparative parameter to evaluate baseline comparability.
Studies were considered eligible if they met the following criteria. They had to be original research articles with a prospective or retrospective study design, published in English, and involving patients who underwent parotidectomy for benign parotid tumors. In addition, studies were required to provide a direct comparison between ECD and SP, reporting at least one of the following perioperative parameters: operative time, anesthesia duration, drain placement duration, LOS, or medical costs. Studies were excluded if they involved malignant parotid tumors, utilized endoscope-assisted or robot-assisted surgery, or examined surgical techniques incorporating fibrin sealants, flap reconstruction, or fascia grafting after parotidectomy. Articles that did not include both ECD and SP for direct comparison were also excluded. Furthermore, review articles, letters to the editor, case reports, and cadaveric studies were not considered for inclusion.
Data Extraction and Quality Assessment
Two independent researchers extracted data from the selected studies (Y.-C.L. and T.-Y.T.). The authors assessed the articles for bias using the Newcastle-Ottawa Scale for nonrandomized studies and the Cochrane Collaboration’s risk of bias tool (RoB 1.0) for randomized studies.16,17 Any discrepancies in study selection or data extraction were resolved through consensus discussions among the authors.
Outcomes
The primary outcomes were operative time (minutes), anesthesia time (minutes), duration of drain placement (days), LOS (days), and medical costs (United States dollars). Tumor size (centimeters) was included as a secondary parameter for comparison between groups.
Data Analysis
Statistical analyses were performed using Comprehensive Meta-Analysis software (version 3; Biostat, Englewood, NJ, USA). The mean difference (MD) was used for continuous variables. If necessary, missing means and standard deviations were estimated using validated statistical methods.18,19 A random-effects model was used in meta-analysis. Heterogeneity was evaluated using the I2 statistic, with values exceeding 50% indicating moderate heterogeneity and values above 75% suggesting high heterogeneity. 20 Egger’s intercept test and funnel plots were used to assess potential publication bias. 21 A P < .05 was considered statistically significant.
Results
Study Selection
The initial search identified a total of 240 studies. After removing 100 duplicate records, 140 articles remained for title and abstract screening. Of these, 37 studies were excluded based on relevance to the study criteria. The full text of the remaining 103 articles was reviewed in detail. Following this assessment, 88 studies were excluded for various reasons, including procedures not meeting the study criteria (12 studies), lack of relevant parameters (46 studies), classification as case reports, reviews, comments, or posters (23 studies), publication in a non-English language (4 studies), or failure to meet the specified inclusion criteria (3 studies). Ultimately, 15 studies met the inclusion criteria and were included in the final qualitative synthesis.22-36 A flowchart summarizing the study selection process is provided in Figure 1. The keywords used and the details of the literature search are provided in the Supplemental Material (see eTable 1).

Flow diagram of the literature search.
Characteristics of the Included Studies.
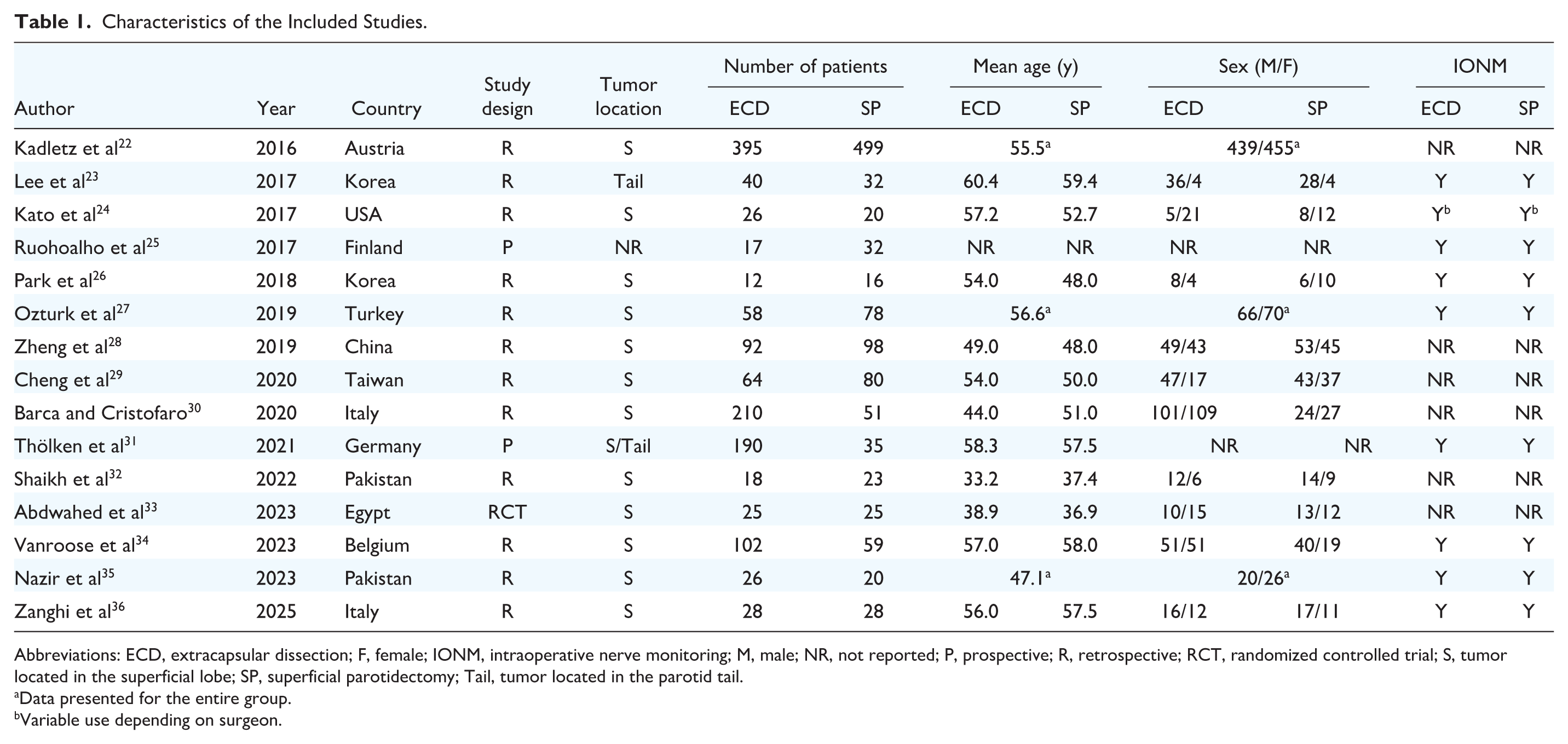
Abbreviations: ECD, extracapsular dissection; F, female; IONM, intraoperative nerve monitoring; M, male; NR, not reported; P, prospective; R, retrospective; RCT, randomized controlled trial; S, tumor located in the superficial lobe; SP, superficial parotidectomy; Tail, tumor located in the parotid tail.
Data presented for the entire group.
Variable use depending on surgeon.
Demographics
The included studies analyzed a total of 2399 patients undergoing parotidectomy. Patient characteristics, including age, sex, tumor location, and study design, are summarized in Table 1. The PRISMA checklist is provided in the Supplemental Material (see eTable 2), while the overall methodological quality of the studies is detailed in the Supplemental Material (see eTables 3 and 4).
Operative Time (Minutes)
Twelve studies reported data on operative time.22 -28,31 -35 A pooled analysis of the included studies demonstrated that operative time was significantly shorter in the ECD group compared to the SP group [MD, −48.95; 95% confidence interval (CI), −66.40 to −31.50; I2 = 99.17%; Figure 2]. Subgroup analyses were conducted based on total patient number (fewer than or more than 100), publication date (before or after 2020), study design (retrospective or prospective), and mean patient age (below or above 50 years). The P values for subgroup differences were 0.981 (patient number), 0.422 (publication date), 0.080 (study design), and 0.009 (mean age), respectively. These findings suggest that patient age may be a contributing factor to the observed heterogeneity, and the results of the subgroup analyses are provided in the Supplemental Material (see eTable 5).

Forest plot of operative time.
Anesthesia Time (Minutes)
Two studies provided data on anesthesia time.24,34 Meta-analysis of the included studies showed that anesthesia time was significantly lower in the ECD group than in the SP group (MD, −73.17; 95% CI, −81.61 to −64.73; I2 = 0.00%; Figure 3A).

Forest plot of outcomes. (A) Anesthesia time and (B) drain placement duration.
Drain Placement Duration (Days)
Two studies recorded data on the duration of drain placement.28,36 The pooled results of the included studies indicated that the duration of drain placement was shorter in the ECD group than in the SP group (MD, −2.10; 95% CI, −3.82 to −0.38; I2 = 97.66%; Figure 3B). We sought to explore potential sources of heterogeneity; however, given that only 2 studies reported related data, subgroup analysis could not be reliably performed.
Length of Hospital Stay (Days)
Six studies provided data on LOS.24,26,29,30,34,36 Analysis of the included studies revealed that patients in the ECD group had a significantly shorter LOS compared to those in the SP group (MD, −0.91; 95% CI, −1.34 to −0.48; I2 = 90.91%; Figure 4A). Subgroup analyses were conducted based on total patient number (fewer than or more than 100), publication date (before or after 2020), study design (retrospective or prospective). The P values for subgroup differences were .72 (total patient number), .41 (publication date), and 1.00 (study design), respectively, in the Supplemental Material (see eTable 6). Sensitivity analysis was performed by sequential omission of each study and revealed that heterogeneity decreased substantially (I2 = 0.00%) after excluding the study by Barca and Cristofaro, suggesting it may have contributed to the variability. 30
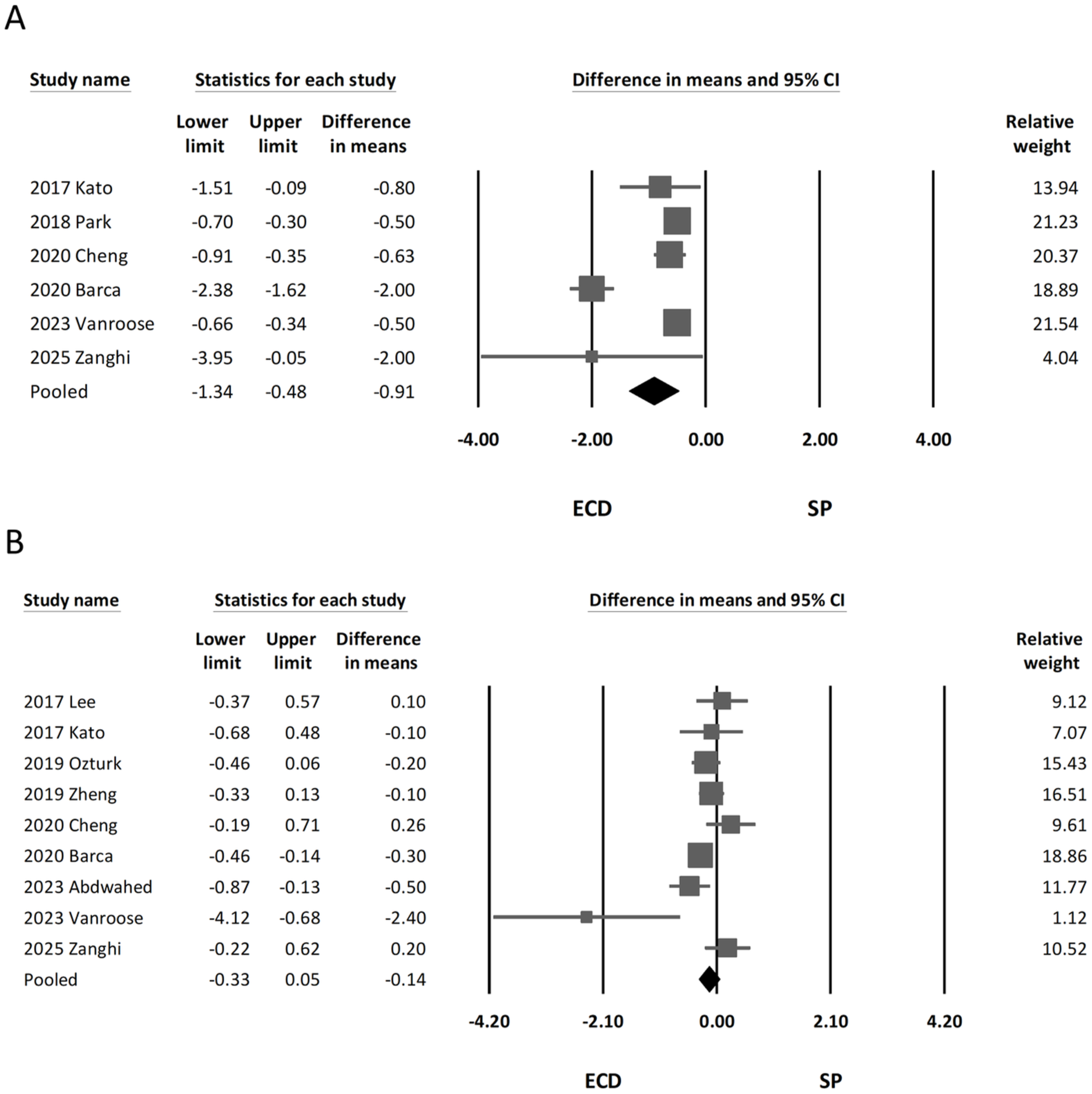
Forest plot of outcomes. (A) Length of hospital stay and (B) tumor size.
Overall Cost (United States Dollars)
Only one of the included studies reported the overall cost for both groups, finding that the ECD group had significantly lower mean costs than the SP group (24,118.23 and 35,835.88 United States dollars, respectively). 24 Due to the limited data, a meta-analysis of medical costs was not feasible, and this finding should be interpreted as preliminary.
Tumor Size (cm)
Nine of the included studies reported the size of parotid tumors.23,24,27-30,33,34,36 A pooled analysis indicated no significant difference between the 2 surgical procedures (MD, −0.14; 95% CI, −0.33 to 0.05; I2 = 60.43%; Figure 4B).
Publication Bias
The funnel plots along with the results of Egger’s test and the heterogeneity analysis are presented in the Supplemental Material (see eTable 7). The findings from Egger’s intercept test suggest no evident publication bias.
Discussion
The present study demonstrated that ECD is associated with significantly shorter operative time, anesthesia time, duration of drain placement, and LOS compared to SP. In contrast, tumor size was comparable between the 2 surgical groups. To our knowledge, this is the first research that systematically reviewed and analyzed the perioperative efficiency of ECD versus SP.
Several meta-analyses have been published comparing ECD and SP, the 2 commonly used surgical procedures for managing benign parotid tumors.11 -15 These studies primarily focus on oncologic and functional outcomes, such as recurrence rates, postoperative FN palsy, Frey syndrome, or other complications. Overall, ECD has been associated with lower rates of temporary FN injury and Frey syndrome, similar or lower rates of permanent FN injury, and comparable recurrence rates. While these factors are critical in determining surgical safety, perioperative efficiency, and economic impact have been relatively understudied. Only 1 review, published in 2019, systematically examined the operative time of ECD versus SP using 3 studies, but it did not conduct a meta-analysis. Additionally, 1 of the 3 studies in this review compared ECD with all other types of parotidectomy procedures rather than focusing on SP, which increased the heterogeneity of the analysis. 15 However, with an increasing number of studies addressing surgical efficiency and healthcare resource utilization, there is now a more substantial evidence base to evaluate these aspects comprehensively. By addressing this knowledge gap, our study provides important insight into the comparison of ECD and SP, enabling more informed decision-making that balances clinical effectiveness with procedural efficiency and supports thoughtful use of healthcare resources.37,38
Our results indicate that ECD requires significantly less operative time and anesthesia time compared to SP. The primary procedural difference between these 2 techniques lies in the need for formal FN dissection in SP, which likely accounts for the increased time requirement. Our subgroup analysis identified patient age as a potential contributor to the observed heterogeneity. This may be related to the association between tumor type and age. Warthin’s tumors, which are more common in older patients and typically located in the parotid tail, are generally more likely to be managed with ECD, potentially contributing to shorter operative times.39,40 In contrast, the time-saving advantage of ECD may be less consistent in younger patients, who more often present with tumor types requiring broader dissection. Several studies have reported that prolonged operative time is associated with an increased risk of postoperative complications, including temporary facial palsy and surgical site infection.25,41,42 In addition, prolonged general anesthesia has been linked to a higher risk of postoperative pulmonary complications, such as pneumonia.43,44 Therefore, selecting ECD for appropriately indicated cases may offer advantages in perioperative efficiency and contribute to improved patient safety by reducing operative and anesthesia-related risks.
The duration of postoperative drain placement and LOS are important factors related to patient recovery. Our findings demonstrate that patients undergoing ECD experience shorter durations of drain placement and reduced LOS compared to those undergoing SP. This difference is likely attributable to the less invasive nature of ECD, which minimizes tissue disruption and facilitates quicker recovery. In addition to reducing exposure to hospital-acquired risks, shorter hospital stays may also be associated with lower medical costs and more efficient use of healthcare resources. These advantages could be particularly meaningful in modern healthcare systems facing rising costs and constrained resources.45 -47
Selection bias has been a key concern in all studies comparing ECD and SP. One example of this is that some surgeons prefer to use ECD for smaller tumors while reserving SP for larger tumors, which could influence study outcomes. 48 In our study, with the exception of 1 article that did not specify the indications for ECD and SP, 25 all other studies clearly stated that both procedures were performed for tumors located in the tail region or superficial lobe of the parotid gland. This homogeneity in tumor location helps minimize potential bias in our results. Additionally, we conducted a meta-analysis on tumor size, which showed no significant difference between the ECD and SP groups. While it is difficult to control for all variables, these findings suggest that in evaluating perioperative efficiency parameters, ECD retains its advantages even when tumor size and location are similar between groups. Although these efforts helped improve the comparability of included studies, certain factors may still influence outcomes due to limitations in study design. For example, since ECD is conceptually intended to avoid direct FN dissection, surgeons may be more inclined to select ECD for tumors that are located more superficially or in the parotid tail, areas typically farther from the FN. These differences in surgical decision-making could contribute to variability in clinical outcomes, and therefore, the interpretation of our results should be approached with caution. However, several studies have also reported an increasing trend in the use of ECD in recent years compared to SP, suggesting growing recognition and acceptance of ECD among clinicians.34,49,50
The authors acknowledge several limitations of the current research. First, most studies included in this analysis are retrospective, which may introduce inherent biases. Second, for some parameters, only a limited number of studies provided sufficient data for analysis. Third, the lack of standardized surgical selection criteria across studies introduces potential selection bias. The independent relationship between tumor size and other parameters could not be further analyzed due to limitations in study design and available data. Furthermore, due to insufficient data, this study cannot directly confirm overall cost differences between ECD and SP. However, based on the observed differences in operative time, anesthesia time, drain placement duration, and LOS, which are closely related to healthcare resource use, it is reasonable to speculate that ECD may offer potential advantages in cost-effectiveness. Future studies with robust economic data are needed to directly evaluate the cost implications of these surgical approaches. Finally, the findings are most applicable to benign, superficially located parotid tumors managed in centers with specific expertise in ECD.
Conclusion
In conclusion, results from this meta-analysis suggest that ECD may offer certain procedural advantages over SP, including shorter operative and anesthesia times, reduced drain placement duration, and shorter LOS. However, the choice of surgical approach should also consider tumor characteristics, patient condition, and the surgeon’s clinical judgment, in addition to perioperative efficiency. These findings add to the growing body of evidence supporting ECD as a viable option for benign parotid tumors, emphasizing the importance of individualized surgical planning.
Supplemental Material
sj-docx-1-ohn-10.1177_19160216251385927 – Supplemental material for Extracapsular Dissection Versus Superficial Parotidectomy: A Systematic Review and Meta-Analysis of Perioperative Efficiency
Supplemental material, sj-docx-1-ohn-10.1177_19160216251385927 for Extracapsular Dissection Versus Superficial Parotidectomy: A Systematic Review and Meta-Analysis of Perioperative Efficiency by Yi-Chan Lee, Li-Jen Hsin, Yao-Te Tsai, Wan-Ni Lin, Tuan-Jen Fang, Shih-Chi Su, Cheng-Ming Luo, Rodney Cheng-En Hsieh and Tsung-You Tsai in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Acknowledgements
The authors would like to thank all colleagues who contributed to this study, as well as the anonymous reviewers and the editor for their valuable comments and suggestions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Not required for this study, as it is a meta-analysis of previously published data.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.