
Abstract
Importance
There are many methods for pediatric voice assessment, but each has its own limitations. Currently, there are few studies that have compared the outcomes of subjective and objective evaluation methods in children with voice disorders.
Objective
To apply and compare the pediatric Voice Handicap Index (pVHI) with acoustic analysis in pediatric benign voice disorders.
Design
Case-control study.
Setting
This study was conducted at a single institution.
Participants
Pediatric participants with and without benign voice disorders were included from August 2021 to April 2023.
Intervention or Exposures
The questionnaire results for the pVHI were obtained, and acoustic analysis was conducted.
Main Outcome Measures
The main outcomes included the pVHI scores, acoustic parameters, and the Pearson Correlation Coefficient.
Results
Out of the 338 participants, 160 children were diagnosed with voice disorders, whereas 178 did not exhibit such conditions. The total scores and those of each subscale were significantly higher in the patient group than in the control group (P < .05). Significant differences were also observed in the fundamental frequency (228.13 ± 66.78 vs 253.65 ± 47.21), jitter (2.08 ± 2.59 vs 2.42 ± 1.75), shimmer (8.52 ± 5.78 vs 9.44 ± 3.69), harmonic to noise ratio (HNR) (0.50 ± 0.68 vs 0.65 ± 0.19), s/z ratio (1.46 ± 1.89 vs 0.99 ± 0.44), and maximum phonation time (6.08 ± 3.38 vs 7.82 ± 2.50) (P < .05). When comparing the types of diseases, the physical dimension of the pVHI (17.43 ± 7.02 vs 15.29 ± 6.92 vs 13.32±7.71) and the HNR (0.39 ± 0.16 vs 0.41 ± 0.21 vs 0.75 ± 1.24) were most negatively affected in the vocal fold polyps group. Moderate to strong correlations were shown among the pVHI total and each subscale scores (P < .05), while the highest r score was shown between the physical and the total scores of the pVHI (r = 0.882).
Conclusions and Relevance
Pediatric patients with voice disorders exhibit more severe voice handicaps in both pVHI scores and acoustic parameters. The total score of the pVHI is moderately to strongly correlated with each subscale, whereas no strong correlation was presented between different acoustic parameters or between acoustic parameters and pVHI scores. This indicates that the two evaluation methods are not interchangeable; thus, a comprehensive evaluation is essential in clinical practice to prevent bias.

Key Message
This study introduces a primary framework aiming at enhancing diagnostic accuracy and improving treatment outcomes for pediatric voice disorders.
Combining subjective and objective assessment methods provides a more comprehensive evaluation of the impact of voice disorders on children.
Introduction
Voice disorders are common in the pediatric population and might have a significant impact on quality of life, as well as social and academic performance. 1 The incidence of voice disorders in children is estimated to be between 6% and 23% at some stages in their development. 2 The most common causes of pediatric dysphonia include vocal misuse, benign lesions, and infections, such as human papillomavirus, which can cause papillomatosis. 1 It has been demonstrated that children with dysphonia can sometimes be judged more negatively than can children without voice disorders. 3
There are many methods for pediatric voice assessment, but each has its own limitations.4,5 Several studies have demonstrated the use of subjective evaluation methods, such as perceptual rating scales, in children with voice disorders.6-9 However, these methods rely on the listener's perception of the child's voice quality and could be influenced by the rater's individual biases and lack of standardization. 10 Objective evaluation methods, such as acoustic analysis, have been used to evaluate children's voice disorders; 11 however, these methods require specialized equipment and sites and may not always be feasible in less developed medical institutions. By combining multiple methods, more accurate results can be obtained.
In the current study, we aimed to compare the results of subjective and objective evaluation methods in children with voice disorders. The pediatric Voice Handicap Index (pVHI), the most widely used subjective assessment scale in the pediatric population, has been demonstrated to reflect the impact of voice disorders on the quality of life of children with voice diseases. 12 Moreover, acoustic analysis can reflect the objective condition of the voice through the acoustic parameters of the voice. By analyzing and comparing the differences between the acoustic parameters of voice in individuals with and without voice disorders, objective indicators of the degree of hoarseness can be obtained, providing a theoretical basis for the application of voice acoustic testing in clinical voice assessment and therapeutic evaluation of vocal fold diseases. By applying the pVHI scale and acoustic analysis to each participant, we examined the differences in both approaches between children with and without voice disorders. Additionally, we attempted to explore the relationship between these two assessment methods using correlation analysis to explore better evaluation strategies, hoping to identify a more optimized approach to evaluating voice disorders in children that can improve diagnosis and treatment outcomes.
Methods
The current study was conducted at the West China Hospital of Sichuan University from August 2021 to April 2023. The study was approved by the Ethics Committee of Sichuan University (approval number: 2021-300), and participants were enrolled prospectively. Informed consent was obtained from the legal guardians of each participant prior to enrollment. The consent process involved providing each patient with detailed verbal and written explanations of the study’s purpose, procedures, risks, and benefits by trained research staff of our research team. Legal guardians of each participant were allowed sufficient time to ask questions before signing the consent form. This protocol was also reviewed and approved by our institutional ethics committee, ensuring compliance with ethical standards.
Participants
Pediatric participants aged 4 to 14 years were enrolled in this study, including 160 in the patient group and 178 in the control group. Each participant from the patient group was recruited from the outpatient department of the same hospital due to hoarseness and was confirmed to have voice disorders with observed presentation under video stroboscopy (Olympus Medical Systems Corp., Tokyo, Japan). The control group individuals were recruited from the outpatient department of the same hospital due to otitis media or ocular diseases, and each of them was confirmed to have no history of vocal complaints or any other long-lasting voice disorders. Video stroboscopy was also conducted to exclude individuals with voice disorders from the control group. Those who received voice therapy, experienced acute laryngitis for at least 3 months, or suffered from obstructive sleep apnea, common cold, or upper respiratory infection at the time of the investigation were excluded from the study. Video stroboscopy was conducted by the same laryngeal specialist, who was not involved in other processes of the study, to control bias.
Questionnaires and Self-assessment
All parents of the participants from the patient group were asked to provide their children’s information on several demographic characteristics, including gender, age, under the guidance of the same staff from our research group. Factors contributing to vocal strain and fatigue in children were also recorded, such as holding student leadership roles (which often require frequent or loud speaking to manage the class) and being over-scheduled with extracurricular activities (especially those involving singing, shouting, or prolonged speaking like choir, sports cheering, or debate club). Additionally, they were asked to complete the validated Chinese version of the pVHI scale, 12 which included 23 items and was classified into 3 subscales: (i) a functional subscale (7 items) investigating the parents’ perception of the impact of voice disorders on children’s communication and daily activities; (ii) a physical subscale (9 items) investigating the parents’ perception of the symptoms of their children's laryngeal discomfort; and (iii) an emotional subscale (7 items) investigating the parents' perception of children's affective responses to voice disorders. Each item was scored on a Likert scale ranging from 0 to 4. The maximum score was 92, and a higher score indicated that the parents perceived a more severe impact of the children's voice.
All the legal guardians of each pediatric participant completed the questionnaires online via Wenjuanxing, a platform powered by www.wjx.cn, which provides online technical support for questionnaire completion and data collection under the guidance of our research team members.
Acoustic Analysis
Acoustic recordings were collected in the same soundproof room with similar environmental noise levels below 45 dB. The speech signal was picked up by an electronic microphone from a LingWAVES SPL meter (ATMOS MedizinTechnik, Germany), which was mounted on a headset to ensure a constant, reproducible distance (30 cm) from the mouth, pointing toward the mouth at an angle of 45° from the voice source by the same examiner. For each participant, three 5-second recordings of the /i/ vowel were obtained and analyzed, and the middle and sustained 1-second segments were selected for acoustic analysis using LingWAVES, which can analyze and transform the voice. The acoustic parameters included vocal fundamental frequency (F0; Hz), mean percentage vocal jitter (%) and shimmer (%), and mean harmonics-to-noise ratio (HNR; dB). The maximum phonation time (MPT; second) represents the maximum time that a person can sustain a vowel sound, which is produced in one deep breath at a relatively comfortable pitch and loudness. The best result of 3 attempts was chosen at producing the sustained vowel /a/ for as long as possible. The maximum phonation time required to produce the sustained consonant /s/ or /z/ was examined and recorded as “s” and “z”. The s/z ratio was also calculated. Acoustic parameter analysis was conducted by a laryngology specialist with formal training in acoustic assessment and more than 5 years of experience in this domain.
Statistical Analysis
All the data were analyzed using IBM SPSS Statistics (version 21.0; IBM Corp., Armonk, NY, USA). Means and standard deviations (SDs) were calculated for continuous variables. The Kolmogorov–Smirnov one-sample test was used to test the normality of the distribution of the measurement data. Differences between subgroups were compared using the Chi-square, rank sum, Mann‒Whitney U and ANOVA tests. Correlations were calculated as Pearson correlations. Statistical significance was set at a 2-tailed P = .05.
Results
A total of 338 participants were included in this study (186 boys and 152 girls; male-to-female ratio = 1.22:1), including 160 participants with and 178 without voice disorders. No significant difference was observed in age or gender distribution between the 2 groups (P > .05) (Table 1). The patient group consisted of vocal fold polyps (n = 74), chronic laryngitis (n = 44) and vocal fold nodules (n = 42).
Demographic characteristics of the participants.

Abbreviation: SD, standard deviation.
The pVHI scores and acoustic parameters from the acoustic analysis of both groups are presented in Tables 2 and 3. The total score and each subscale score were significantly greater in the patient group than in the control group (P < .05), revealing a more severe voice handicap in individuals with voice disorders. The same trend was also observed for all the acoustic parameters in the current study, including F0, jitter, shimmer, HNR, s, z, s/z, and MPT (P < .05). In regard to the comparison among the types of diseases, significant differences were only present in the physical subscale of the pVHI and the HNR (P < .05) (Table 4).
Comparison of the pVHI Scores Between the Patient Group and the Control Group.
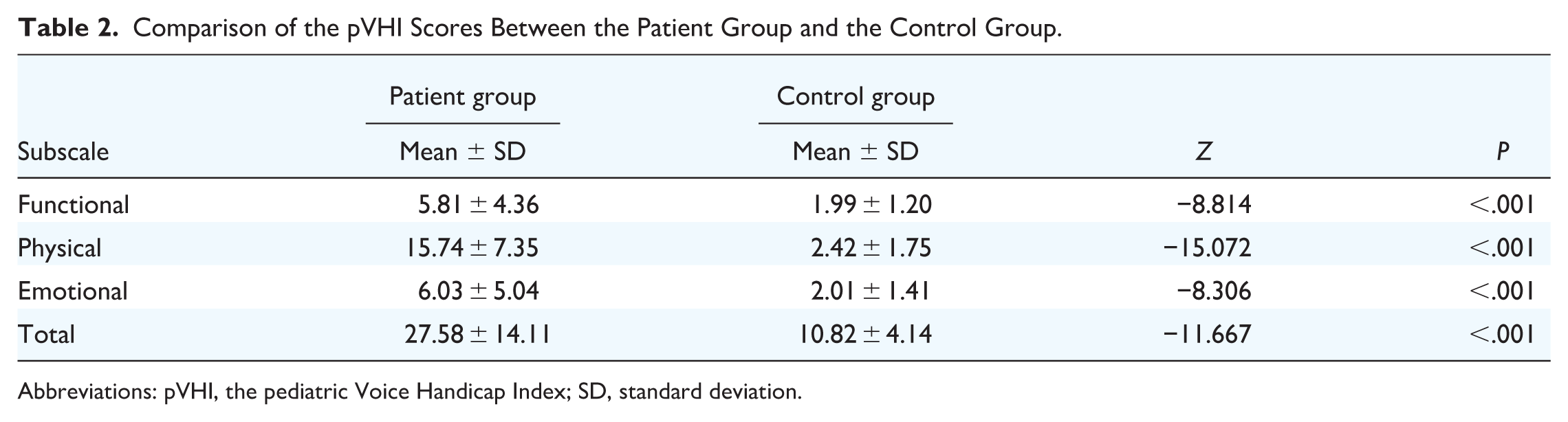
Abbreviations: pVHI, the pediatric Voice Handicap Index; SD, standard deviation.
Comparison of Acoustic Parameters Between the Patient Group and the Control Group.

Abbreviations: SD, standard deviation; F0, fundamental frequency; HNR, harmonic to noise ratio; MPT, maximum phonation time.
Comparison of the pVHI Scores and Acoustic Parameters Among Different Voice Disorders.

Abbreviations: pVHI, the pediatric Voice Handicap Index; SD, standard deviation; F0, fundamental frequency; HNR, harmonic to noise ratio; MPT, maximum phonation time.
The correlation analysis revealed a moderate to strong correlation between the pVHI total and each subscale scores core (P < .05). The highest r score was shown between the physical score and the total score of the pVHI. However, the acoustic parameters were not all significantly correlated with each other or with the pVHI scores (Table 5).
Coefficient (r value) of Correlation Between the pVHI Scores and Acoustic Parameters Scores.

Abbreviations: pVHI, the pediatric Voice Handicap Index; SD, standard deviation; F0, fundamental frequency; HNR, harmonic to noise ratio; MPT, maximum phonation time.
P < 0.05; **P < 0.01.
Discussion
Pediatric voice disorder patients are still a large group of patients who cannot be ignored by laryngologists. In a population-based, nationally representative household sample investigation, it was found that the annual prevalence of voice problems among children was estimated to be 14 per 1000.2 Pediatric dysphonia is very common, with prevalence rates up to 38% in the USA, while vocal fold nodules are the most common cause, accounting for 60% of pediatric dysphonia.13,14. Given the distinct anatomical, physiological, and psychological characteristics of children, it is inappropriate to directly and fully apply treatment approaches for adult voice disorders to the pediatric population. Therefore, it is crucial to have a correct understanding and assessment of pediatric voice disorders.
The assessment of voice disorders is of great importance during the diagnosis and treatment process. However, Holger et al. conducted and compared the Voice Handicap Index 12 (VHI-12) and the Göttingen Hoarseness Diagram (GHD) among adults. 15 There are already some reports on subjective assessment methods for pediatric voice disorders in the literature, yielding inconsistent or incomplete conclusions.10,16 In our previous studies, we translated and validated the pVHI questionnaire in the Chinese population, the results of which were consistent with our current study. 17 For the acoustic analysis results, the parameters we included were significantly different between the 2 groups, as expected. More specifically, children with voice disorders not only have poorer voice quality but also tend to have a faster speaking rate and greater difficulty sustaining phonation compared to the control population, which was reflected by the lower HNR and F0 and smaller MPT values. Moreover, the parameters of jitter and shimmer were significantly lower in the patient group, possibly indicating that children with voice disorders tend to have more stable voice abnormalities than do normal children with weak control of their vocal folds. The s/z ratio of the patient group deviated further from the normal range than that of the control group. This phenomenon possibly suggests that children with voice disorders are more likely to adapt to new ways of speaking continuously and erroneously to meet daily communication needs without consciousness. If persistent for a long time, it may lead to other voice disorders (eg, functional voice disorders). Therefore, the diagnosis and treatment of these patients are important and urgent. We also need to emphasize that the sound emitted by children may not necessarily represent the real situation when conducting objective evaluations, which might be more obvious for parameters such as pitch, tone, and MPT. When children come to unfamiliar environments without close contact with medical personnel, it may be timely and difficult for them to produce sound correctly according to medical requirements.
Furthermore, we compared the differences among disease spectra. Vocal fold nodules are typically the most common finding in pediatric voice disorders, whereas vocal fold polyps were the primary diagnosis in the current study. We believe this may be attributable to differences in disease distribution, as our hospital serves as a national referral center for complex voice disorders. Consequently, we receive a high proportion of patients from other regions who often present with longer disease duration and more severe conditions compared to the general population. It was also discovered children with vocal fold polyps exhibit more severe impairment across all dimensions of subjective voice assessment, though statistically significant differences were found only in the physical dimension according to the pVHI scale. We propose that this phenomenon may arise from the fact that these items are more readily detectable and observable by parents when compared to emotional and functional dimensions. Additionally, the results also appear associated with the level of vocal health awareness and attentiveness to observational details demonstrated by parents of children with voice disorders. In contrast, chronic laryngitis showed the mildest presentation (the s/z ratio confirmed that this group had the most severe voice hoarseness), the results of which were presented for all parameters except for the s/z ratio, although most of the differences were not significant. A possible explanation is that the pediatric group has insufficient control and understanding of vocal fold movement, which may prevent them from better coordinating with whether the vocal fold vibrates to produce s or z sounds. This provides guidance for us to properly understand the severity of different voice disorders in the child population.
For the correlative analysis, moderate to strong correlations were presented between the total and subscale scores of the pVHI, which is consistent with previous studies.18,19 Meanwhile, the correlation between the total and the physical subscale was the strongest, which is different from previous research and may be due to differences in sample selection of the population. 20 As found in the current literature, Narasimhan et al. conducted a correlation experiment between objective and perceptual parameters using the GRBAS rating scale and acoustic and cepstral parameters, showing that the perceptual ratings of grade, breathness, and roughness had better correlations with cepstral measures than with time-based acoustic parameters. 4 However, in the study of Soumya et al., the opposite results were obtained, as the perceptual parameters showed a weak and moderate correlation with the acoustic parameters of elderly speakers. 21 Few studies have compared the assessment tools in the pediatric population. As demonstrated in the current study among children, the correlation between the included acoustic parameters was not satisfactory. A moderate correlation between jitter and shimmer was presented, with the highest r value among all the relationships, as these 2 indicators are both related to vocal fold vibration abnormalities. The correlations between MPT and s or z were relatively satisfactory because they are related to aerodynamic indices. Previous studies on adult voice disorders have suggested that F0 is important for the diagnosis of voice disorders. However, the F0 value is greater in the pediatric population than in adults, and there is not much difference between the sexes during childhood. 22 As found in our study, the correlation between F0 and other parameters was not as good as expected. As reported by Bilal et al., the mean F0, HNR, and jitter were more affected by the width or length of the lesion.11,23 We speculate that this reflects the differences between children and adults.
Overall, the correlation between subjective and objective indicators was not as good as we expected. We speculate that this might be related to the extent of parents’ knowledge about voice disorders. Some parents might consider hoarseness to not be a major problem and therefore pay little attention to the negative impact of voice disorders on their children. Therefore, it is necessary to strengthen the promotion of voice disorders and vocal health knowledge. In addition to attaching importance to the voice-related quality of life filled out by parents, it is also necessary to attach importance to children's own understanding of voice-related quality of life. For example, subjective scales such as the Children's Voice Handicap Index (CVHI) 24 filled out by children themselves are still very important for assessing children's voice disorders; these scales are more convenient to use and require little attention. It can be used to preliminarily screen whether children have physiological, psychological, or functional negative impacts caused by voice symptoms. Based on the results, objective tests such as voice analysis can be conducted to more accurately analyze children's voice performance. A voice treatment plan can then be formulated by combining the pVHI and voice analysis results. For some medical institutions that do not have the conditions to perform acoustic analysis examinations, open-source software could be considered to provide auxiliary assistance, such as the PRAAT, a cost-free desktop program dedicated to those studying linguistics (https://praat.en.softonic.com/). Relying solely on subjective evaluation scales still has obvious limitations.
It is important to acknowledge several limitations of the present study. First, the use of the pVHI scale, which is completed by parents, may not accurately capture the child’s own subjective experience. Second, this study was conducted at a tertiary referral center, which predominantly manages more complex or severe cases of pediatric voice disorders; therefore, the findings may not be generalizable to children with milder conditions seen in primary care or community settings. Third, patients with higher vocal demands—such as those participating in choirs or debate clubs—were excluded from the study, although this group may represent an important subgroup with distinct characteristics not reflected in our analysis. Future research would benefit from including more diverse populations and incorporating assessment tools that directly capture the perspectives of pediatric patients
Conclusion
The pVHI scores and all the included acoustic parameters presented significant differences between the patient and control groups, indicating more severe voice handicap in the individuals in the patient group. Moderate to strong correlations were demonstrated between the total score and each dimension of the pVHI scale, while the correlations between the acoustic parameters and the acoustic parameters and subjective evaluation scales were not satisfactory. This study indicates that the 2 evaluation methods are not interchangeable, therefore comprehensive evaluation is necessary in clinical practice to avoid bias.
Footnotes
Authors contributions
Study design: Dan Lu. Data curation: Lingyu Yu, Jia Ren, Huan Lu, Bin Zeng. Formal analysis: Jia Ren, Tianpei Ma. Methodology: Dan Lu, Lingyu Yu, Tianpei Ma. Writing – original draft: Lingyu Yu. Writing – review and editing: Lingyu Yu, Jia Ren, Dan Lu, Zhongjing Pan, Qinghan Zeng, and Yuanyuan Peng. All the authors have read and approved the final manuscript.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
The study was approved by the Ethics Committee of Sichuan University, and written informed consent was obtained from the legal guardians of each participant.
Competing Interests
The authors declare that they have no competing interests.