
Abstract
Importance
Sudden sensorineural hearing loss (SSNHL) is associated with metabolic syndrome, central obesity, and albumin level. Malnutrition may adversely affect recovery in older patients with SSNHL, yet its clinical relevance remains underexplored.
Objective
This study investigated the associations of the geriatric nutritional risk index (GNRI) with clinical outcomes in older patients (age >65 years) with SSNHL.
Design
Observational retrospective study.
Setting
Tertiary academic medical center.
Participants
A total of 328 patients aged over 65 years who were diagnosed with SSNHL were retrospectively enrolled. Patients were included if they had complete clinical, audiometric, and laboratory data, including serum albumin levels and anthropometrics for GNRI calculation.
Intervention/Exposures
The primary exposure was the GNRI, calculated using body weight, height, and serum albumin. All patients received steroid treatment for SSNHL.
Main Outcome Measures
The primary outcome was hearing recovery, categorized as favorable or unfavorable based on clinical audiometric improvement.
Results
Among older patients with SSNHL, 107 (32.62%) and 221 (67.38%) had favorable and unfavorable outcomes, respectively. Vertigo, worse initial level of hearing loss, and low GNRI were mainly associated with unfavorable hearing outcomes in older patients with SSNHL. Furthermore, low GNRI (<99) was linked to unfavorable clinical outcomes (odds ratio [OR] = 1.91, P = .0151). Multivariate logistic regression revealed that vertigo (aOR = 3.45, P = .0002), worse initial level of hearing loss (per 1 unit increase in hearing loss elevates the risk of poor hearing recovery by 2%, P = .0015), and low GNRI (aOR = 1.79, P = .0435) were associated with unfavorable clinical outcomes.
Conclusion
In summary, evaluation of nutritional status plays a crucial role in improving clinical outcomes in SSNHL. Moreover, GNRI can predict clinical outcomes in older patients with SSNHL treated with steroids. Older patients with SSNHL who have vertigo, a worse initial level of hearing loss, and low GNRI exhibit unfavorable outcomes.
Relevance
GNRI is a simple, accessible marker that can help identify older SSNHL patients at higher risk of poor recovery. Future prospective studies should validate its use as a prognostic tool and explore whether nutritional interventions can improve hearing outcomes.

Key Message
Low geriatric nutritional risk index (GNRI; <99) is significantly associated with unfavorable clinical outcomes in older patients (age >65 years) with sudden sensorineural hearing loss (SSNHL).
Vertigo and worse initial hearing loss are independent predictors of poor hearing recovery in this population.
Nutritional status evaluation using GNRI may aid in risk stratification and management planning for older patients with SSNHL.
Introduction
Sudden sensorineural hearing loss (SSNHL) is defined as acute hearing loss of at least 30 dB at 3 continuous frequencies within 3 days. 1 The incidence of SSNHL has been reported to be 5 to 27 per 100,000 people in the United States and 8.33 per 100,000 people in Taiwan annually.1,2 The etiology of SSNHL remains unclear, but the etiology may involve viral infection, vascular disease, autoimmunity, and genetic factors. 3 Numerous prognostic factors influence recovery from SSNHL, including patient age, presence of vertigo, severity of initial hearing loss, configuration of the audiogram, and duration between hearing loss onset and treatment implementation. 1 Nevertheless, the factors leading to unfavorable outcomes in patients with SSNHL and the underlying mechanisms remain incompletely understood.
Metabolic syndrome is a group of common pathologies, including abdominal obesity, hypertension, insulin resistance, and dyslipidemia. A study revealed that metabolic syndrome is an independent risk factor for SSNHL in Taiwan. 4 Moreover, a study demonstrated that the rate of recovery from SSNHL was lower among patients with metabolic syndrome than among those without metabolic syndrome in Korea. 5 Wang et al revealed that normal weight central obesity is an unfavorable prognostic factor for SSNHL in Taiwan, and Lee et al indicated that increased body mass index (BMI) is significantly associated with the development of SSNHL and its unfavorable prognosis in Korea.6,7 Zheng et al demonstrated that lower serum albumin levels are an unfavorable prognostic factor for SSNHL in China. 8
The geriatric nutritional risk index (GNRI) is a simple and well-established nutritional assessment tool and is a significant prognostic factor in various cancers, including head and neck cancer.9 -11 Previous studies demonstrated that decreased GNRI was significantly correlated with unfavorable head and neck cancer overall survival.9 -11 GNRI is a novel nutritional scale consisting of 3 main objective parameters related to nutritional status, body weight (BW), height, and serum albumin level. Compared with albumin or BMI alone, GNRI is a more effective index indicating nutrition-related risk.11,12
In both acute and chronic diseases, albumin levels commonly decrease. This decrease in albumin levels not only provides crucial prognostic insights for a range of diseases but also serves as a biomarker of inflammation. 8 Despite steroid treatment, low recovery of hearing has been reported in older patients with idiopathic SSNHL.13 -16 A study revealed that after the age of 65 years, the likelihood of treatment success markedly decreases. 14 We wish to identify the prognostic factors for SSNHL in older patients. No study has evaluated the correlation between nutritional status and GNRI in older patients with SSNHL. Thus, this study evaluated GNRI in older patients with SSNHL and explored whether GNRI is associated with treatment outcomes in older patients with SSNHL.
Materials and Methods
Patient Population
This retrospective study was conducted at Kaohsiung Medical University Hospital in Taiwan. The medical records of older patients (age >65 years) who were newly diagnosed with SSNHL between January 2009 and August 2019 were collected and reviewed. SSNHL was diagnosed as sensorineural hearing loss of at least 30 dB at 3 contiguous frequencies within 3 days, as determined through pure-tone audiometry. 1 The exclusion criteria were hearing loss caused by acoustic neuroma, central lesions, Meniere’s disease, multiple sclerosis, infectious diseases, trauma, medication, noise, or ear surgery. The Meniere’s disease patients were diagnosed according to the diagnostic criteria of the 2015 Classification Committee of the Bárány Society for definite Meniere’s disease. 17 The uncontrolled hypertension, uncontrolled diabetes, and gastric ulcer were excluded. To rule out acoustic neuroma, all recruited patients received audiometry tests, including pure-tone audiometry and auditory brainstem-evoked responses, and magnetic resonance imaging. Information on demographic characteristics was obtained. Before treatment, all patients underwent routine blood and biochemistry tests, including measurement of albumin levels.
We recruited 328 older patients with SSNHL at Kaohsiung Medical University Hospital. All included patients had received oral prednisolone (1 mg/kg per day, maximum dose of 60 mg, gradually tapered within 14 days). All patients were followed up for at least 3 months after initial treatment at the outpatient department. To evaluate hearing improvement, the patients’ audiogram obtained at 3-month follow-up was compared with the audiogram taken at the time of SSNHL diagnosis. The pure-tone average (PTA) was calculated as the average of hearing abilities measured at the following 4 frequencies: 500, 1000, 2000, and 4000 Hz. The hearing outcomes after treatment were assessed according to Siegel’s criteria. 18 The complete recovery group included patients with the final hearing abilities of <25 dB. The partial recovery group included patients with hearing recovery >15 dB, with the final hearing abilities between 25 and 45 dB. The slight recovery group included patients with hearing recovery >15 dB, with the final hearing abilities >45 dB. The nonrecovery group included patients with hearing recovery <15 dB, with the final hearing abilities >75 dB. Complete recovery and partial recovery were considered favorable outcomes, whereas slight improvement and no improvement were considered unfavorable outcomes.
Geriatric Nutritional Risk Index
The GNRI is an objective, simple, and easily available tool for clinical practice because this index only requires measurements of body weight, height, and serum albumin level. 9 GNRI was calculated using the following equation incorporating BW and serum albumin: 14.89 × albumin (g/dL) + 41.7 × (BW/ideal BW). The ideal BW was calculated as 22 × (body height (m)) 2 . BW/ideal BW was defined as 1 when the patient’s BW exceeded the ideal BW. 19
Statistical Analysis
Continuous variables are expressed as mean ± standard deviation (SD), and categorical variables are expressed as frequencies. The Independent t test, Chi-square test, and Fisher’s exact test were used to compare the distributions of baseline characteristics between SSNHL patients with favorable and unfavorable outcomes. A receiver operating characteristic (ROC) curve was used to estimate the discriminative cutoff value of GNRI associated with clinical outcomes in older patients with SSNHL. Multivariate logistic regression was used to calculate adjusted odds ratios (aORs) with 95% CI for the factors influencing clinical outcomes in older patients with SSNHL. All statistical analyses were performed using JMP software for Windows, version 10.0 (SAS Institute Inc., Cary, NC, USA). Two-tailed P values <.05 were considered significant.
Results
Clinical Characteristics of Study Participants
The baseline clinical characteristics of the study participants are provided in Table 1. A total of 328 older patients with SSNHL were included in the present study. According to Siegel’s criteria for hearing recovery, the study participants were divided into favorable and unfavorable outcome groups. The unfavorable outcome group included 221 patients (67.38%), comprising 122 (55.20%) men and 99 (44.80%) women. The favorable outcome group included 107 patients (32.62%), comprising 47 (43.93%) men and 60 (56.07%) women. The mean age of participants was 70.80 ± 4.62 years. The mean ages were 71.07 ± 4.90 years and 70.24 ± 3.95 years in the unfavorable and favorable outcome groups, respectively. The right ear was affected in 157 (47.87%) patients and the left ear in 171 (52.13%) patients. The average duration from the onset of hearing loss to the initiation of treatment was 5.36 ± 4.69 days. No significant differences were noted in age, sex, lesion side, and duration from hearing loss onset to treatment initiation between the favorable and unfavorable outcome groups. In addition, the prevalence rates of smoking, diabetes mellitus, and hypertension were not significantly different between the unfavorable and favorable outcome groups.
Demographic Characteristics of Older Patients With SSNHL (N = 328) According to Steroid Treatment.

Abbreviations: GNRI, geriatric nutritional risk index; HL, hearing loss; PTA, pure-tone average; SD, standard deviation; SSNHL, sudden sensorineural hearing loss.
Independent t test.
Chi-square test.
Fisher exact test.
P < .05.
Factors Influencing Clinical Outcomes in Older Patients With SSNHL
In this study, some of the older patients with SSNHL had associated symptoms such as vertigo (26.52%), tinnitus (78.96%), and aural fullness (42.68%). None of the symptoms significantly influenced hearing outcomes, except for vertigo (P = .0002) (Table 1). The initial PTAs (mean ± SD) of the affected ear were 79.64 ± 17.67 dB and 73.84 ± 22.38 dB in the unfavorable and favorable outcome groups, respectively. The initial hearing loss was significantly worse in the unfavorable outcome group than in the favorable outcome group (P = .0114) (Table 1). The final PTAs (mean ± SD) of the affected ear were 66.16 ± 23.15 dB and 38.65 ± 16.28 dB in the unfavorable and favorable outcome groups, respectively (P < .0001) (Table 1). In older patients with SSNHL, the hearing status of the unaffected contralateral ear was 38.35 ± 23.37 dB. The initial PTAs (mean ± SD) of the unaffected ear were 39.18 ± 24.95 dB and 36.65 ± 17.21 dB in the unfavorable and favorable outcome groups, respectively. There was no significant difference between the unfavorable and favorable groups regarding the unaffected ear hearing thresholds (P = .3192). The most common hearing loss type was the flat type (60.37%), followed by the total hearing loss type (32.01%). The prevalence of the low-tone hearing loss type (3.96%) and high-tone hearing loss type was low (3.66%).
GNRI and Older Patients With SSNHL
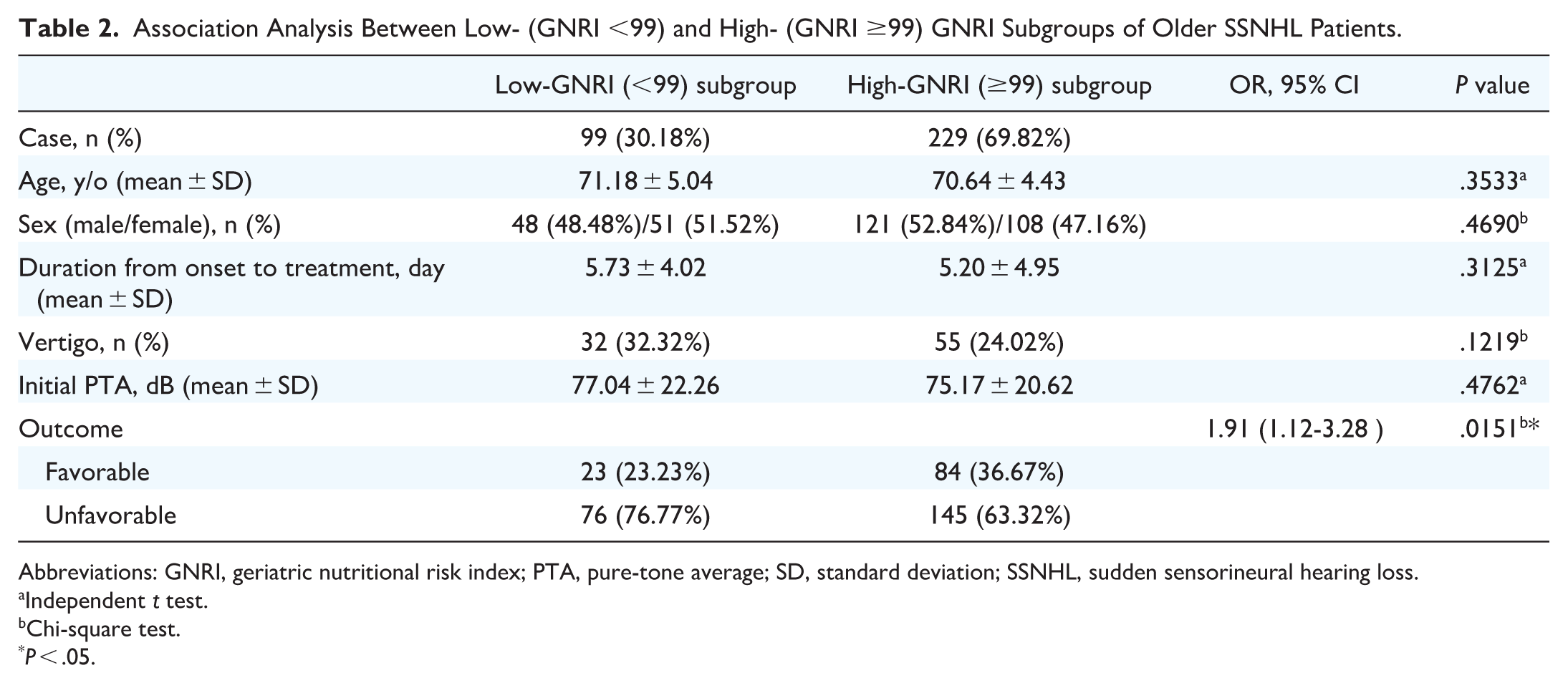
Comparing GNRI in the 2 groups, we found that the unfavorable outcome group had significantly lower GNRI than the favorable outcome group (P = .0201) (Table 1). The ROC analysis revealed that the area under the curve was 0.576 for GNRI in relation to clinical outcomes in older patients with SSNHL. In the ROC analysis, GNRI <99 and GNRI ≥99 were the cutoffs for defining the low-GNRI subgroup and high-GNRI subgroup, respectively. The low-GNRI subgroup included 99 (30.18%) patients, and the high-GNRI subgroup included 229 (69.82%) patients. No significant differences were found in age, sex, duration from hearing loss onset to treatment initiation, vertigo, and initial level of hearing loss between the low- and high-GNRI subgroups (Table 2). Older patients with SSNHL with low GNRI exhibited significantly unfavorable hearing outcomes (OR = 1.91, 95% CI = 1.12-3.28, P = .0151) (Table 2).
Association Analysis Between Low- (GNRI <99) and High- (GNRI ≥99) GNRI Subgroups of Older SSNHL Patients.
Abbreviations: GNRI, geriatric nutritional risk index; PTA, pure-tone average; SD, standard deviation; SSNHL, sudden sensorineural hearing loss.
Independent t test.
Chi-square test.
P < .05.
Table 3 presents the results of multivariate logistic regression models based on GNRI subgroups and prognostic factors, including age, duration from hearing loss onset to treatment initiation, vertigo, and initial level of hearing loss. Further multivariate logistic regression analysis of independent factors revealed that patients with vertigo (aOR = 3.45, 95% CI = 1.85-6.81, P = .0002), worse initial level of hearing loss (per 1 unit increase in hearing loss elevates the risk of poor hearing recovery by 2%, P = .0015), and low GNRI (aOR = 1.79, 95% CI = 1.03-3.18, P = .0435) were at higher risk of unfavorable outcomes (Table 3).
Multivariate Logistic Regression Analysis of Clinical Outcomes of Older Patients With SSNHL.

Abbreviations: aOR, adjusted odds ratio; GNRI, geriatric nutritional risk index; PTA, pure-tone average; ref, reference category; SSNHL, sudden sensorineural hearing loss.
aORs of unfavorable outcomes by age, duration from onset to treatment, vertigo (Y/N), initial PTA, and GNRI (Low/High) subgroup among the 328 older patients with sudden sensorineural hearing loss (age >65 years).
P < .05.
Discussion
In this study, we demonstrated that the nutritional status plays an important role in predicting clinical outcomes in older patients newly diagnosed with SSNHL. To the best of our knowledge, this study is the first to investigate the influence of GNRI, which includes the main objective parameters of albumin level and BMI, on clinical outcomes in older patients with SSNHL. GNRI may be related to the prognosis of older patients with SSNHL. GNRI in the unfavorable outcome group was significantly lower than that in the favorable outcome group. Our results revealed that the cutoff value of GNRI (99), which was calculated using ROC, is predictive of clinical outcomes in older patients with SSNHL.
Malnutrition is a complex state comprising a reduction in protein reserves, caloric collapse, and weakening of immune defenses. 9 There are no standard definitions or indices of malnutrition in patients. Historically, weight loss, low BMI, and low serum albumin level have been used to identify patients with malnutrition. Considering that these single parameters have a limited ability to assess nutritional status and predict prognosis, several models combining multiple parameters have been proposed. 9 The GNRI was originally developed as a new index for evaluating at-risk elderly patients. Although GNRI has not been assessed in SSNHL, a previous study has associated hypoalbuminemia with an increased risk and poor outcome of SSNHL. 8
Nutritional status is commonly assessed by measuring albumin levels. The albumin level is commonly low in patients with acute and chronic diseases. The albumin level not only provides valuable information on the prognosis of diseases but also is a biomarker of infection and inflammation. 8 Several studies have reported that albumin plays an active role in the pathophysiology of thrombosis, coagulation, and atherosclerosis.8,20,21 A low albumin level, even within the normal range, is associated with myocardial infarction, coronary heart disease, and stroke-related morbidity and mortality.8,21 The etiology of SSNHL involves viral infection, vascular disease, autoimmunity, and genetic factors. 4 Several studies have demonstrated that in older patients, SSNHL may be caused by vascular insufficiency.15,22 Previous studies have revealed that inflammation-related, thrombosis-related, coagulation-related, oxidative stress-related, heat shock protein, and steroid hormone receptor genes were associated with susceptibility to SSNHL.3,23 -27 Given the inflammatory and microcirculation basis of the pathogenesis of SSNHL, albumin levels should be assessed before initiating treatment to predict the prognosis of hearing loss. Zheng et al demonstrated that low serum albumin levels are a potential predictive marker of and unfavorable prognostic factor for SSNHL in China. 8 Low albumin levels indicate systemic inflammation and impaired immune function, which may be detrimental to the healing process, especially in delicate patients in the post-operative setting. 10
Metabolic syndrome encompasses a group of common conditions, including abdominal obesity, hypertension, insulin resistance, and dyslipidemia. A meta-analysis revealed the increased prevalence of SSNHL in patients with metabolic syndrome; the results also indicated a significantly higher likelihood of unfavorable prognosis among patients with SSNHL with metabolic syndrome than among those without metabolic syndrome. 28 The mechanism for SSNHL development in patients with metabolic syndrome may involve vascular disease. 28 In Korea, Lee et al found a significant association between increased BMI and both the prevalence and unfavorable prognosis of SSNHL, and in Taiwan, Wang et al highlighted normal weight central obesity as an unfavorable prognostic factor for SSNHL.6,7 These results indirectly support that the mechanism for SSNHL development involves vascular disease.
Studies have indicated that hearing outcomes in patients with SSNHL are influenced by several factors, including age, duration from hearing loss onset to treatment initiation, vertigo, and initial PTA.13 -15 Consistent with these results, in the present study, vertigo and the severity of initial hearing loss influenced clinical outcomes in older patients with SSNHL. By comparing the prognosis factors of different outcome groups, we found that the unfavorable outcome group had significant vertigo (P = .0002), worse initial level of hearing loss (P = .0114), and lower GNRI (P = .0201) than the favorable outcome group. Patients with SSNHL in the low-GNRI subgroup exhibited significantly worse hearing outcomes (OR = 1.91, 95% CI = 1.12-3.28, P = .0151). In the multivariate logistic regression analysis adjusted for the aforementioned factors, in addition to vertigo and the initial PTA, GNRI was an independent factor for clinical outcomes in older patients with SSNHL. The multivariate logistic regression indicated that patients with low GNRI (aOR = 1.79, 95% CI = 1.03-3.18, P = .0435) were at high risk of unfavorable outcomes. Our results also revealed that vertigo (aOR = 3.45, 95% CI = 1.85-6.81, P = .0002) and the initial level of hearing loss (per 1 unit increase in hearing loss elevates the risk of poor hearing recovery by 2%, P = .0015) showed strong associations with the treatment outcomes in older patients with SSNHL. According to Siegel’s criteria for hearing recovery, Attanasio et al and Chen et al have reported favorable outcomes in 38% of older patients with SSNHL in Italy and 46.67% in Taiwan.14,29 In the present study, 32.62% of older patients with SSNHL exhibited favorable outcomes.
The risk of complications related to steroid use may be higher in older patients with SSNHL than in younger patients with SSNHL. 16 However, in older patients with SSNHL, the conventional high-dose steroid regimen may lead to superior hearing recovery than low-dose steroid treatment. 30 In this study, we applied the high-dose steroid regimen for older patients with SSNHL.
In this study, we demonstrated that the nutritional status may play an important role in predicting clinical outcomes in older patients newly diagnosed with SSNHL. Our findings support that GNRI is highly predictive of clinical outcomes in older patients with SSNHL receiving steroid regimens. Our study incorporated the nutritional status into the evaluation, and the results demonstrated that GNRI, which can be determined using regular blood tests and body size measurement at diagnosis, is a feasible prognostic factor for SSNHL in older patients. GNRI more effectively reflects nutrition-related risk than albumin or BMI alone.11,12 Although the optimal cutoff values of GNRI might differ for patients with different illnesses and ethnic groups, lower GNRI tends to be associated with higher unfavorable outcomes.
Drawing from these findings, we suggest that patients with low GNRI may benefit from nutritional interventions and tailored treatment strategies to improve their quality of life and prognosis. 11 In the short term, lowering GNRI, especially through BW loss, is difficult. However, increasing albumin levels is relatively easier. A new highlight may be the potential to improve the outcome of SSNHL by altering nutritional status. Nutritional supplementation agents may have potential for the treatment of SSNHL patients who have lower GNRI and merit further investigation.
This study has some limitations. First, the retrospective nature of this study may introduce reporting bias into the results. A multicenter study should be conducted to confirm the study findings. Second, only the baseline nutritional status was assessed, without longitudinal assessment of nutritional status. Thus, nutritional status during treatment and its effect on clinical outcomes remain to be clarified. Third, GNRI was measured only on admission; thus, its change over time could not be examined. Fourth, the GNRI was mostly used as a nutritional parameter in head and neck cancer, especially in Eastern Asia countries, including Japan, China, and Taiwan, and only a few studies were conducted in the United States and Australia.9 -11 Area under the curve of 0.576 may indicate limited discrimination. In populations with high homogeneity or less variation in nutritional status, the area under the curve value for nutritional indices like GNRI may naturally be lower. Further studies involving different ethnic groups are required to generalize our results. Fifth, this study was limited to patients older than 65 years old; future research could explore its applicability to younger patients. Lastly, this study did not include a healthy control group for comparing GNRI between patients with SSNHL and normal controls.
Conclusion
In summary, this study investigated prognostic factors for SSNHL in older patients. The results revealed that in addition to the initial PTA level and vertigo, GNRI may be an independent prognostic factor for SSNHL in older patients. The GNRI is a quick, cost-effective method for assessing nutritional status since it only requires BW and height measurements along with a serum albumin analysis. Our study demonstrates the differing GNRI scores between unfavorable and favorable outcomes of SSNHL patients, underscoring the importance of nutritional status in SSNHL patients. Older patients with SSNHL who have vertigo, a worse initial level of hearing loss, and low GNRI exhibit unfavorable hearing outcomes. Our findings indicate that the nutritional status plays a crucial role in the initial treatment evaluation and prognosis. Conclusively, GNRI is a feasible prognostic factor for SSNHL in older patients.
Footnotes
Acknowledgements
This manuscript was edited by Wallace Academic Editing.
Author Contributions
Shu-Yu Tai: data collection, analysis and interpretation, manuscript writing and revision; Leong-Perng Chan: data collection, analysis and interpretation, and manuscript revision; Chin-Kuo Chen: data analysis and interpretation; Ning-Chia Chang: data collection, analysis and interpretation; Tadao Okayasu: data analysis and interpretation; Ling-Feng Wang: discussion and manuscript revision; Kuen-Yao Ho: discussion and manuscript revision; Chen-Yu Chien: study conception and design, data analysis and interpretation, manuscript revision.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Ministry of Science and Technology (MOST 108-2314-B-037-087), Kaohsiung Medical University Hospital (KMUH113-3M33), and Kaohsiung Municipal Ta-Tung Hospital (kmtth-110-011 and kmtth-112-012).
Ethics
This study was approved by the Institutional Review Board (IRB) of Kaohsiung Medical University Hospital (IRB approval No.: KMUHIRB-E(II)-20200379).