
Abstract
Importance
Modified Blair and Facelift incisions are conventional approaches to parotid pathologies. However, they frequently result in prominent scars in cosmetically sensitive regions. A newer alternative, U-shaped incision offers a minimally visible scar along the contour of the pinna while enabling management of parotid pathologies.
Objective
This study aimed to compare the cosmetic and surgical outcomes between U-shaped incision and conventional incisions including Modified Blair and Facelift incisions.
Design/Setting/Participants/Intervention or Exposures
This is a multicenter case-control study on 16 patients who underwent parotidectomy using U-shaped incisions for parotid tumors between 2019 and 2022. Seventeen disease characteristics-matched controls underwent conventional approach were included, amounting to a total of 33 patients.
Main Outcome Measures
The surgical outcomes including perioperative events, postoperative complications, and cosmetic outcomes using the Visual Analog Scale (VAS) score of scar satisfaction and the Patient Scar Assessment Scale (PSAS) were analyzed.
Results
There were no significant differences in the age (P = .817), tumor diameter (P = .398), and pathologies (P = .300) among the 2 groups. No significant differences in length of stays (P = .087) and resection margin (P = .117) were found. U-shaped incision group had a significantly less mean operating time (145 minutes, P < .001) and mean blood loss (10.45 ml, P = .043), compared to the conventional group which had 243 minutes and 43 ml, respectively. A significantly higher overall scar satisfaction based on VAS score in U-shaped incision group (P = .009) was noted. No significant differences between the 2 groups were found in the overall PSAS score and all the subscores. There were no significant differences in postoperative complications including facial nerve dysfunction (P = .520) between the 2 groups except the presence of a significantly higher sialocele in U-shaped incision group (P = .011).
Conclusion
The present study indicated that U-shaped incision is a safe alternative with better cosmetic outcomes over conventional incisions and comparable surgical outcomes.
Relevance
Surgeons are encouraged to adopt the U-shaped incision to achieve better cosmetic results while ensuring oncological safety.
Graphical abstract

Key Messages
U-shaped incision group showed comparable oncological safety and postoperative complications including the incidence of facial nerve dysfunction as the conventional incision group
U-shaped incision group can be regarded as a safe alternative with better cosmetic outcomes regardless of patient characteristics and tumor size and nature
Introduction
There has been an ongoing evolution of the parotidectomy incision since its first introduction in a bid to balance between adequacy of exposure and cosmetic outcomes. An adequate exposure of operative field ensures complete excision of the parotid lesion and allows delicate tissue handling for facial nerve preservation.1,2 However, lengthening of the incision to permit improved exposure may leave a noticeable scar which is less cosmetically appealing.
Modified Blair incision and facelift incision are the 2 most common conventional approaches to parotid pathologies.3,4 Despite their well-studied advantage in achieving adequate exposure, a conspicuous scar commonly remains in the cosmetically sensitive areas, causing facial disfigurement.5,6,7
In recent years, a newer alternative, U-shaped incision, is a minimally perceivable scar as it hugs the inferior contour of the pinna, extending anteriorly from the pre-tragal crease to the post-auricular crease posteriorly 5 (Figures 1 and 2). Therefore, this incision permits management of parotid pathologies without leaving any submandibular or cervical scars. 8
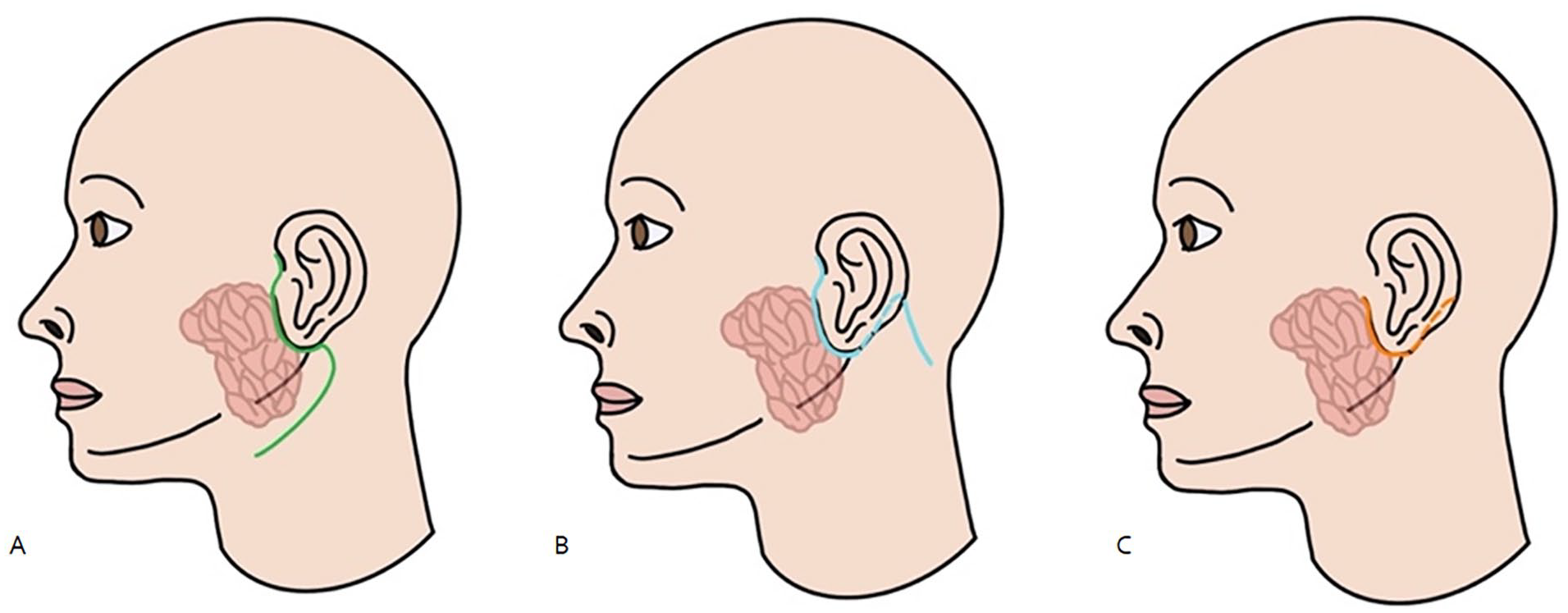
Schematic diagram of parotidectomy incisions. (A) Modified Blair incisions. (B) Modified facelift incision. (C) U-shaped incision.

(A) Preoperative view of the anterior limb of U-shaped incision (green line) compared to Imaginary Modified Blair incision (orange line). (B) Preoperative view of the posterior limb of U-shaped incision (green line); dotted circle refers to parotid tumor. (C) Intraoperative view with elevation of skin flap anteroinferiorly while retraction of parotid gland posterosuperiorly to visualize the main trunk and inferior trunk of facial nerve and greater auricular nerve through U-shaped incision. (D) Intraoperative view with manipulation of parotid tumor. (E) Preoperative view of another case of parotidectomy of deep lobe parotid tumor using U-shaped incision; dotted circle refers to parotid tumor. (F) Intraoperative view of manipulation of deep lobe tumor with identification of facial nerve branches.
Unfortunately, there are only limited studies assessing the functional, diseases, and cosmetic outcomes of parotidectomy using U-shaped incision to further validate their safety use in parotidectomy.9,11
The present study aimed to compare the cosmetic and surgical outcomes between U-shaped incision and conventional incisions including modified Blair and facelift incisions.
Materials and Methods
Study Design and Patient Eligibility
This is a prospective case-control study on patients with parotidectomies performed between 2019 and 2022 by specialists from the department of otorhinolaryngology, Head and Neck Surgery of Prince of Wales Hospital and Tseung Kwan O Hospital. Majority of the study would be retrospective data mining and analysis while the only prospective component would be the collection of subjective scar assessment scores through phone contact. This study has been approved by The Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee. Consent from patients was acquired and documented prior to collecting the data for assessment. Patients under the age of 18 were excluded from the study.
A case-control study was designed including 33 patients that were matched by age, sex, past medical history (hypertension, dyslipidemia, diabetes mellitus and renal disease), tumor diameter, and tumor depth. Sixteen cases of U-shaped incision parotidectomy performed from 2019 to 2022 in the included centers were matched to a group of 17 patients who underwent parotidectomy with the conventional incisions and matched by the above parameters. Tumors in all selected cases were within field of incision and were randomly assigned into the U-shaped and conventional incision groups.
Surgical Technique
Intraoperative facial nerve monitoring was employed throughout the procedures. Patients were positioned with a head ring and shoulder supports. The surgical field was prepared using standard aseptic techniques, with draping extended to the neck for exposure. A surgical pen was used to outline the tumor location and relevant surface anatomical landmarks.
Either one of the two incision types was utilized:
U-shaped incision: Extending from the pre-tragal crease to the post-auricular crease (Figure 2A, green line)
Modified Blair and Facelift incisions: Executed as per established protocols (Figure 2A, orange line)
A #15 scalpel was used to initiate the skin incision, followed by subcutaneous flap dissection via monopolar diathermy. The flap was elevated anteriorly over the parotidomasseteric fascia, inferiorly over the sternocleidomastoid muscle, and circumferentially around the lesion. The U-shaped incision’s limited exposure necessitated strategic use of Langenbeck retractors and adjustments in patient head positioning to optimize access. The greater auricular nerve was identified and preserved whenever feasible. Tumor excision adhered to standard parotidectomy principles using conventional incisions. Hemostasis was secured, and a drain was placed. Subcutaneous layers were approximated with Vicryl sutures, while skin edges were reapproximated using Ethion sutures. Skin sutures were removed on postoperative day 7.
Outcome Measurements
Patient demographics including age, gender, past medical history, side of operation, tumor diameter, tumor depth, and tumor pathology were documented. Each tumor diameter defined as the longest dimension of the lesion. The type of incision used for each patient was recorded as either U-shaped incision or conventional incisions (ie, modified Blair or facelift incision).
The primary outcome was subjective scar assessment using Visual Analog Scale (VAS) of patient scar satisfaction (0-10) and the Patient Scar Assessment Scale (PSAS) taken from the Patient and Observer Scar Assessment Scale (POSAS) which includes changes in scar color, stiffness, thickness, irregularity of the scar, itchiness, and associated pain12,22 (Figure 3). These cosmetic scores were taken at least 12 months postoperatively. Secondary outcomes were perioperative metrics including the operating time, total blood loss, resection margins status, intraoperative complications, duration of hospital stay, injury, or sacrifice of the greater auricular nerve and facial nerve as well as postoperative outcomes including facial nerve dysfunction, earlobe numbness, seroma/sialocele, infection, hematoma, scar complications, and Frey’s syndrome. Transient facial nerve paresis was defined as full recovery of facial nerve function by 24-week follow-up while permanent paresis as persistent facial nerve paralysis beyond 24-week follow-up, aligning with prior studies reporting recovery of facial nerve function post-parotidectomy by 24 to 36 weeks regardless of pathologies.23 -25

Patient and Observer Scar Assessment Scale.
Statistical Analyses
IBM (Armonk, New York, USA) SPSS version 28.0 was utilized. Continuous variables were presented as means with standard deviation while categorial variables in descriptive statistics. Nonparametric test, Mann-Whitney test was used to analyze all continuous variables. Chi-square test and Fisher’s exact test were used to compare categorical variables between the groups. Statistical significance was defined as P < .05, and P values were 2-sided.
Results
Thirty-three patients with a mean age of 58.0 years (95% CI, 52.8-63.1 years) were included in the study. There were 11 (33.3%) male patients and 22 (66.7%) female patients. Mean period of follow-up was 22.3 months. Table 1 shows the preoperative patient’s characteristics of the studied groups. The parotid lesions were most frequently situated in the superficial lobe, accounting for 25 cases. Lesions within the deep lobes were seen in 2 cases and both lobes in 6 cases. The mean tumor diameter was 19.9 mm in U-shaped incision group and 25.6 mm in conventional incision group with no significant differences, while the largest diameter for U-shaped incision group was 55 mm versus 40 mm in conventional incision group. There were 27 benign tumors and 6 malignant tumors included in this study, with the most common pathology being pleomorphic adenoma which accounted for 18 (54.5%) cases. Malignant tumors included acinic cell carcinoma and low-grade mucoepidermoid carcinoma. There were no significant differences between the 2 groups among all the preoperative characteristics of the patients.
Patients’ Preoperative Characteristics in Each Group.

Taken from the longest dimension.
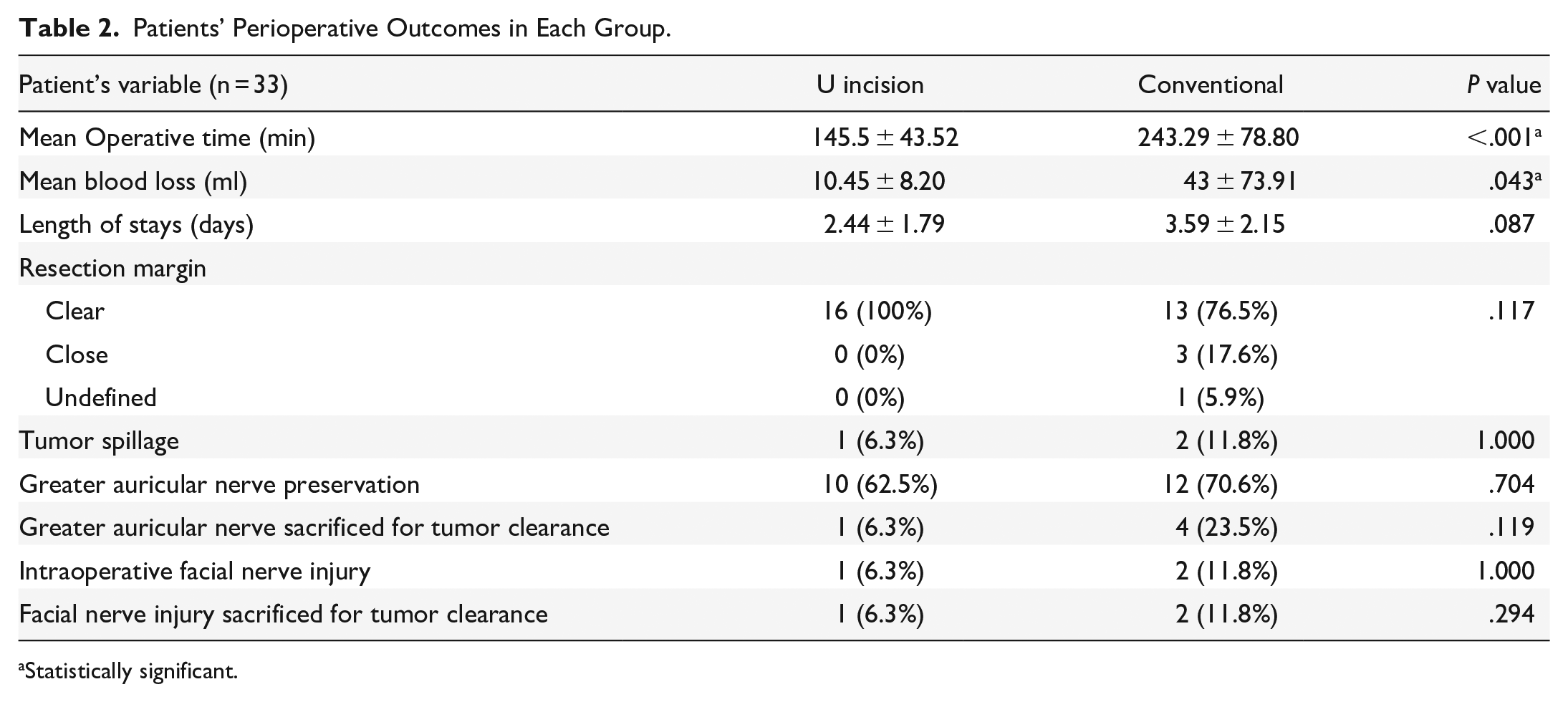
Regarding the perioperative outcomes (Table 2), the mean operative time of 145.5 minutes in U-shaped incision group (95% CI 124-167 minutes) was significantly shorter than the duration of 243.3 minutes in conventional incision group (95% CI 206-281 minutes) (P < .001). The mean amount of blood loss in the U-shaped incision group was 10.5 ml (95% CI 6.4-14.5 ml) which was significantly smaller than the amount of 43 ml (95% CI 7.9-78.1 ml) in conventional incision group (P = .043). The length of stay was 2.44 days (95% CI 1.56-3.32 days) in U-shaped incision group; however, it was 3.59 days (95% CI 2.57-4.61 days) in conventional incision group.
Patients’ Perioperative Outcomes in Each Group.
Statistically significant.
One patient (6.3%) from U-shaped incision group and 2 patients (11.8%) from conventional incision group were complicated by tumor spillage, which is defined as a violation of the tumor capsule. No significant difference was found between length of stay (P = .087), or tumor spillage (P = 1.000) among the 2 groups. Clear resection margin was achieved in majority of patients, accounting for 16 cases (100%) in U-shaped incision group and 13 cases (76.5%) in conventional incision group. Majority of patients had their greater auricular nerve preserved as U-shaped incision group had 10 patients (62.5%) while conventional incision group had 12 patients (70.6%).
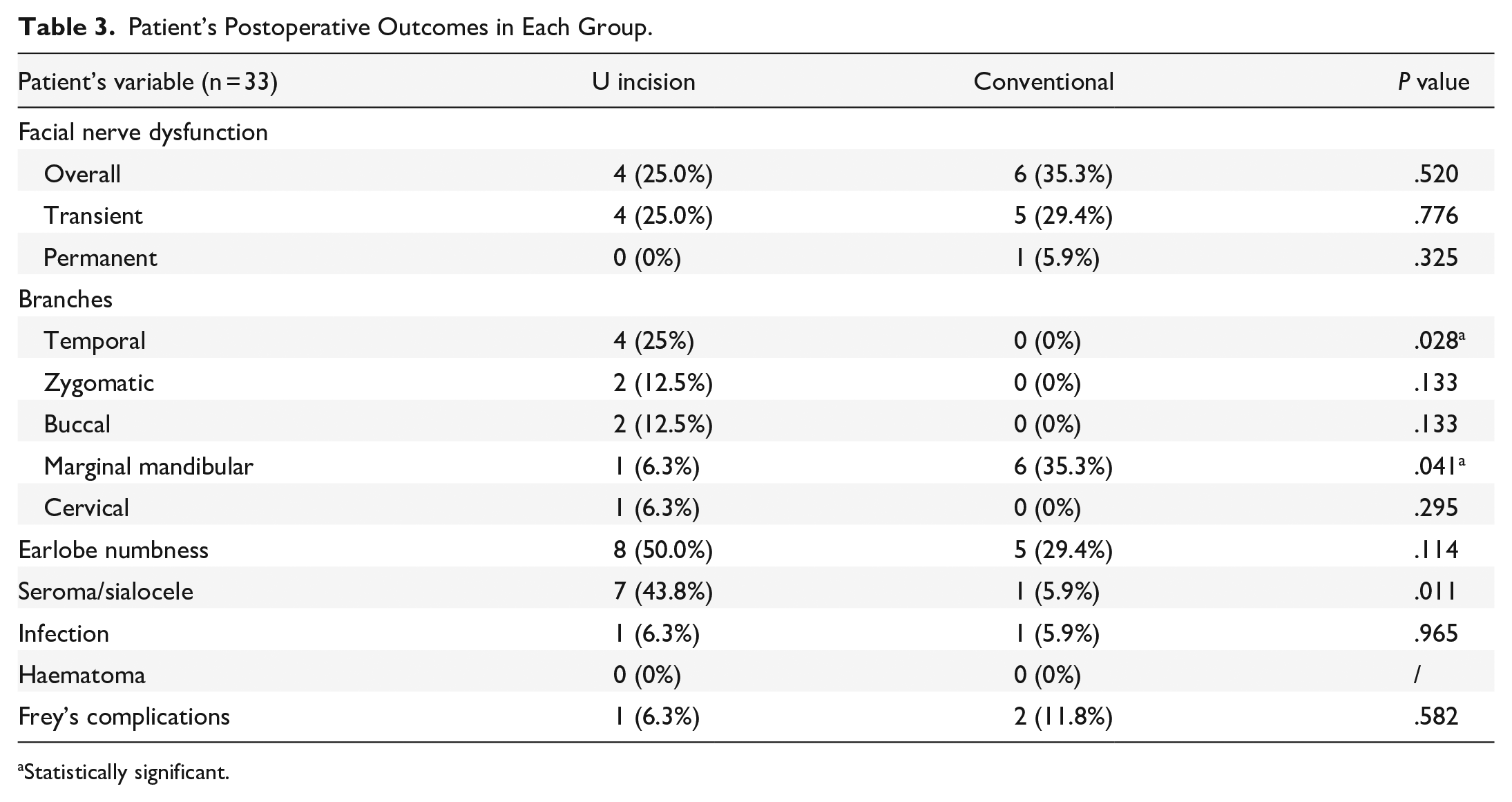
Concerning the postoperative outcomes (Table 3), postoperative facial nerve dysfunction of one or more nerve branches was noted in 4 cases (25%) in U-shaped incision group and 6 cases (35.3%) in conventional incision group. Four cases (25%) from U-shaped incision group and 5 cases (29.4%) from conventional incision group showed transient facial nerve paresis of one or more nerve branch. Zero cases (0%) from U-shaped incision group and 1 case (5.9%) from conventional incision group reported sustained facial nerve paralysis of one or more nerve branch after 24-week follow-up, as known as permanent facial nerve paralysis. No significant differences in the incidence of transient paresis (P = .776) and permanent palsy (P = .325) between the 2 groups were shown. Among all branches of the facial nerve, the U-shaped incision group reported 4 cases (25%) of temporal branch paresis, which was significantly higher than the conventional incision group, which had 0 cases (0%) (P = .028). Importantly, all 4 cases of facial nerve dysfunction involving the temporal branch in the U-shaped incision group were transient. In addition, the conventional incision group had 6 cases (35.3%) of facial nerve dysfunction involving the marginal mandibular branch, significantly higher than the U-shaped incision group (1 case, 6.3%) (P = .041). No significant differences between the 2 groups were reported for the remaining facial nerve branches.
Patient’s Postoperative Outcomes in Each Group.
Statistically significant.
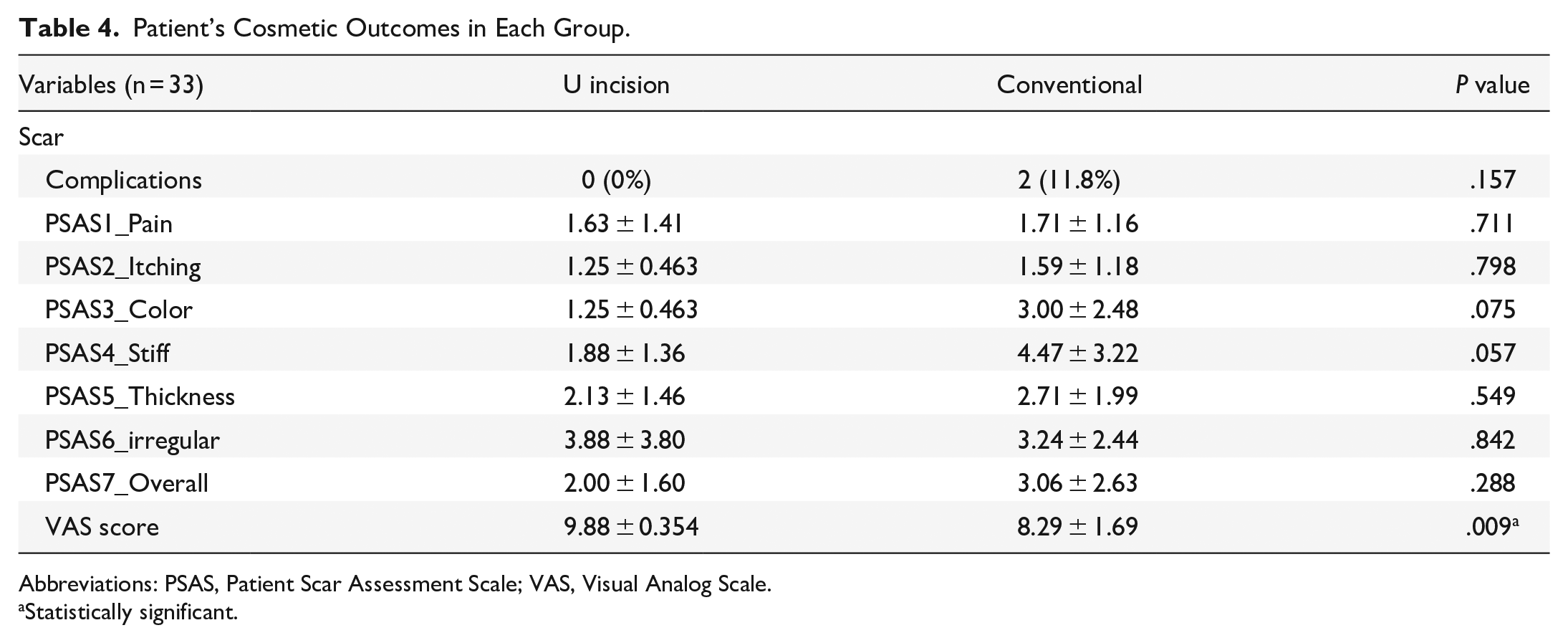
Eight patients (50.0%) in U-shaped incision group and 5 patients (29.4%) in conventional incision group developed greater auricular nerve numbness. The incidence rate of seroma and sialocele in U-shaped incision group (7 patients, 43.8%) was significantly higher than those in conventional incision group (1 patient, 5.9%) (P = .011). Both groups had 1 patient (6.3% in U-shaped incision group; 5.9% in conventional incision group) developed postoperative wound infection while 1 patient (6.3%) from U-shaped incision group and 2 patients (11.8%) from conventional incision group had Frey’s syndrome. No hematoma was found in both groups. There were no scar complications including hypertrophic scar, thickening of skin or gap dehiscence of wound reported in the U-shaped incision group, while it was observed in 2 (11.8%) patients in conventional incision group (see Table 4). There were no significant differences in these postoperative scar complications between the 2 groups (P = .157).
Patient’s Cosmetic Outcomes in Each Group.
Abbreviations: PSAS, Patient Scar Assessment Scale; VAS, Visual Analog Scale.
Statistically significant.
Regarding the cosmetic outcome, our study reported significant differences between the 2 groups in the VAS of patient scar satisfaction with U-shaped incision group having a higher score of 9.88 (95% CI 9.71-10.0) versus 8.29 (95% CI 7.49-9.09) in conventional group (P = .009). For the PSAS outcome in which lower scores represent resemblance to normal surrounding skin, there were no significant differences between the 2 groups in all parameters of PSAS. U-shaped incision group achieved a lower overall score of 2.00 (95% CI 1.22-2.78), in contrast to the score of 3.06 (95% CI 1.81-4.31) in the conventional incision group. Among the parameters, the U-shaped incision group demonstrated lower mean scores across several measures: pain was reported at 1.63 (95% CI 0.94-2.32), itchiness at 1.25 (95% CI 1.02-1.48), color at 1.25 (95% CI), stiffness at 1.88 (95% CI 1.21-2.55), and thickness at 2.13 (95% CI 1.42-2.85). Conversely, the conventional incision group exhibited higher mean scores: pain was reported at 1.71 (95% CI 1.16-2.26), itchiness at 1.59 (95% CI 1.03-2.15), color at 3.00 (95% CI 1.82-4.18), stiffness at 4.47 (95% CI 2.89-6.05), and thickness at 2.71 (95% CI 1.76-3.66).
Discussion
The absence of descending limb down the hairline theoretically enables the periauricular incision to optimize cosmesis by hiding the scar of the posterior limb within the post-auricular skin crease. Theoretically, wound remodeling after 3 months is strongly predictive of the eventual scar evolution. 37 Our study evaluated the cosmetic satisfaction at >12 months postoperatively—exceeding the 3-month threshold linked to scar stabilization—using VAS and PSAS from POSAS, a tool theorized to offer improved reliability over Vancouver Scar Scale (VSS) 36 and was not adopted in previous studies (Table 5). Our findings demonstrated a significantly higher mean VAS score of 9.88 in the U-shaped incision group than the mean VAS score of 8.29 in the conventional group, aligning with prior studies.8,10,11 ,13 -16 The U-shaped incision group also reported lower overall PSAS score of 2.00 with higher patient satisfaction on the scar pain, itchiness, color, stiffness, and thickness. Patients were matched for chronic conditions affecting wound healing, for example, diabetes mellitus, renal disease to minimize confounding.
Current Study and Previous Studies Evaluating U-Shaped Incision.

Abbreviations: PSAS, Patient Scar Assessment Scale; SMAS, Superficial Musculoaponeurotic System; VAS, Visual Analog Scale; VSS, Vancouver Scar Scale.
Therefore, the studied skin incision is favored by authors in their approach in managing benign parotid pathologies as described in previous studies, which however reported limited cosmetic outcome data. Pagès et al 14 reported extremely satisfactory aesthetic results in what Pagès and his team termed as minimal incision (comparable to U-shaped incision in the present study). However, there was no formal scar assessment with validated tools listed. Roh et al 11 and Shaaban et al 10 reported a high median VAS score of 9 in assessing patient’s satisfaction with the scar appearance and a significantly higher VAS score in periauricular incision group (comparable to U-shaped incision in the present study) than standard Blair’s incision group, respectively. Ahn et al 13 described a higher degree of cosmetic satisfaction from 14 patients with a mean VAS of 9 and mean VSS of 0.9. Therefore, our study affirmed the anesthetic superiority of U-shaped incision over conventional incision as suggested by previous studies.
Another key issue is whether the U-shaped incision permits safe disease control since the shorter length of the incision in U-shaped incision may undermine the exposure and manipulation of the tumor, putting the facial nerve in jeopardy.10,13,15,17 Some authors suggested that U-shaped incision come short of adequately exposing the tumors located at the inferior pole or parotid tail, requiring an extension of the U-shaped incision to face-lift incision.10,13,16,17 Other studies reported no limitations in achieving adequate exposure by U-shaped incision in any tumor location.9,11,14 Roh et al stated that tumors located in the inferior, anterior, or superior poles were not associated with increased complication rates as compared to middle tumor location. 11 Except for the significantly higher incidence rate of sialocele, our present study showed similar results as in previous studies,10,11,13 that the postoperative outcome of U-shaped incision group was comparable to conventional incision group irrespective of the tumor diameter and depth. Although the retrospective nature of the present study limited its ability to precisely locate the tumor and to evaluate whether the location would limit the feasibility of U-shaped incision, tumor located at the inferior pole appears not to be an absolute limitation of the U-shaped incision given the versatility of the U-shaped incision allowing extension of the incision to be done readily for better exposure in difficult cases. 13 Such flexibility allows pursuing better esthetic outcomes while not sacrificing tumor clearance.
Our study demonstrated that the U-shaped incision provided comparable oncological safety to conventional approaches, even when applied to tumors of varying depths and pathologies including low-grade malignancies and deep lobe lesions. While prior studies predominantly restricted the U-shaped technique to superficial lobe benign tumors with exclusion to malignancies and deep lobe cases due to concerns over radial resection adequacy.9,10,11,13,17 Our cohort achieved clear resection margin in 100% of U-shaped cases with 93.8% showing no tumor spillage. For low-grade malignancies, margins adhered to the NCCN-recommended threshold of ≥1 mm 34 while benign tumors met ESGS criteria of intact tumor capsule and absence of residual cells. 35 However, further discussion on the oncological implication of U-shaped incision for malignancy cases is warranted as long-term recurrences rates which was not included in our study remain critical to confirm its procedural safety.
Our study found a 25% incidence of transient facial nerve paresis in the U-shaped incision group compared to 35.3% in the conventional group. Notably, no permanent facial nerve paralysis occurred with the U-shaped approach, whereas 1 case (5.9%) was observed in the conventional group. Permanent nerve injuries in our cohort were attributed to intraoperative facial nerve branch sacrifice and inclusion of parotid lesions of any pathologies and locations which are established determinants of facial nerve outcomes.18,19 Critically, no significant difference in overall facial nerve injury rates was observed between the 2 techniques. These findings align with prior studies reporting transient nerve dysfunction while no permanent palsy following parotidectomy for superficial lobe benign tumors using minimally invasive approaches (eg, periauricular incisions).1,11,13,16 Given the facial nerve’s pivotal role in dictating functions of facial muscles responsible for facial expression and hence aesthetic outcomes, 20 its preservation remains paramount. Our results suggest that the U-shaped incision, while accommodating diverse tumor pathologies and depths, does not compromise nerve safety. This approach may thus offer a viable alternative to conventional methods, balancing oncological rigor with optimal functional and cosmetic results.
The present study showed a significant shorter operating time of 145.5 minutes in U-shaped incision group than of 243.3 minutes in conventional incision group after taking covariates tumor pathology or depth into account. On contrary to previous studies (see Table 5), Shaaban et al reported a significantly longer operating time with a mean of 100.8 minutes in periauricular incision group than of 92.5 minutes in modified Blair’s incision group. 10 Shaaban and his team attributed the longer operating time to inclusion of different extent of parotidectomy such as superficial, partial, or total parotidectomy and more flapping and retractions involved in U-shaped incision. 10 Other studies, including those by Pages et al, reported an average operating time of 115 minutes for parotidectomy via periauricular incision, 14 while Roh noted a median operating time of 55 minutes, with no significant variances based on tumor location. 11 The variations in operative duration compared to earlier reports likely stem from differences in surgical technique, instrumentation, surgeon expertise, and case selection such as tumor pathology, types of parotidectomy performed. Li et al noted a learning curve of 3 to 5 cases for minimizing operative time. 27 In addition, the U-shaped incision which is shorter in length facilitates a reduced suturing time. Regarding intraoperative blood loss, our current study demonstrated a significantly lower mean intraoperative blood loss of 10.5 ml in U-shaped incision group versus 43 ml in conventional incision group. This finding contrasts with previous studies (Table 5), including those by Roh et al, which reported a median blood loss of 36 ml in periauricular incision group. 11 Wang et al revealed a mean blood loss of 52 ml in U-shaped incision group and 48 ml in conventional incision group with no significant differences. 21 Tsao et al’s meta-analysis highlighted a possible link between significantly reduced blood loss in post-auricular approaches and employment of advanced instruments, for example, endoscopes, Harmonic scalpels, enabling precise dissection and hemostasis. 26 In our cohort, shorter operations and lower blood loss may reflect involvement of experienced head and neck surgeons who become adept at identifying dissection plane and modern instruments. However, multi-surgeon variability which was unaccounted in our analysis could influence outcomes. While our findings suggest U-shaped incisions offer practical advantages with shorter operating time and less intraoperative blood loss, critical limitations remain. The anticipated costs for parotidectomies utilizing U-shaped incision were expected to be similar to those of the conventional group as operative theater setting, nursing staff, mode of anesthesia were the same despite the lack of direct cost data. The duration of hospital stay between 2 groups showed no significant differences. Future studies should employ prospective designs with cost analyses and surgeon skill assessments to validate benefits while addressing learning curves and technical standardization.
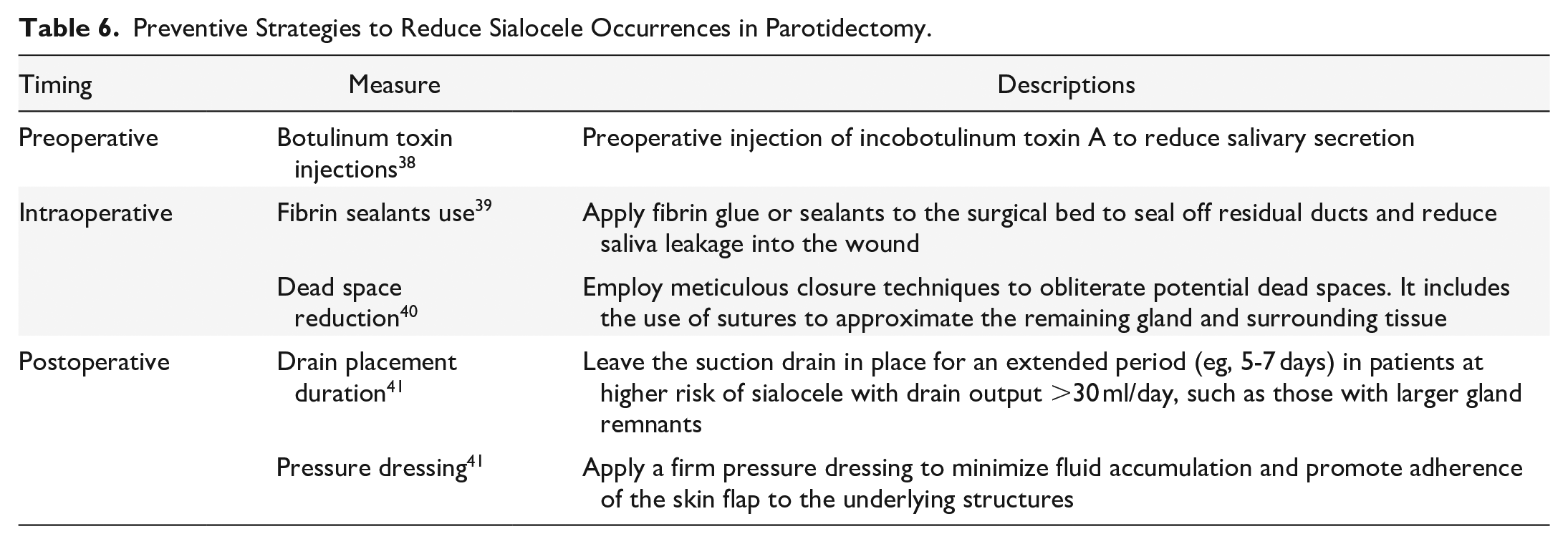
Our study identified a significantly higher incidence of seroma and sialocele in the U-shaped incision group (43.8%) compared to the conventional group (5.9%). While seroma arises from fluid accumulation in dead space, 28 sialocele reflects saliva leakage from residual glandular tissue 28 which often linked to surgical technique, gland preservation, or postoperative management. Prior studies propose contributing factors such as minimal resection extent leaving more functional gland tissue and hence increasing saliva production,29,31 -33 as seen in our U-shaped group with mean tumor diameter 19.9 mm versus 25.6 mm in conventional group, and the use of surgical implants such as surgicel, hemostatic sponges disrupting ductal systems.29,30 We hypothesize that the U-shaped technique’s smaller incisions may heighten risk of sialocele via 2 mechanisms. First, the shorter incision may inadvertently reduce direct visualization of surgical field, requiring greater tissue retraction that may potentially traumatize residual gland tissue. 29 Second, limited exposure could compromise meticulous duct ligation29,30 or dead space reduction. However, the retrospective design limited our ability to preclude definitive conclusions since variables like gland volume, implant use, tissue handling nuances, postoperative protocols such as use of pressure dressing were not recorded. To mitigate this complication, established strategies such as preoperative botulinum toxin injection, 38 prolonged drainage, 41 or fibrin sealants warrant exploration 39 (Table 6).
Preventive Strategies to Reduce Sialocele Occurrences in Parotidectomy.
There are several limitations in our study that warrant consideration. Our study’s dual approach with prospective cosmetic outcome evaluation and retrospective noncosmetic outcome assessment restricted our capacity to systematically analyze tumor localization and characteristics, tissue handling methods, and gland preservation from medical records, thereby introducing confounding factors in concluding the potential contributors to the observed elevated sialocele incidence, shorter surgical duration, less intraoperative hemorrhage, and oncological safety. The small sample size and multi-institutional variability in surgical techniques and perioperative care may constrain the generalizability and statistical power of our study. Also, operator-dependent differences stemming from varying surgeon experiences and technical executions could also influence outcomes despite standardized surgical approaches. Our study relies solely on subjective scales for scar assessment, introducing potential measurement bias. Future research should prioritize prospective multicenter studies with larger cohorts and extended follow-up to allow further subgroup analysis, cost analysis, oncological evaluation, and the use of objective scar evaluations tools, for example, Observer Scar Assessment Scale (OSAS) to address these limitations.
This study makes a novel contribution to the field of parotid surgery by being the first to utilize the PSAS in conjunction with the VAS for a comprehensive evaluation of scar outcomes. By including patients with low-grade malignancies and deep lobe tumors, the applicability of the U-shaped incision is significantly broadened, addressing gaps in previous research. In addition, our findings demonstrate notable operative efficiency, characterized by a shorter operating time and reduced blood loss compared to conventional incisional approaches. While we observed a higher incidence of seroma and sialocele (43.8%) in the U-shaped incision group versus the conventional group (5.9%, P = .011), we hypothesize that the shorter incisions may compromise surgical field visualization, potentially increasing ductal trauma that warrants further prospective studies for evaluation.
Conclusion
Parotidectomy using a U-shaped incision is a safe alternative that demonstrates comparable postoperative outcomes to conventional incisions, along with enhanced overall patient cosmetic satisfaction and ensured clear resection margins. This is the first local study providing preliminary evidence of the cosmetically superiority, comparable oncological safety, and possibly better cost-effectiveness in U-shaped incision. Future prospective studies further evaluating the surgical outcomes of U-shaped incision will be valuable for enhancing preoperative planning and surgical strategies for parotid tumors.
Footnotes
Acknowledgements
The authors acknowledge the assistance with administrative works and data collections of all involved research assistants at the department of otorhinolaryngology, Head and Neck Surgery under the Faculty of Medicine of the Chinese University of Hong Kong.
Author Contributions
David Chun Man Yeung and Jason Ying Kuen Chan designed the work; Jason Ying Kuen Chan, Zenon Wing Chi Yeung, Eric Hui Lun Lau, Ronald Lai, and Hon Kwan Andy Chan acquired data; Hei Man Nicole Fong analyzed the data & drafted the manuscript; David Chun Man Yeung revised and approved the manuscript; Hei Man Nicole Fong and David Chun Man Yeung agree to be accountable for all aspects of the work.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Data collected may include gender, age, pathological result, imaging result and medical comorbidities, etc. The data collected in this study will be kept confidentially without identification of the subject for 6 years and will be used for research purpose only. Documentation of verbal consent from patients who took part in this study has been made. We will not store personal identifiable data. All data will be stored in secured offices of the department of otorhinolaryngology, Head and Neck Surgery at the Prince of Wales Hospital. Only the investigators and research assistants from department of otorhinolaryngology, Head and Neck Surgery, Faculty of Medicine, the Chinese University of Hong Kong will have access to these records. Access to patient’s medical records and data collected during this study will be granted to institutional review board/ethics committee, and regulatory authorities for verification of the research study to the extent permitted by the applicable laws and regulations. This study has been reviewed and approved by The Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee. There is no funding for this research.