
Abstract
Objectives
The middle turbinate (MT) was considered related to olfactory function. Whether the MT should be partially resected during relevant surgery is still debated. Our primary objective was to compare the olfactory outcome between partial MT resection (MTR) and MT preservation (MTP).
Methods
A search was performed on the Cochrane Library, Embase, PubMed, Scopus, and Web of Science databases from their inception through February 10, 2024. Eligible studies included those that compared the olfactory outcome between partial MTR and MTP. Data were extracted manually, and a random-effects model was used to evaluate it. We calculated the standardized mean differences (SMD) in the scores for the olfactory function. Further subgroup analysis was also performed for variables of interest. The pooled results were examined using influence analysis.
Results
After systematically reviewing all relevant articles, 7 studies were qualified for inclusion. The pooled results showed no significant difference in olfaction between the partial MTR and MTP (SMD, 0.140; 95% CI, −0.159 to 0.438; P = .359; I2 <1%). Subgroup analysis preferred partial MTR in the objective test (SMD, 0.370; 95% CI, 0.17-0.56; P < .001; I2 = 0%). No significance was observed in studies with subjective test (SMD, −0.271; 95% CI, −0.604 to 0.63; P = .112; I2 <1%), undergoing functional endoscopic sinus surgery (0.10; 95% CI, −0.35 to 0.54; P = .67; I2 = 85%), undergoing skull base surgery with endoscopic endonasal approach (SMD, 0.25; 95% CI, −0.04 to 0.53; P = .09; I2 = 0%), and following up more than 6 months (SMD, 0.09; 95% CI, −0.21 to 0.39; P = .57; I2 = 75%).
Conclusion
Our findings showed that MTR does not deteriorate olfactory function compared with MTP. Considering the potential benefit, partial MTR might be prioritized in clinical settings.

Keywords
Highlights
Middle turbinate (MT) resection (MTR) during endonasal surgery did not significantly affect olfactory function compared to MT preservation.
Subgroup analysis showed that MTR revealed better olfactory outcomes assessed with objective tests.
Partial MTR can be prioritized in functional endoscopic sinus surgery and endoscopic endonasal approach without compromising olfactory outcomes.
Introduction
Olfactory perception plays a crucial role in human life, enabling individuals to locate food, distinguish tastes, avoid dangerous substances, 1 navigate spaces, 2 and even understand emotions. 3 It is also associated with choosing partners,4,5 enhancing memory, 6 and improving certain cognitive skills. 7 People experiencing olfactory impairments often face challenges in cooking, feelings of vulnerability, 7 and experiencing more severe depression and anxiety. 8 Moreover, a significant relationship between the loss of smell and increased mortality has been observed in several research studies.9,10
The olfactory epithelium is a sensory organ located in the superior recess of the nasal cavities, comprising the cribriform plate, the upper third of the nasal septum, and the upper portions of the superior turbinate (ST) and middle turbinate (MT).11,12 Injury to any of these structures may occur during endonasal surgery, resulting in olfactory impairment and even leading to anosmia. As medical technology has evolved, the precision and sophistication of endoscopic surgery have significantly improved. Consequently, the incidence of unintended damage to anatomical structures during these procedures has substantially decreased. 13 Nevertheless, during surgery, including functional endoscopic sinus surgery (FESS) or endoscopic endonasal approach (EEA) of skull base surgery, resection or manipulation of structures that are potentially responsible for olfaction is sometimes be required to expand the surgical field intraoperatively and prevent postoperative synechia as well. 14
Given its physiological function and role as an essential anatomical landmark,1,3,15,16 whether partial resection of the MT has remained controversial in recent years. Proponents and opponents hold perspectives regarding the benefits and potential physiological impacts of partial MT resection (MTR). Within this discourse, whether MTR leads to olfactory dysfunction represents the most contentious and uncertain issue.17,18
Despite the literature on the subject, there is still no definitive evidence to support this debate. To address this issue, our study sought to provide a comprehensive analysis through a systematic review and meta-analysis. We hope that this research will provide surgeons with more evidence-based guidance when considering partial resection of the MT during surgery.
Materials and Methods
Study Design
This study is a systematic review and meta-analysis that adheres to the guidelines outlined by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. 19
Search Strategy
The Cochrane Library, PubMed, Embase, Web of Science, and Scopus databases were searched for studies published from inception through February 10, 2024. Two citation subsets were used under the framework of Medical Subject Headings and text words: 1 including studies on concepts with turbinectomy (“Turbinate Resection,” “Nasal Surgery”) and 1 including concepts with olfaction disorders (“Smell Disorder” OR “Olfactory Impairment”). We did not exclude publications by language or country. The full search strategy is described in the Table S1.
The Eligibility Criteria
Two reviewers (Yen-An Chen and Chih-Hao Chen) selected the studies that met all of the following criteria: (a) the study was a randomized controlled trial or prospective trial involving patients undergoing MTR during endoscopic sinus surgery or endonasal skull base surgery; (b) the study compared MTR with MT preservation (MTP) and reported an outcome of olfactory function; and (c) the study provided adequate information to calculate the effect estimates for meta-analysis. No studies were excluded based on publication date or geographical area. However, articles written in languages other than English were excluded, as they would be difficult to appraise. In cases where there were discrepancies regarding the inclusion of a study, a third author (Ming-Ying Lan) would provide consensus or facilitate further discussion.
Data Extraction
Two reviewers (Yen-An Chen and Chih-Hao Chen) extracted datasets from the eligible studies. The extracted information included the author’s name, publication year, country, number and mean age of patients, type, and number of MTR, method of olfactory function test, type of surgery, and length of follow-up that had been assessed and reported. The coauthor (Ming-Ying Lan) would provide the final judgment when there was no consensus on data extraction.
Risk of Bias Assessment and Evidence Evaluation
Given the inclusion of both non-randomized and randomized studies in this review, we employed 2 appraisal methods: The Revised Risk of Bias 2 Tool for Randomized Trials (RoB 2) tool 20 and the Risk of Bias in Non-randomized Studies—of Interventions (ROBINS-I) tool. 21 RoB 2 is specifically designed for assessing the risk of bias in randomized controlled trials, while ROBINS-I evaluates the risk of bias in non-randomized studies of interventions to evaluate the methodological quality of the studies included. In addition, we employed the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) assessment to evaluate the overall quality of the evidence. 22 GRADE is a widely used framework for rating the certainty of evidence and the strength of recommendations in systematic reviews and guidelines. It evaluates evidence across several domains, including study limitations (risk of bias), inconsistency, indirectness, imprecision, and publication bias, providing a comprehensive and transparent assessment of evidence quality. Two reviewers (Yen-An Chen and Chih-Hao Chen) would perform the appraisal. In case of any disagreements, the coauthor (Ming-Ying Lan) was responsible for resolving them.
Statistical Analysis
To account for a potential second source of error in addition to sampling error, the researchers utilized the random-effects model for effect size calculation. The Cochran Q test and the I2 statistic were used to evaluate statistical heterogeneity, with I2 values indicating low, moderate, and high heterogeneity at <50%, 50% to 74%, and ≥75%, respectively. 23 To explore the impact of various factors, such as olfactory testing method, disease type, and follow-up length, on the outcome, subgroup analyses were conducted. In addition, the influence analysis of the comparison between MTP and partial MTR was carried out by omitting 1 included study at a time. After a full-text review, we conducted a sensitivity analysis by excluding studies with a high risk of bias and re-evaluating the results to validate the robustness of our findings.24,25 The models for all outcomes were assessed considering an alpha value of .05 and a power of 80%. All meta-analytical computation was conducted using the Comprehensive Meta-Analysis software (CMA version 3.0; Biostat, Inc., Englewood, NJ, USA) 26 and the R statistical software version 4.3.2 (R Project for Statistical Computing; The R Foundation for Statistical Computing, Vienna, Austria) in RStudio statistical software version 1.3.959 (RStudio; Posit, PBC (formerly RStudio, PBC), Boston, MA, USA)
Results
Study Identification and Selection
The initial search yielded 773 records, but after eliminating duplicates and reviewing titles and abstracts, only 12 studies were considered for full-text review. Five of those 12 studies were excluded because they did not meet the eligibility criteria (N = 4) or contained unsuitable data (N = 1). Therefore, the final analysis included 7 eligible studies (Figure 1). 27

PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study Characteristics
A total of 788 patients were allocated to the partial MTR group or the MTP group during rhinology and skull base surgery. Three of the studies included enrolled patients who underwent EEA,24,28,29 while another 4 recruited patients who underwent FESS.25,30-32 Five studies evaluated the olfactory outcome with objective tests,24,28,29,31,32 and the other 2 studies assessed the olfactory outcome with subjective questionnaires.25,30 Detailed information is presented in Table 1.
Study Characteristics.

Abbreviations: ADSS, Adelaide Disease Severity Score; CCCRC, Connecticut Chemosensory Clinical Research Center; CRS, chronic rhinosinusitis; CRSsNP, chronic rhinosinusitis without nasal polyposis; CRSwNP, chronic rhinosinusitis with nasal polyps; CSF, cerebrospinal fluid; EEA, endonasal endoscopic approach; FESS, functional endoscopic sinus surgery; MTP, middle turbinate preservation; MTR, middle turbinate resection; NSF, nasoseptal flap; OP, operation; SNOT-22, Sino-Nasal Outcome Test; UPSIT, University of Pennsylvania Smell Identification Test.
Risk of Bias Assessment and Evidence Evaluation
In the evaluation of the risk of bias, the ROBINS-I assessment indicates that 3 studies had a moderate overall risk of bias, with issues primarily related to confounding, participant selection, and, in some cases, classification of interventions or deviations from intended interventions.28,31,32 Two studies were classified as having a serious overall risk of bias, with significant concerns in participant selection, missing data, and measurement of outcomes.24,25 Common sources of bias across the studies included confounding and participant selection in non-randomized designs, as well as missing data and measurement biases in studies with higher levels of risk. The RoB 2 assessment identified varying levels of bias across the included randomized controlled trials. One study was categorized as having “some concerns” for overall bias, with specific concerns arising from the randomization process and handling of missing data, while other domains showed a low risk of bias. 29 Another study demonstrated a low risk of bias across all domains, including the randomization process, deviations from intended interventions, missing data, measurement of outcomes, and selection of reported results. 30 Overall, 1 study was rated with low bias, and the other with some concerns. As for the GRADE assessment, a few studies provide high-certainty evidence due to their robust randomized controlled trial designs, low risk of bias, consistent findings, direct relevance to the research question, and strong precision supported by adequate sample sizes. These studies strongly support the conclusion that MTR does not significantly affect olfactory function.29-31 Several studies offer moderate-certainty evidence, characterized by non-randomized designs with some concerns regarding bias, inconsistency, and imprecision. While these studies contribute valuable data, their limitations reduce the overall reliability of their conclusions.25,28,32 One study provides low-certainty evidence, with significant limitations in bias, inconsistency, and imprecision, making it less reliable for drawing robust conclusions. 24 Overall, the evidence consistently suggests that MTR does not result in significant long-term olfactory impairment, with the strongest support derived from high-quality randomized studies. The detailed assessment is presented in Table 2 and Figures S1 and S2; Tables S2 and S3.
Summary of Findings and GRADE Assessment Table.
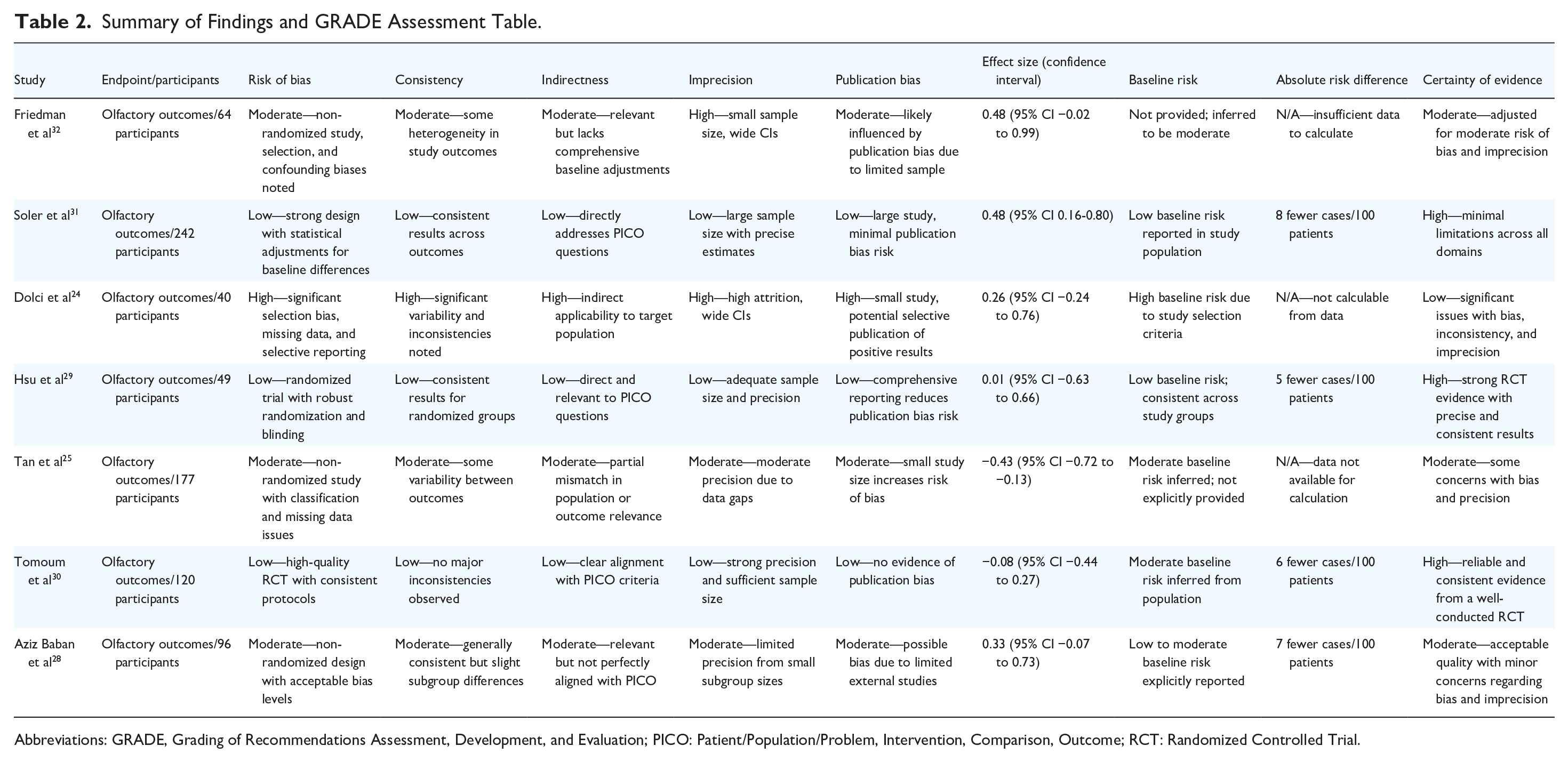
Abbreviations: GRADE, Grading of Recommendations Assessment, Development, and Evaluation; PICO: Patient/Population/Problem, Intervention, Comparison, Outcome; RCT: Randomized Controlled Trial.
Outcomes
The overall effect of the comparison between MTP and MTR
Seven studies compared olfactory function between the MTR and MTP groups. Consequently, the pooled effect estimate demonstrated a nonsignificant difference24,25,28-32 [standardized mean difference (SMD), 0.140; 95% CI, −0.159 to 0.438; P = .359; I2 <1%] (Figure 2).

Overall effect of the comparison between MTP and MTR. MTP, middle turbinate preservation; MTR, middle turbinate resection; SMD, standardized mean difference; CI, confidence interval; IV, inverse variance.
Subgroup analysis by the olfactory test method
Subgroup analysis was performed according to the method of the olfactory test. Five included studies enrolled patients who evaluated olfactory function with objective tests, and the pooled results showed significantly better olfactory outcomes in patients who underwent MTR than in those who preserved MT24,28,29,31,32 (mean, 0.370; 95% CI, 0.17-0.56; P < .001; I2 = 0%). Two other included studies enrolled patients who evaluated olfactory function with subjective tests, and the pooled result showed no significant difference between the MTP and MTR groups25,30 (SMD, −0.271; 95% CI, −0.604 to 0.63; P = .112; I2 <1%; Figure 3).

Subgroup analysis by the olfactory test method. SMD, standardized mean difference; CI, confidence interval; IV, inverse variance.
Subgroup analysis by surgery type
Four studies included patients with chronic rhinosinusitis (CRS) who underwent FESS, and the pooled results showed no significant difference between the MTP and MTR groups25,30-32 (0.10; 95% CI, −0.35 to 0.54; P = .67; I2 = 85%; Figure 3). In addition, 3 studies included patients with skull base disease who underwent surgery via an EEA, and the pooled results also showed no significant difference between the MTP and MTR groups24,28,29 (SMD, 0.25; 95% CI, −0.04 to 0.53; P = .09; I2 = 0%; Figure 4).

Subgroup analysis by surgery type. SMD, standardized mean difference; CI, confidence interval; IV, inverse variance.
Subgroup analysis by follow-up length
Six studies included patients whose olfactory function was checked more than 6 months after surgery, and the pooled results showed no significant difference between the MTP and MTR groups24,25,28-31 (SMD, 0.09; 95% CI, −0.21 to 0.39; P = .57; I2 = 75%). One study included patients whose olfactory function was checked <6 months after surgery, and the pooled results also revealed no significant difference between the MTP and MTR groups 32 (SMD, 0.484; 95% CI, −0.022 to 0.99; P = .061; I2 = 0%; Figure 5).

Subgroup analysis by follow-up length. SMD, standardized mean difference; CI, confidence interval; IV, inverse variance.
Influence analysis
The influence analysis was conducted by systematically removing each study and observing the effect on the pooled point estimates. The results showed that the 95% confidence intervals of the overall pooled results for these outcomes still contained the estimates after excluding each study (Figure 6).

Influence analysis of the overall results. CI, confidence interval; IV, inverse variance; SMD, standardized mean difference.
Sensitivity analysis
We conducted a sensitivity analysis on the studies identified as having a higher risk of bias.24,25 After excluding these studies, we found that the statistical significance toward MTR (SMD, 0.26; 95% CI, 0.01-0.51; P = .04; I2 = 41.3%), which may suggest a potential underestimation of the benefits of MTR in the excluded 2 studies (Figure 7).
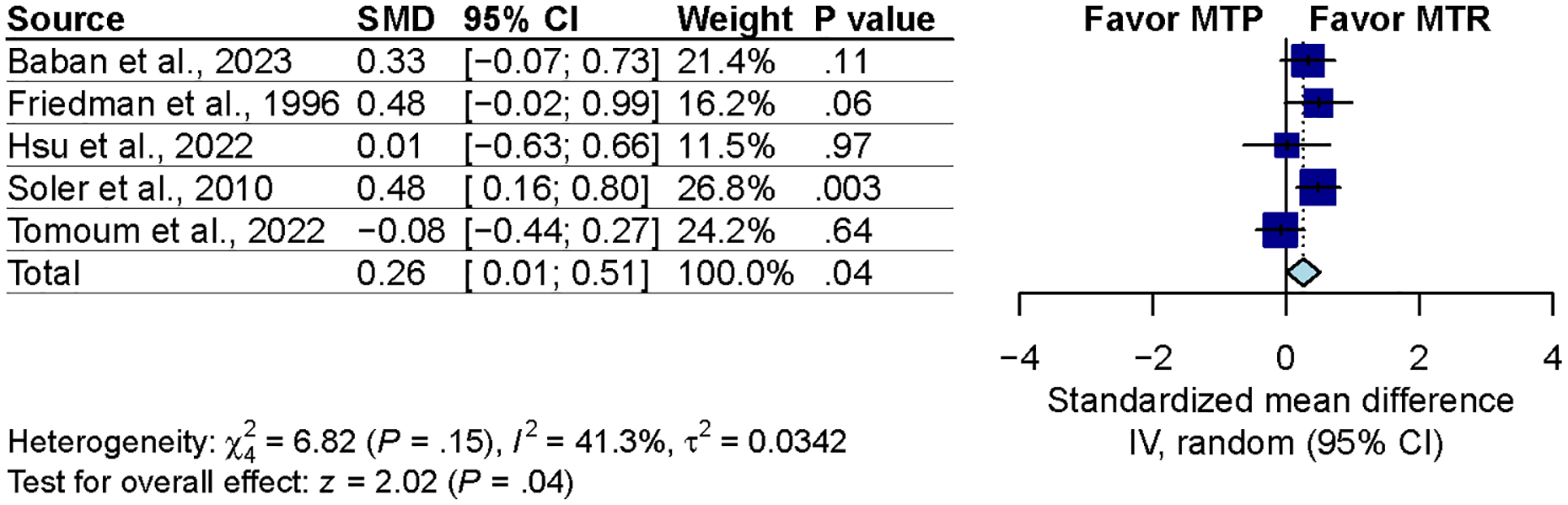
Sensitivity analysis excluding high risk of bias studies. SMD, standardized mean difference; CI, confidence interval; IV, inverse variance.
Discussion
The main finding of the present study was that partial MTR during endonasal surgery did not deteriorate olfactory function compared with MTP as the sensitivity analysis suggested a potential underestimation of MTR’s effect on olfactory function. Further subgroup analysis indicated that MTR even revealed better olfactory outcomes with objective tests. On the other hand, partial MTR in FESS for CRS or skull base lesions does not jeopardize olfactory function. In addition, the olfactory function of patients who were assessed 6 months after partial MTR was comparable to that of patients who underwent MTP.
Issues regarding partial MTR in patients who underwent endonasal endoscopic surgery have been discussed for decades. Those who support the MTP are concerned that overly aggressive removal may result in negative outcomes such as atrophic rhinitis, narrowing of the frontal sinus opening, and unnecessary elimination of a significant anatomical landmark.17,18 Nevertheless, in previous reviews33,34 of effects after partial MTR in endoscopic endonasal skull base surgery, the benefit of MTR compared to MTP in terms of patient outcomes remains controversial, with some studies reporting a positive impact while others finding no significant difference. However, no quantitative evidence is currently available. Therefore, we systematically examined all relevant studies and obtained quantitative results via meta-analysis. To the best of our knowledge, this meta-analysis represents the first comprehensive effort to evaluate the impact of partial MTR on olfactory function.
Subjective assessments of olfaction can be easily influenced by psychological factors, whereas objective olfactory thresholds may be affected by various factors, such as disease type or odor type.35-37 This well-known incongruence between subjective and objective olfactory assessments highlights a potential limitation in interpreting olfactory outcomes, as the results from 1 method may not fully align with the other. 37 Drawing upon our findings, we observed that MTR demonstrated better outcomes in objective olfactory assessments compared to other surgical approaches. While the exact mechanisms underlying this improvement remain unclear, 1 possibility is that MTR enhances airflow to the olfactory region, facilitating better odorant delivery to the olfactory epithelium.35,36,38 Another plausible explanation is that MTR improves inflammatory control and enhances medication delivery to the olfactory cleft, as suggested in prior studies. What we can confirm, however, is that MTR does not lead to olfactory deterioration. Previous studies have shown that the olfactory epithelium, which is distributed across the cribriform plate, the inner side of the ST, the upper part of the nasal septum, and the inner surface of the upper MT, 39 is not significantly affected by partial MTR. In addition, histological evidence indicating that the ST exhibits ~4-fold greater olfactory activity than the MT further supports the idea that partial resection of the MT does not impair olfactory function. 40 Although these results highlight that MTR not only preserves olfactory function but also may enhance it in objective assessments, further studies are needed to clarify the underlying mechanisms.
There has been intense debate regarding whether the EEA of skull base surgery impacts olfaction.41,42 Similar to the views held by those advocating for the preservation of the MT, experts who believe that EEA of skull base surgery could cause olfactory dysfunction argue that the surgery damages a significant number of olfactory nerves, especially when involving structures near the cribriform plate and sphenoid sinus, including the MT.43,44 However, previous evidence suggests that sellar and parasellar skull base surgery does not significantly increase the risk of olfactory loss.45-47 Similarly, our study revealed that partial removal of the MT during EEA skull base surgery does not increase the risk of olfactory loss.
Given the reliance on objective olfactory tests in this context, identification tests, such as the University of Pennsylvania Smell Identification Test,48-50 are commonly used in most postoperative evaluations. These tests primarily assess the ability to recognize and label odors, relying not only on olfactory function but also on cognitive factors such as memory and language. However, they do not capture other key aspects of olfactory function, such as threshold sensitivity and discrimination ability, which could provide a more comprehensive understanding of postoperative changes. 51 Yet, it is worth noting that specific surgical interventions in skull base surgery, such as ST resection, may have distinct effects on threshold sensitivity or retronasal olfaction. These dimensions, often overlooked in identification testing, warrant further investigation. Incorporating threshold and discrimination assessments into postoperative evaluations could provide a more holistic understanding of the mechanisms influencing olfactory outcomes and offer insights into the nuanced effects of surgical interventions. Future research in this area is crucial to enhance the comprehensiveness of olfactory evaluations.
Research indicates that ~16.8% to 27% of patients with posttraumatic olfactory dysfunction experience spontaneous recovery within the first 6 months due to the neuroplasticity of the olfactory system. 52 Other studies identified that the majority of clinically significant improvements in olfactory function occur within 3 to 6 months after trauma, making this early phase the most active period for potential recovery.51,53 By analyzing outcomes at 6 months, the present study aimed to exclude the effects of this spontaneous recovery phase to determine if MTR causes significant long-term damage to olfactory function. If MTR were truly detrimental, we would expect to observe a pronounced decline in olfactory outcomes in the subgroup with follow-ups longer than 6 months, while the subgroup with follow-ups shorter than 6 months would allow an evaluation of potential transient effects immediately post-surgery. However, the analysis found no significant differences in olfactory outcomes between the 2 follow-up subgroups, suggesting that MTR does not cause substantial olfactory damage in either the short or long term. It is important to note, however, that the subgroup with follow-ups shorter than 6 months included only 1 study, which limits the robustness of conclusions regarding short-term effects. While this analysis allows a confident conclusion that there is no difference between MTR and MTP in terms of long-term olfactory outcomes, further evidence is needed to better understand the potential short-term impact of MTR.
Proponents of MTR assert that removing the partial MT expands the surgical field. This is especially important for critical surgery involving vital organs (ie, the skull base). Alfieri and Jho 14 have conducted cadaveric studies to investigate various approaches to accessing the sphenoid sinus through the ethmoid sinuses during endoscopic surgery. They found that routes involving MTR are advantageous for accessing the lateral wall of the sphenoid sinus. The combined approach of MTR and middle antrostomy helps to enlarge the surgical space. 14 In addition, some proponents stated that diseased MTs could act as a nidus for the recurrence of sinusitis and nasal polyps along with synechiae formation or closure of the antrostomy, suggesting that MTR is essential.17,54-56 In the present study, the findings suggest that partial MTR during FESS or EEA surgery does not have a negative impact on patients’ subjective olfactory perception. Given the potential benefits, partial MTR should be considered in such surgical interventions.
The current study was subject to several limitations. First, the small number of included studies (n = 7) restricts the generalizability of the results. Moreover, the method of MTR is influenced by regional, hospital, and individual physician preferences, leading to variations in the procedure that could contribute to some degree of heterogeneity. In addition, factors such as age, sex, race, and disease type (eg, CRS with or without polyposis) might influence postsurgical olfactory recovery, introducing further heterogeneity. These variables were not fully presented in the articles, and some variables required meta-regression analysis (eg, age). According to the Cochrane Handbook for Systematic Reviews of Interventions, 57 a total of 10 studies are recommended for meta-regression to explore heterogeneity with sufficient accuracy. Given the potential for heterogeneity, this article employed a random-effects model to address heterogeneity that may not be quantifiable. Despite the efforts made through statistical methodologies to account for these variations, they cannot eliminate the potential biases and inconsistencies introduced by such heterogeneity. This limitation should be considered when interpreting the findings and their applicability to broader clinical contexts. Second, most studies included in this review provided only postoperative data for analysis. While baseline measurements were confirmed to show no significant differences between groups, relying solely on post-intervention data limits the ability to evaluate the actual magnitude of change in outcomes. Third, the comparison between MTR and MTP encompasses more outcomes than just olfaction, such as synechiae and disease recurrence rate. Unfortunately, the articles included in this study were unable to compare these outcomes, and we look forward to future research providing further evidence on these aspects. Fourth, some studies employ different scales and methods for assessing olfaction, which may pose challenges in interpreting the results. In light of this, our research utilizes the SMD as a uniform measure for evaluation. Lastly, some studies included in this review were found to have a higher risk of bias during the appraisal process. Considering that these studies did not violate the inclusion criteria and given the scarcity of relevant studies on this topic, we decided not to exclude them. To assess whether the high risk of bias significantly impacted the original results and led to entirely different conclusions, we conducted a sensitivity analysis. The results indicated that studies with a high risk of bias tended to underestimate the potential benefits of MTR. However, this did not result in conclusions that were entirely contradictory to our earlier findings that MTR does not adversely affect olfactory function. On the contrary, the analysis provided additional evidence partially supporting the benefits of MTR.
Conclusions
This systematic review and meta-analysis delineated the olfactory outcomes of patients who underwent partial MTR and MTP. Our results demonstrated that MTR does not deteriorate olfactory function compared with MTP. Considering the potential benefit, partial MTR might be prioritized in clinical settings.
Supplemental Material
sj-docx-1-ohn-10.1177_19160216251351566 – Supplemental material for Partial Middle Turbinate Resection Versus Preservation on Olfactory Function: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-ohn-10.1177_19160216251351566 for Partial Middle Turbinate Resection Versus Preservation on Olfactory Function: A Systematic Review and Meta-Analysis by Yen-An Chen, Chih-Hao Chen, Wei-Hsin Wang and Ming-Ying Lan in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Author Contributions
The leading author (Y.-A. C.), the second author (C.-H.C.), and the senior author (M.-Y.L.) had comprehensive access to the study’s data and bear responsibility for both the data’s integrity and the precision of its analysis. Concept and design: all authors. Acquisition, analysis, or interpretation of data: Y.-A.C., C.-H.C., M.-Y.L. Drafting of the manuscript: Y.-A.C., C.-H.C., M.-Y.L. Critical revision of the manuscript for important intellectual content: W.-H.W., M.-Y.L. Statistical analysis: Y.-A.C., C.-H.C. Obtained funding: M.-Y.L. Administrative, technical, or material support: M.-Y.L. Supervision: W.-H.W., M.-Y.L.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from Taipei Veterans General Hospital (V113C-100 and V114C-123) and the Ministry of Science and Technology (NSTC112-2314-B-075-008-MY3-1). The funders did not play any role in the study design, data collection, or analysis, decision to publish, or preparation of the manuscript.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.