
Abstract
Importance
Neck dissection is a common surgical treatment for patients with oral squamous cell carcinoma (OSCC). Due to the low incidence of level IIb metastases and the risk of injury to the spinal accessory nerve during level IIb dissection, the need for preventive neck dissection of this area has been discussed.
Objective
This study aimed to verify the incidence of level IIb metastases in patients with cN0 OSCC and to discuss the need for excision.
Design
Retrospective cohort study.
Setting
This study was conducted at 3 centers: the Department of Oral and Maxillofacial Surgical Oncology at the Institute of Science Tokyo Hospital, the Department of Oral and Maxillofacial Surgery at Kobe University Graduate School of Medicine, and the Department of Clinical Oral Oncology, Hokkaido Cancer Center.
Participants
In total, 222 patients with cN0 OSCC underwent supraomohyoid neck dissection (SOHND) between 2013 and 2021.
Main Outcome Measures
Incidence of level IIb metastases in patients with cN0 OSCC.
Results
Lymph node metastasis was confirmed in 57 patients (25.7%). Two patients (0.9%) had level IIb metastasis. The primary site in these cases was the tongue in 1 case and the lower gingiva in the other, both with advanced cT4 primary tumors. Isolated level IIb metastasis was observed in tongue OSCC samples. Both patients with level IIb metastases experienced primary recurrence. The 5 year overall survival rates for pN(−) and pN(+) patients were 80.6% and 74.3%, respectively (P = .229). The 5 year disease-specific survival rates for the pN(−) and pN(+) patients were 89.6% and 77.2%, respectively (P = .057).
Conclusions and Relevance
Level IIb lymph node involvement in clinical N0 neck cancers is rare. Thus, SOHND may be adequate for most patients with OSCC. Therefore, level IIb dissection may be omitted in patients with cN0 in early-stage OSCC.

Key Messages
Routine dissection of level IIb lymph nodes in clinically-node-negative oral squamous cell carcinoma is unnecessary due to the low incidence of metastasis, thus potentially reducing surgical morbidity and preserving patients’ quality of life.
Background
Squamous cell carcinoma is the most common malignant tumor of the oral cavity, accounting for the vast majority (~90%) of oral cancers. 1 Lymph node metastasis is an important prognostic factor of oral squamous cell carcinoma (OSCC). 2 Occult disease rates have been reported to range from 15% to 34%.3,4 In patients with early-stage OSCC, prompt treatment is recommended because delays in treatment after biopsy increase the incidence of local and cervical failure. 5 Neck dissection is a key component in OSCC treatment.
During surgical management of the neck, the type of neck dissection depends on the clinical status of the neck nodes. It consists of selective neck dissection (SND) for clinically–node-negative patients and modified radical neck dissection (MRND) for clinically-involved necks. 6 OSCC has the highest risk of spreading to level I-III neck nodes. Skip metastasis to level IV or V, in the absence of disease at levels I-III, is exceedingly rare. Therefore, supraomohyoid neck dissection (SOHND) is currently the most common surgical method for detecting occult metastatic cervical lymph nodes and treating N0 neck cancers. As level II is one of the most likely regions in which OSCC tends to metastasize, meticulous dissection is required in this area. 7 The upper internal jugular vein (IJV) and spinal accessory nerve (SAN) lymph nodes in the posterior region of level II are known as level IIb. 8 Complications that may occur during and after level IIb dissection include SAN dysfunction, which results in limitation of shoulder movements 9 and thus has a negative impact on quality of life. To overcome this complication, avoiding a level IIb dissection has been proposed. The frequency of metastasis to level IIb varies widely in the literature, ranging from 0% to 10.4%,10,11 and the question of whether level IIb should be resected remains unclear. Hence, the present study aimed to determine the prevalence of nodal metastasis at level IIb in patients with cN0 OSCC and assess the various clinicopathological factors that influence metastasis to determine whether level IIb lymph node dissection is unnecessary.
Materials and Methods
Between 2013 and 2021, 222 patients with OSCC were treated at 3 centers: the Department of Oral and Maxillofacial Surgical Oncology at the Institute of Science Tokyo Hospital in Tokyo, the Department of Oral and Maxillofacial Surgery at Kobe University Graduate School of Medicine in Kobe, and the Department of Clinical Oral Oncology, Hokkaido Cancer Center in Sapporo. Patients presenting with biopsy-proven squamous cell carcinoma of the oral cavity were included. The exclusion criteria were synchronous head and neck cancer, history of surgery or radiotherapy of the head and neck, history of head and neck cancer, and primary treatment with brachytherapy. All the patients underwent tumor resection and SOHND for elective neck dissection. If the tumor was located on or crossed the midline, a bilateral dissection was performed. After the dissection, all nodal stations were separately labeled as levels I-III, with the level II group being divided into IIa and IIb, and were to the Department of Pathology for the analysis of the permanent section.
All eligible patients underwent a detailed medical history, clinical examination, and routine blood investigations, including renal function tests. Various details such as tumor grade, Yamamoto-Kohama (YK) classification, 12 perineural and lymphovascular invasions, 13 total number of lymph nodes, number of involved lymph nodes, extranodal extension (ENE), and lymph node positivity were recorded. TNM staging was used to stage the tumors. All primary tumors and neck metastases were staged according to the eighth edition of the American Joint Committee on Cancer TNM staging system.
These included pathological investigations, such as biopsy, and radiological investigations, such as US, CT, MRI, and PET-CT. Postoperative treatment was performed in patients with positive margins, advanced primary tumors, ≥4 histological cervical lymph node metastases, or the presence of pathological ENE, which may cause dissemination to the surrounding tissues outside of the neck dissection area or distant organs. Either postoperative chemotherapy or radiotherapy (2.0 Gy/fraction, total 50-66 Gy) or both were administered to these patients with platinum-based anticancer agents administered concurrently, if possible. Older patients and those with renal dysfunction were administered S-1. The follow-up period was set from the date of treatment initiation to March 31, 2023, and the mean follow-up period was 47 months (range, 1-119 months). This study adhered to the principles of the Declaration of Helsinki on Medical Protocols and Ethics. The Institutional Review Board of the Institute of Science Tokyo Hospital approved this clinicopathological study. The requirement for written informed patient consent was waived owing to the retrospective nature of this study (approval no. D2022-062). Survival curves were estimated using the Kaplan-Meier method, and differences were examined using the log-rank test. All statistical analyses were performed using the R-3.5.3 statistical software (https://www.r-project.org/). Statistical significance was set at P < .05.
Results
Records from all 222 cases were suitable for analysis. Table 1 presents the clinical characteristics of the datasets.
Baseline Characteristics.

Abbreviations: ENE, extranodal extension; YK, Yamamoto-Kohama.
Of the 222 patients, 127 (57.2%) were male and 95 (42.8%) were female, with ages ranging from 21 to 93 years and a median age of 68.0 years. The number of early-stage (T1/T2) cases was 114, and the number of patients with advanced-stage (T3/T4) was 108, which were almost the same. Reconstruction with a vascularized free flap was performed in 210 (94.6%) patients. Bilateral neck dissections were performed in 15 patients. The mean nodal yield per neck dissection was 35.4 (range 10-77). Neck node specimens from 57 patients (25.7%) were N(+). No pathological metastatic lymph nodes were observed at the contralateral cervical level. An ENE was observed in 8 patients (14.0%). The distribution of primary cancer subsites and incidence rates of cervical nodal metastases with primary cancer subsites are shown in Table 2.
Patterns of Lymph Node Metastasis.
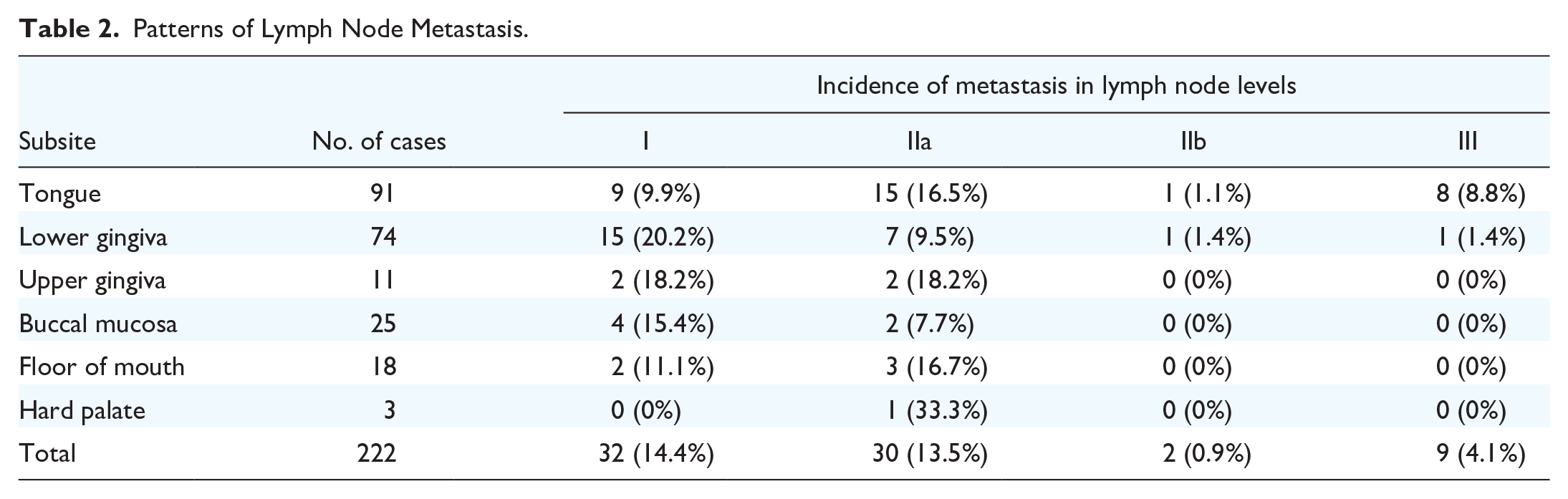
In our study, 25.7% of the patients had occult metastasis, with the tongue being the most common site (28.5%), followed by the floor of the mouth (27.8%), lower gingiva (24.3%), upper gingiva and hard palate (21.4%), and buccal mucosa (20.0%). Lymph node metastasis from OSCC was predominantly observed in levels I and IIa. Level III metastasis was observed in 9 patients, of which 4 had skip metastasis. Two patients (0.9%) had level IIb metastasis, and 1 had isolated metastasis. The primary site was the tongue in 1 case and the lower gingiva in 1 case. Table 3 lists positive IIb cases.
Summary of the Characteristics of Patients With Level IIb Metastases.
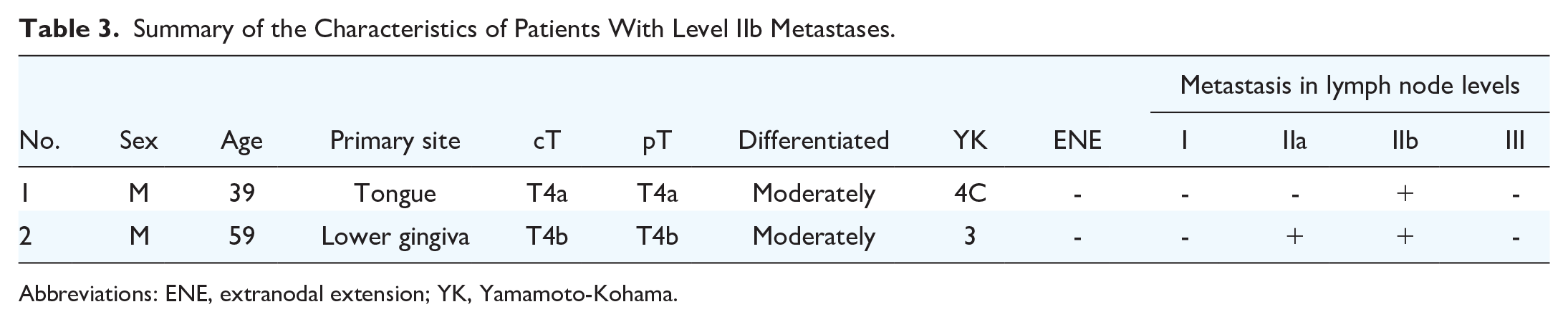
Abbreviations: ENE, extranodal extension; YK, Yamamoto-Kohama.
Two patients with level IIb metastases had advanced cT4 primary tumors. Postoperative adjuvant therapy was administered to 35 patients, 18 of whom had received chemoradiotherapy. Ten patients received chemotherapy, and 7 patients received radiotherapy. The recurrence patterns and details of the regional recurrence sites are summarized in Table 4.
Recurrence Pattern.
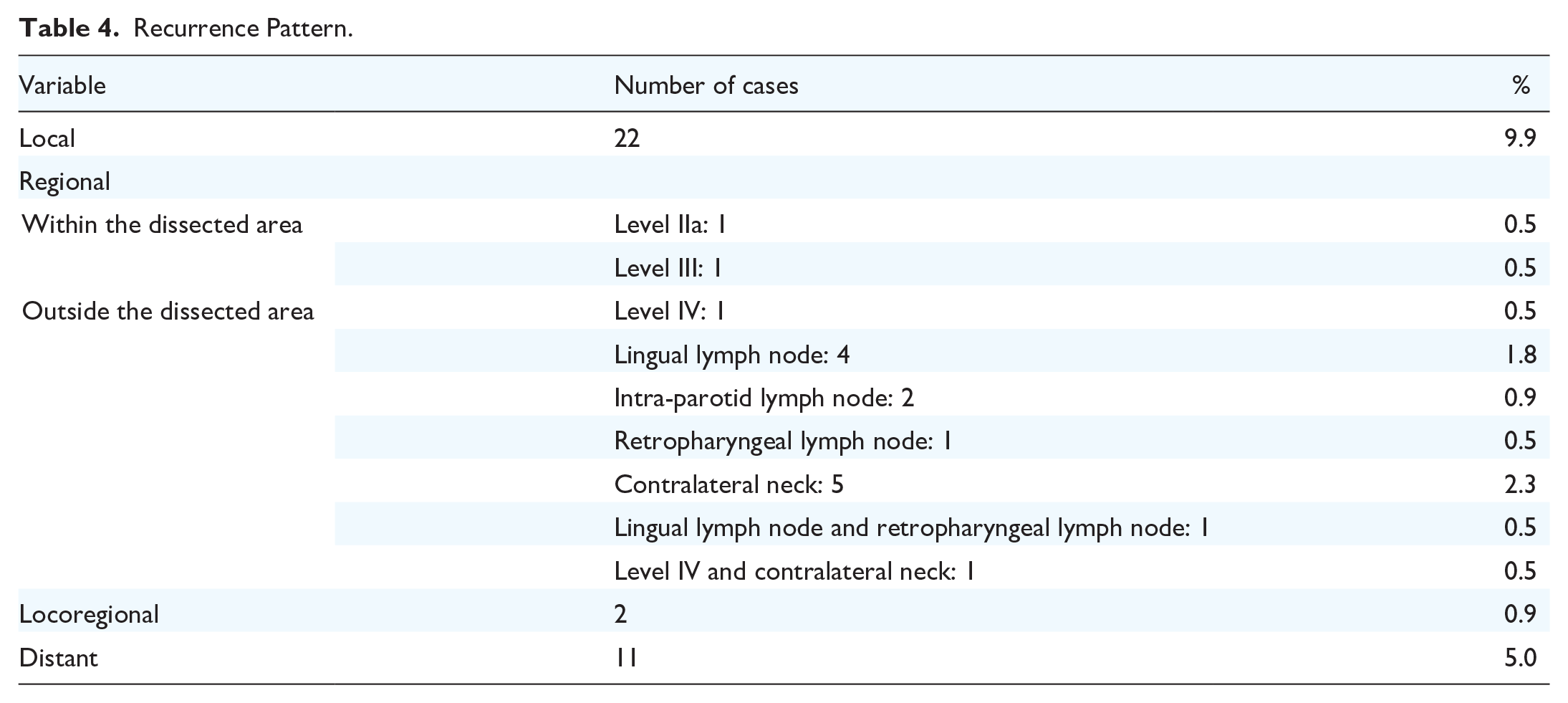
Twenty-two (9.9%) of 222 patients developed recurrence at the local primary site, and 17 (7.7%) developed regional recurrence. Of the 17 patients with regional recurrence, 15 were outside of the dissected area, and 2 were within the dissected area. Of the 2 patients with regional recurrence within the dissected area, 1 was at level IIa, and the other was at level III. Distant metastases were found in 11 patients (5.0%), 6 of whom achieved locoregional control. Both patients with level IIb metastases experienced primary recurrence. Analysis of the risk factors associated with level IIb metastasis in cN0 OSCC could not be performed because very few events occurred. The 5 year overall survival rates for pN(−) and pN(+) patients were 80.6% and 74.3%, respectively (P = .229; Figure 1A). The 5 year disease-specific survival rates for the pN(−) and pN(+) patients were 89.6% and 77.2%, respectively (P = .057; Figure 1B).
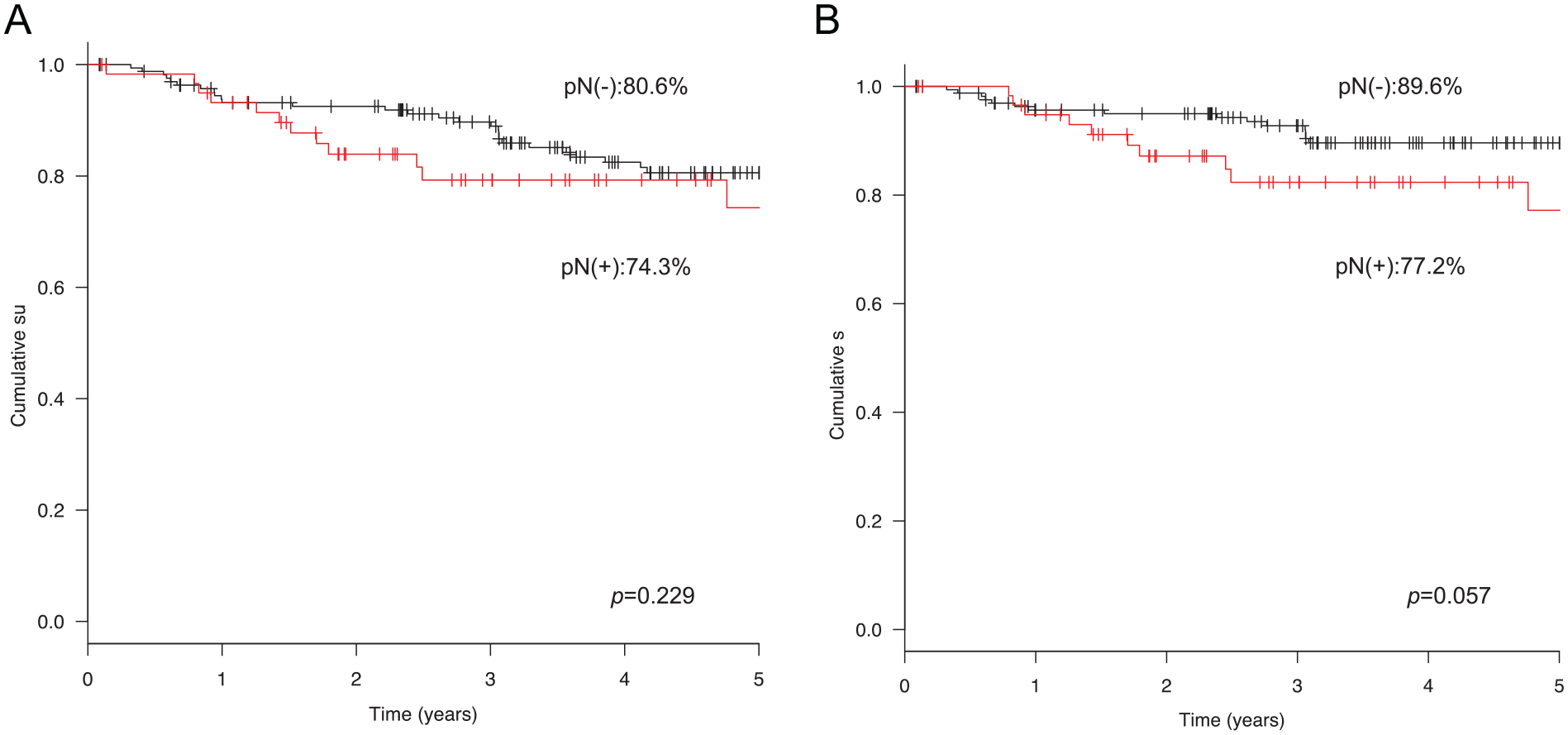
Kaplan-Meier estimates of overall survival (A) and disease-specific survival (B) in patients with cN0 OSCC based on lymph node metastasis.
Discussion
Neck dissection is a routine treatment for head and neck cancer because OSCC tends to metastasize to cervical lymph nodes via lymphatic vessels. Radical neck dissection (RND) was previously the standard treatment for lymph node metastases; however, it is associated with high morbidity. To reduce the morbidity associated with RND, many surgeons apply MRND and SND techniques to remove selected cervical lymph nodes while maintaining oncological safety. The goal of SND is to reduce morbidity by preserving the sternocleidomastoid muscles, the IJV, and the SAN. The SAN is important for supplying motor function to the trapezius muscle in most people, and the loss of this nerve causes significant shoulder dysfunction and pain. 9 This loss may be due to traction and elevation of the nerve during incision of the submuscular recess, that is, level IIb. Therefore, it is important to clarify whether cervical level IIb dissection should be performed to improve postoperative quality of life in patients with OSCC. Shoulder syndrome caused by RND was first described by Nahum et al. 14 Findings of this syndrome include shoulder pain, restricted abduction, a normal passive range of motion, pathoanatomical changes (shoulder drop, muscle atrophy, wing scapula), and abnormal electroneuromyographic changes. With SND, such as SOHND, shoulder dysfunction is observed in 21%-60% of cases at the expense of sparing the SAN. 15 Nerve function recovers approximately 3 months after surgery, 16 but axonal damage repair may take 12-18 months. The SAN has a variable course, particularly at its origin, and is adjacent to the IJV. Surgeons should familiarize themselves with common SAN variations to avoid nerve damage. 17 Manola et al 18 found that although the risk of metastasis at level IIb is generally low, it is statistically significant in cases of N(+) or when level IIa is involved. Furthermore, direct lymphatic drainage at level IIb has been demonstrated. 18 In this study, the level IIb metastasis in the patients with cN0 OSCC was 0.9%. Level IIb metastases are thought to be formed by retrograde lymph node flow, which results from obstruction by metastases to other lymphatic chains and insufficiency of the lymphatic vessel valves. Current literature clinically supports level IIb-sparing neck dissection in the N0 neck based on the fact that level IIb metastases are unlikely in the absence of level IIa and III involvement.19,20
The tongue is the most common primary site for OSCC. Some studies have reported no statistical significance for the primary site of level IIb metastases.21,22 In this study, we observed isolated metastases to level IIb in patients with OSCC of the tongue.
Maher et al recommended level IIB dissection for the treatment of OSCC in clinically-N0 patients. 23 There are many reasons why other researchers may be wary of omitting level IIb dissections. First, the uppermost lymph nodes of the spinal accessory lymph chain overlap with the uppermost lymph nodes of the internal jugular chain. 24 Second, many studies emphasizing oncological safety without dissecting level IIb appear to overlook the presence of micrometastases or isolated tumor cells in pN0 lymph nodes. In recent studies, the proportion of micrometastases in pN0 cases was as high as 9%, and the risk was highest at levels Ib and IIa. 25 Considering studies on nodal recurrence rates, recurrence at cervical level IIb may be very rare after conventional SOHND procedures in oral SCC. However, recurrence at level IIa or IIb cannot be distinguished. 26 In the hands of experienced head and neck surgeons, the rate of SAN injury is very low, and level IIB dissection might be relatively safe.
The low incidence of occult metastases up to level IIb compared with the high morbidity caused by SAN injury and associated shoulder dysfunction suggests that it may be better not to dissect this level. 27 However, awareness of recurrence, morbidity, and mortality may be higher in patients with recurrence who do not undergo level IIb neck dissection. Additionally, in patients with recurrence, re-excision of the neck may be difficult, resulting in greater damage to SANs.
This study has some limitations. First, this was a retrospective study. Second, the shoulder function was not evaluated. Further prospective study will be valuable in further defining the answer to this clinical question.
Conclusion
The incidence of level IIb lymph node metastasis in the N0 neck was 0.9%. SOHND may be adequate for most cases. Therefore, level IIb dissection may be omitted in patients with cN0 in early-stage OSCC.
Footnotes
Author Contributions
T.K. contributed to the study design, data collection, interpretation of results, and drafting of the manuscript. T.H. and T.N. contributed to the collection, interpretation of results, and drafting of the manuscript. M.A., M.U., and H.H. contributed to the interpretation of results and manuscript writing. All authors read and approved the final manuscript.
Data Availability Statement
Available on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Japanese Society of Oral and Maxillofacial Surgeons (JSOMS).
Ethics Approval and Consent to Participate
The present study was approved by the Institutional Review Board of the Institute of Science Tokyo Hospital (approval no. D2022-062).