
Abstract
Background
Choosing Wisely Canada recommends against the use of nasal bone X-rays for the evaluation of nasal fractures. The goal of this quality improvement project was to reduce the number of nasal bone X-rays ordered at our institution by 50% by 1 year.
Methods
The Institute for Healthcare Improvement Model for Improvement was used, and a pre- and post-intervention study was conducted. Change ideas included the following: a clinical decision support tool, provider surveys, and education. The number of X-rays ordered monthly was monitored. Financial cost (labor, materials, and overhead) was assessed. Environmental impact was extrapolated based on carbon dioxide equivalent emissions (CO2e). Balancing measures included the use of computed tomography (CT) scans. Analysis included summary statistics, statistical process control charting, and unpaired t-tests.
Results
There was a 73% reduction in total X-rays ordered from 197 pre-intervention (September 2021-November 2022) to 58 post-intervention (December 2022-February 2024). There was a statistically-significant decrease in difference of means of 2.6 X-rays/month (4.9 vs 2.3, pre vs post; P < .001), an average monthly reduction of 53%. There was special cause variation after implementation. Cost savings was $5534.98, and environmental footprint reduction was 111.2 kg of CO2e. There was no compensatory increase in the number of CT scans ordered.
Conclusion
Implementation of a clinical decision support tool and education resulted in a significant reduction in the number of nasal bone X-rays ordered for the evaluation of nasal fractures. This Choosing Wisely Canada project ultimately reduces unnecessary investigations for patients, saves health care costs, and reduces environmental impact.

Keywords
Introduction
Choosing Wisely Canada, a campaign focusing on reducing medically-unnecessary investigations and treatments, recommends against the use of plain film nasal bone X-rays for the evaluation of nasal fractures. This recommendation is listed in both Pediatric Otolaryngology and Rhinology Choosing Wisely statements. Nasal bone X-rays have a low sensitivity (64.9% ± 4.8%) and specificity (67.8% ± 4.7%) for identifying nasal fractures in both adult and pediatric populations. 1 Additionally, nasal bone X-rays do not change clinical management as physical examination is the gold standard for the clinical diagnosis of nasal fractures.1,2
The decision to perform a closed reduction in a nasal fracture depends on many factors. Important elements of the physical examination include the evaluation for nasal deformity or malposition, with palpation for local nasal tenderness with step-off and/or crepitus. 3 It is essential to assess for an associated septal hematoma, the identification of which would mandate urgent surgical intervention. Clinical examination may be hindered due to periorbital swelling or ecchymoses, epistaxis, or local nasal tenderness. However, the decision to perform a closed nasal reduction depends on the degree of external deformity, breathing difficulty, and patient preference, none of which are assessed by X-rays. 3 Nasal fracture reduction should ideally occur within 3 weeks, before nasal bones fixate.3,4
Despite the recommendations and evidence, many patients who are referred to Otolaryngology—Head and Neck Surgery (OHNS) with suspected nasal fractures have nasal bone X-rays. 5 In an American survey study with 140 otolaryngologist responses, it was found that 80% of consultations had imaging performed prior to consultation. 4 Specifically, 39% received nasal bone X-rays and 61% received computed tomography (CT) scans. Despite the prevalence of imaging prior to consultation for nasal fractures, 70% of practicing otolaryngologists reported imaging was “rarely” or “never” helpful in guiding management. 4 In incidents where multiple facial bone fractures are suspected, or there is a high velocity mechanism of trauma, CT imaging should be considered to guide management. 4 However, in isolated nasal trauma, neither CT imaging nor nasal bone X-rays are needed to support clinical decision-making. 3
The goal of this project was to reduce the number of unnecessary nasal bone X-rays ordered for the evaluation of nasal fractures at a Canadian academic health center for both pediatric and adult patients by over 50% over a 12 month period by September 2023. This article shares our quality improvement (QI) approach, results, and facilitators and barriers to success.
Methods
Problem Characterization
A root-cause analysis with the use of an Ishikawa fishbone diagram was performed to inform the reasons for ordering nasal bone X-rays at our institution (Figure 1). A driver diagram was used to demonstrate the relationships between the aim of the project, the key drivers that directly contribute to achieving our aim, and the secondary drivers with specific change ideas to test for each of the secondary drivers (Figure 2). Based on our driver diagram, change ideas included the following: (1) an electronic medical record (EMR) clinical decision support tool, (2) stakeholder surveys highlighting rationales and opinions regarding nasal bone X-ray use, and (3) education (infographics and resources).

Fishbone diagram.

Driver diagram.
Stakeholder Involvement
Stakeholder analysis included discussion and involvement from all relevant physicians and their associated departments, which included OHNS, with subspecialists in pediatric otolaryngology and rhinology, pediatric and adult emergency medicine (EM), radiology, plastic surgery, and oral and maxillofacial surgery. These were our main stakeholders as they were the providers ordering nasal bone X-rays, reading the X-rays, diagnosing nasal fractures, or being the consulting services to reduce nasal fractures.
Surveys were sent to EM physicians, as they are the stakeholders who most frequently order nasal bone X-rays, to understand the clinical rationale for ordering this investigation.
Project Design and Implementation Strategy
This project followed the Institute for Healthcare Improvement (IHI) Model for Improvement 6 (Table 1) with a plan-do-study-act (PDSA) cycle approach. After each PDSA cycle, the metrics were evaluated by the core project team, and subsequent PDSA cycles were informed by the previous cycles. A pre- and post-intervention study design was used. The pre-intervention group comprised data from the 15 months preceding the implementation of our change ideas (September 2021-November 2022). The post-intervention period included the 15 months following the implementation of the initial change ideas (December 2022-February 2024).
Institute for Healthcare Improvement’s Model for Improvement.

The first PDSA cycle included a clinical decision support tool and educational infographic (Figure 3). The second PDSA cycle included a follow-up survey of EM physicians and distribution of results with our peer-reviewed 1-page summary on recommendations for nasal bone fractures and management. 7

Educational infographic.
The clinical decision support tool is a modification of our institution’s EMR system wherein a notification pops up when a health care worker orders a nasal bone X-ray. The notification, which must be acknowledged prior to ordering the investigation, provides a summary of the Choosing Wisely Canada statements advising against the use of nasal bone X-rays for nasal fractures (Figure 4).

Clinical decision support tool.
Setting and Participants
This study was conducted at London Health Sciences Centre, an academic hospital system comprising 2 larger hospitals, and a pediatric hospital embedded within 1 of the 2 larger hospitals. This study received ethics exemption by the Research Ethics Board at Western University (London, Canada) for a QI study. The reporting of this manuscript is consistent with SQUIRE 2.0 guidelines. 8
Performance Measures and Evaluation
The primary measure was the number of nasal bone X-rays ordered monthly. These data were collected by the Decision Support team at our institution. Nasal bone X-rays that were ordered for an indication other than the evaluation of a possible nasal bone fracture (ie, rule out foreign body) were excluded. Statistical process control (SPC) charting was used for the analysis of monthly data to assess for special cause variation and therefore a shift in the center line. SPC charts were created and analyzed using QI Macros for Excel, version 2022.07 (KnowWare International Inc., Denver, CO, USA). Unpaired t-tests were conducted for the pre- and post-intervention analyses with a level of significance of P < .05. T-test analysis was performed using SPSS, version 29.0 (IBM Corp., Armonk, NY). Secondary outcome measures included case costing and greenhouse gas emissions. Cost was calculated from Decision Support data and consisted of labor, material, and overhead costs associated with ordering a nasal bone X-ray. Greenhouse gas emission calculations were an extrapolation of carbon dioxide equivalent emissions (CO2e) from chest X-rays based on a life cycle analysis by McAlister et al that took into consideration electricity, consumables, and associated waste. 9 Our balancing measures of potential compensatory increase in CT scans were assessed monthly, and EM provider burden was assessed by survey. Descriptive statistics were used for the analysis of survey data.
A timeline summary of all interventions and PDSA cycles is illustrated in Figure 5. Pre- and post-intervention time periods were determined by the start of our data analysis and the implementation of our PDSA cycle 1. To keep the pre- and post-intervention study periods even, 15 months were used.

Timeline of change ideas and PDSA cycles.
Results
Baseline Data and Baseline Survey Results
Based on our problem characterization and data from Decision Support, the majority of nasal bone X-rays were ordered by EM physicians in both adult and pediatric emergency departments (ED). Based on the baseline data between September 2021 and August 2022, there were 60 nasal bone X-rays ordered and 46 (77%) of those were ordered within the ED (Table 2). Our baseline survey had 86 responses from EM physicians. Results showed that 27% of the EM physicians believed that patients with suspected nasal fractures required a nasal bone X-ray for evaluation. Sixteen percent also believed nasal bone X-rays would help guide management. Thirty-nine percent believed consulting services (either OHNS or plastic surgery) would require nasal bone X-ray imaging prior to referral. Thirty-one percent were unfamiliar with the Choosing Wisely Canada guidelines. Sixty-five percent agreed they would make suggested changes to investigations if an EMR clinical decision support tool appeared highlighting Choosing Wisely Canada guidelines (Figure 6).
Total Number of Nasal Bone Plain Film X-Rays Ordered at LHSC Between September 2021 and August 2022.


Initial survey results to emergency department physicians in adult and pediatric departments at LHSC.
Implementation of Change Ideas and Statistical Analysis
PDSA cycle 1 included 2 change ideas: (1) A clinical decision support tool (November 2022) and (2) an educational infographic poster distributed to the EM physicians via e-mail and physically posted in high-traffic areas within EDs (December 2022). There was a 73% reduction in total X-rays ordered from 197 pre-intervention (September 2021-November 2022) to 58 post-intervention (December 2022-February 2024). A t-test comparing the monthly mean number of nasal bone X-rays ordered pre- versus post-implementation of PDSA cycle 1 demonstrated a significant decrease in the difference of means from 4.9 to 2.3, or a reduction of 2.60 ± 2.02 X-rays/month (P < .001; Figure 7). After PDSA cycle 1, SPC chart analysis showed special cause variation with a downward shift in the center line, which suggests a statistically-significant reduction in the number of nasal bone X-rays ordered monthly over the study period (Figure 8).

T-test analysis of nasal bone X-rays ordered from December 2021 to September 2022 compared with those from December 2022 to September 2023.
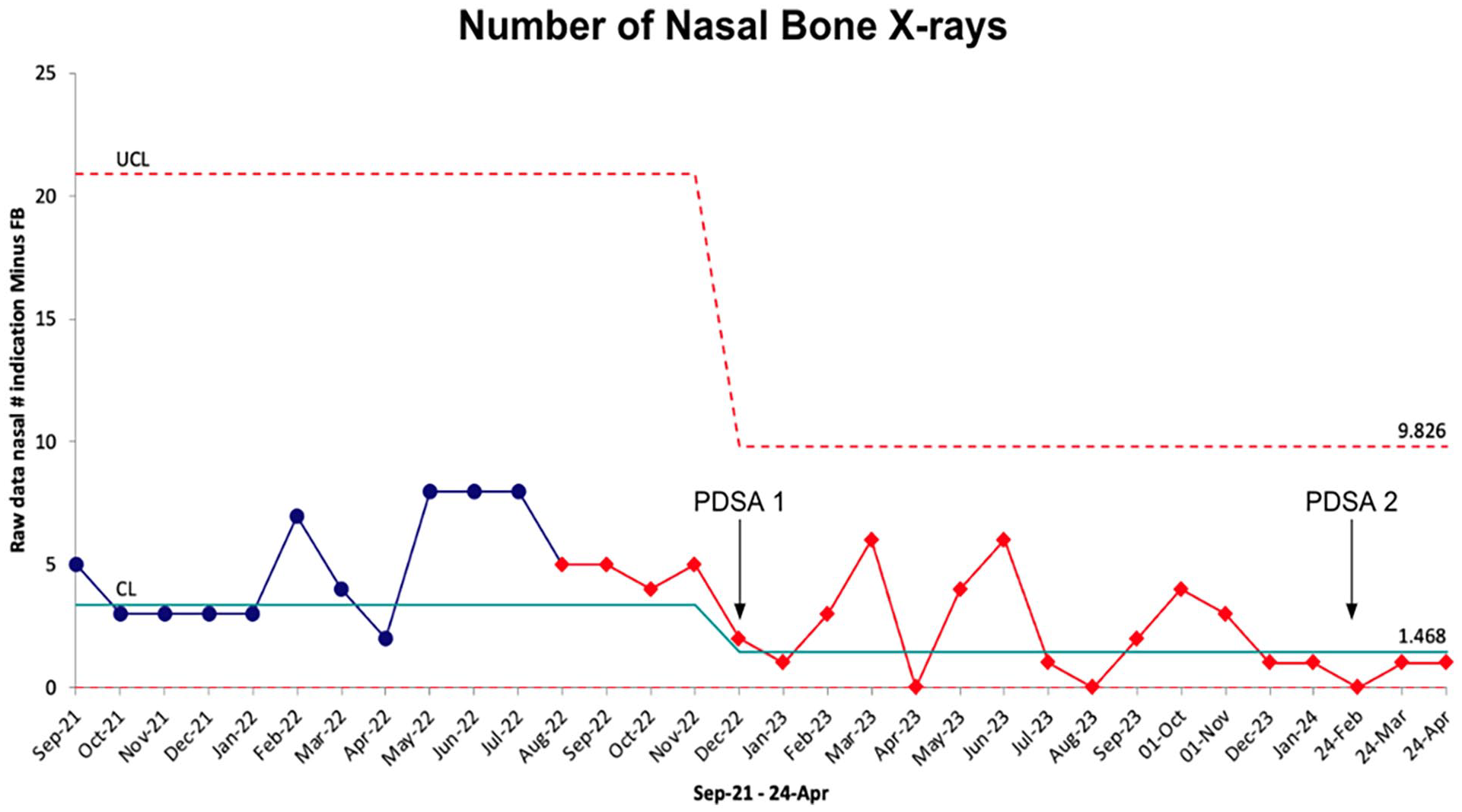
Pre- and post-intervention analysis between September 2021 and April 2024.
PDSA cycle 2 began in February of 2024. This included a follow-up survey to EM physicians along with distribution survey results, in addition to a peer-reviewed 1-page summary on nasal bone fracture management that the project team published in the Canadian Medical Association Journal. 7 There are only 2 additional data points since the implementation of PDSA cycle 2; therefore, further analysis could not yet be completed. However, only 1 nasal bone X-ray was ordered in each of these 2 months.
Follow-Up Survey Results
The same group of EM physicians were surveyed 1 year after the implementation of our change ideas. A total of 68 physicians responded to the survey. Thirty-five percent indicated they had ordered a nasal bone X-ray for concerns about a nasal fracture in the past 12 months. Only 16% indicated they noticed the clinical decision support tool on our EMR system when ordering a nasal bone X-ray, which may be attributable to the fact that physicians would only notice this if they placed an order for a nasal bone X-ray in the EMR. Only 2% indicated that the clinical decision support tool changed their final clinical decision to proceed with a nasal bone X-ray, while 28% indicated it did not change their decision. Eighty-four percent of respondents indicated that increased wait times in the ED and expectations from patients have negatively impacted their well-being. Forty-one percent indicated that nasal bone X-rays were ordered due to patient pressures, despite knowing it would not change their clinical management. Seventy-eight percent indicated that a patient handout highlighting why nasal bone X-rays are not indicated for isolated nasal fractures would be a resource they would be comfortable providing patients in lieu of ordering a nasal bone X-ray (Figure 9).
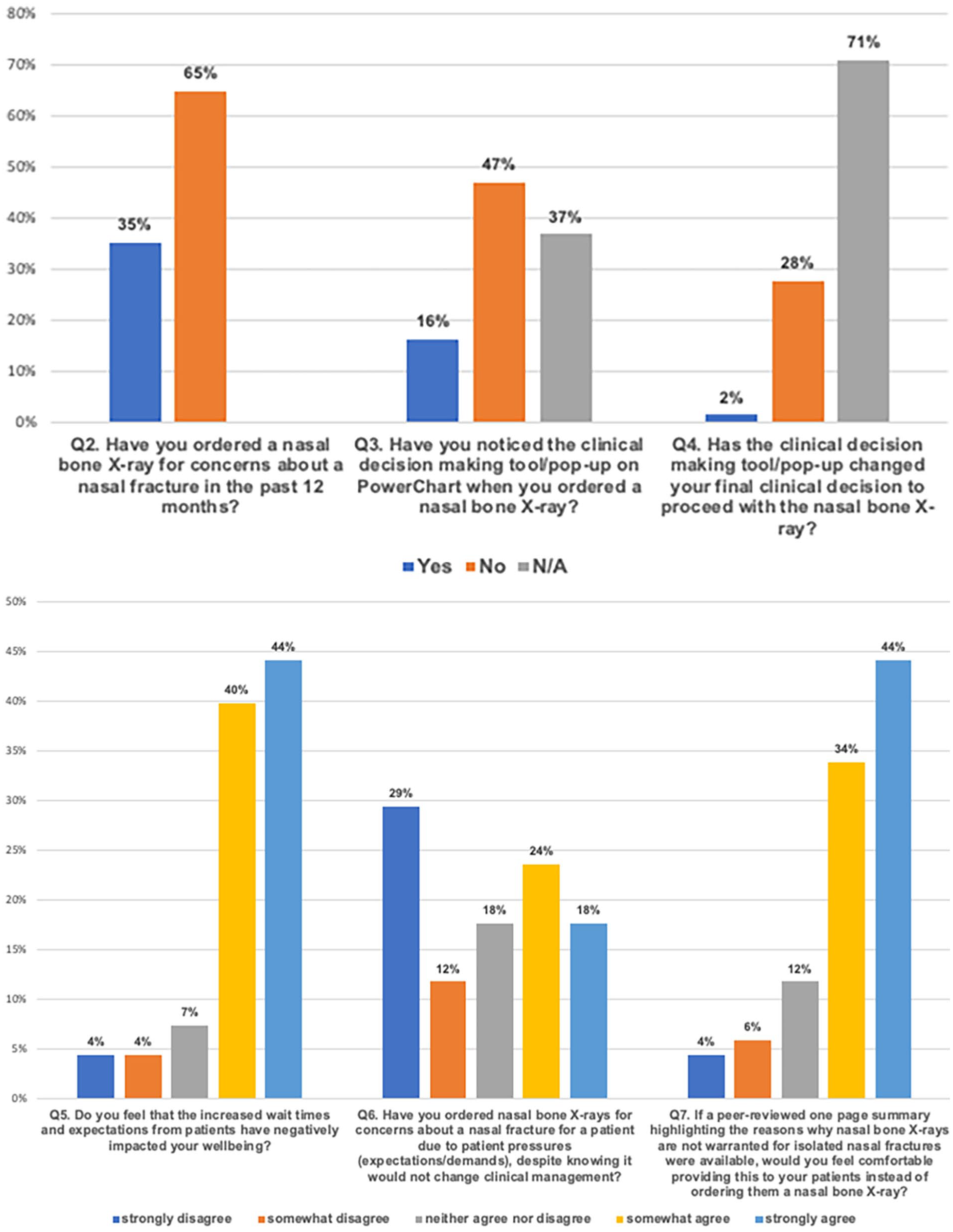
Final survey results to emergency department physicians in adult and pediatric departments at LHSC 1 year after the implementation of change ideas.
Secondary Outcome Measures
Our secondary outcome measures focused on cost analysis and carbon footprint calculations. Based on case costing data provided by Decision Support, the average cost of a single nasal bone X-ray was $39.82 ($19.55 for labor cost, $0.83 for material costs, and $19.44 for overhead). During the post-intervention period of 15 months, there was a cost savings of $5534.98. This was calculated by multiplying the cost of a single nasal bone X-ray ($39.82) by the difference in nasal bone X-rays ordered pre- and post-intervention (139).
Although the mean CO2e for nasal bone X-rays is not available in the published literature, a chest X-ray has a carbon footprint of 0.8 kg CO2e/scan. 9 Although a nasal bone X-ray is not the exact same as a chest X-ray, both are plain film X-rays and the life cycle analysis took into consideration the electricity, consumables, and waste generated, which are likely closely related between the 2 imaging modalities. 9 Extrapolating these results indicate that, during a 15 month post-intervention period, a reduction of 111.2 kg CO2e was likely achieved. This is equivalent to driving a new European car 921 km. 9
Balancing Measures
The balancing measures examined was the potential compensatory increase in CT scans for the evaluation of isolated nasal fractures and provider burden. There was no difference in CT scans ordered pre- and post-implementation of our change ideas. No CT scans were ordered for the sole purpose of assessing an isolated nasal bone fracture (Figure 10). As detailed in the follow-up survey results, EM physicians felt pressured by patients to order nasal bone X-rays despite knowing that it would not change the clinical management.

Balancing measures of facial/head CT scans ordered from September 2021 to April 2024.
Discussion
Choosing Wisely Canada is a national program that provides evidence-based recommendations with a goal of reducing unnecessary tests and treatments in Canada. The rationale behind this program is that unnecessary tests and treatments can expose patients to potential harm and consume precious health care resources. One such Otolaryngology-related Choosing Wisely Canada recommendation suggests that nasal bone X-rays are not indicated for the evaluation of suspected isolated nasal fractures due to low specificity and sensitivity. 1 Physical examination remains the gold standard for clinical diagnosis and management. 2
This QI project, which used a clinical decision support tool and education, resulted in a significant decrease in the number of nasal bone X-rays ordered per month, as demonstrated by both pre- and post-intervention t-test analysis and SPC chart analysis showing special cause variation. Although we were not able to meet our original goal of reducing nasal bone X-rays for the evaluation of nasal fractures by 50% in the first 12 months, we were able to meet this goal 3 months later. We also demonstrated significant financial cost and environmental savings. We saved $5534.98 and 111.2 kg in CO2e in a 15 month period. In a 10 year period, this would reflect $44,279.84 in savings and 889.6 kg in CO2e, which is the equivalent to driving a new European car 7368 km. Climate change is an increasingly-serious threat to human health. 10 Greenhouse gas emissions from health care are estimated to be 5% of net global emissions, whereas air travel is estimated to be 3.5%. 11 Therefore, as clinicians, we have a serious responsibility to champion resource stewardship and protect our planet and health.
Facilitators to the success of this project were understanding the problem and drivers of change. There was multidisciplinary stakeholder buy-in with champions in OHNS and adult and pediatric EM who led the project jointly. The rationale for choosing both the clinical decision support tool and education involved considering the hierarchy of effectiveness for QI interventions. The hierarchy of effectiveness builds from individual-focused interventions that are generally less effective to system-focused interventions that are often more effective: education and training, rules and policies, reminders and checklists, simplification and standardization, automation and computerization, and forcing functions. 12 Interventions toward the top of the hierarchy, such as automation and computerization, are more difficult to implement. The educational infographic targeted 3 levels of the hierarchy: education and training, rules and policies, and reminders and checklists. The clinical decision support tool focused on the second highest level of the hierarchy, automation, and computerization. Data that were readily available from Decision Support were also a key factor to the success of this project.
Other studies in the published literature have used clinical decision support tools with success. Chen et al implemented a clinical decision support tool in their EMR system to address imaging for the evaluation of acute low back pain in the ambulatory care setting. 13 They were able to demonstrate a significant decrease of 9.6% in total imaging, which included magnetic resonance imaging (MRI), CT scans, and X-rays. 13 There was a significant decrease in MRIs being ordered by 14.9%, equating to roughly $1.9 million saved. 13 However, the study also reported that the lower cost imaging modalities including CT and X-rays may have been favored over MRIs after the implementation of their clinical decision support tool. 13 A Choosing Wisely study by Gottheil et al implemented a clinical decision support tool in their EMR system with the aim of reducing inappropriate erythrocyte sedimentation rate (ESR) testing. 14 Their clinical decision support tool forced physicians to choose an appropriate indication before being able to order ESR testing. This resulted in a 40% reduction from 386 to 241 orders/week. 14 The authors reported that they did not have appropriate balancing measures but, perhaps looking into compensatory C-reactive protein levels, would have been useful. Our study was able to investigate the number of facial bone CT scans ordered as a balancing measure, which helps reinforce the true reduction and impact of our change ideas.
Although we were able to show a significant decrease in nasal bone X-rays ordered at our institution, this is a single-center study, and it remains to be shown whether it can be scaled on a broader level to other institutions. Cho et al were able to implement a similar clinical decision support tool in their health system which included 11 acute care facilities and 70 ambulatory centers with positive results. 15 However, a key advantage with their study was that all centers used the same EMR system, which is not the case for all centers and institutions across Ontario.
Barriers to success include the fact that we did not implement education with all stakeholders who may have been ordering nasal bone X-rays, and only focused on our EM colleagues who ordered the majority. However, the clinical decision support tool would pop up for any provider placing the order. Another limitation was the analysis of CO2e since we based our carbon footprint analysis on the Australian study by McAlister et al. 9 We made the assumption that similar electricity, consumables, and waste would be generated from 1 nasal bone X-ray as compared to 1 chest X-ray. Their average chest X-ray scan took 2 minutes, which is likely similar to the amount of time it would take to do a nasal bone X-ray. Further studies to determine the CO2e from nasal bone X-rays in the future, and preferably a Canadian context, may allow us to provide more accurate carbon footprint data estimations. Another limitation was the results of our second survey where only 16% of EM physicians noticed the clinical decision support tool. This is likely explained by the fact that many of the EM physicians did not order nasal bone X-rays during that period, thereby potentially not seeing the clinical decision support tool. Additionally, there may have been nonresponse bias from survey responders whereby those who may have ordered nasal bone X-rays may not have been interested in completing our survey. Only 2% of EM physicians indicated that the clinical decision support tool changed their final decision. This low percentage could be due to the known weakness and inadequacy of personal self-assessment in accurately evaluating performance.16,17 Therefore, it is possible that the tool did influence their final decisions, but this influence was not accurately reflected in their self-reports. Our survey results also showed that 41% of EM physicians felt long wait times and patient pressures forced them to order nasal bone X-rays despite knowing it would not change clinical management. This could also be an underlying reason why only 2% of EM physicians indicated that the clinical decision support tool changed their final decision. A final limitation to our study is that the case costing data from our Decision Support did not reflect the entire financial cost of ordering a nasal bone X-ray as it did not include the professional fee component from the Ontario fee schedule. Including the professional fee of $6.40, the total cost savings from our post-intervention 15 month period would have been $6424.58, reflecting an additional $889.60 saved.
The majority of EM physicians indicated that a patient handout highlighting why nasal bone X-rays are not indicated for isolated nasal fractures would be a resource they would be comfortable providing patients in lieu of ordering a nasal bone X-ray. As such, we are actively working with our Patient Experience team to provide a patient-targeted 1-page handout explaining why nasal bone X-rays are unnecessary for the management of nasal fractures.
We will continue to analyze our data for another year to evaluate the sustainability of our change ideas. Our clinical decision support tool is a permanent implementation at our institution, and if the data continue to reflect a meaningful and beneficial trend, we expect the changes to remain. Knowledge translation of study findings will allow for other institutions to implement similar clinical decision support tools and education.
Conclusion
The use of a clinical decision support tool alongside educational initiatives has demonstrated a significant reduction in nasal bone X-rays ordered for the evaluation of nasal fractures. This Choosing Wisely Canada QI project not only helps to streamline patient care by minimizing unnecessary investigations but also presents a tangible solution for reducing health care costs. By curbing the overutilization of diagnostic imaging, this approach demonstrates a commitment to environmental stewardship, ultimately contributing to a sustainable health care system.
Footnotes
Acknowledgements
Special thanks to Dr Ian Ross and Dr Scott McKillop from the Department of Radiology, Dr Michael Shimizu from the Department of Oral and Maxillofacial Surgery, Dr Kylen Van Osch and Dr Abrar Al Jassim from the Department of Otolaryngology—Head and Neck Surgery, and all physicians from London Health Sciences Centre in London, ON, Canada.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.