
Abstract
Importance
Postoperative hypocalcemia following total thyroidectomy (TT) can significantly affect patients’ quality of life. However, the most effective intraoperative interventions to mitigate this risk remain uncertain.
Objective
To assess the efficacy of parathyroid gland autotransplantation (PTA), near-infrared autofluorescence (NIRAF), and indocyanine green angiography (ICGA) in reducing postoperative hypocalcemia risk after TT.
Design
Meta-analysis.
Setting
This meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines, utilizing data from PubMed, Embase, and the Cochrane Library, with searches conducted through February 2024.
Participants
Patients undergoing TT with or without intraoperative interventions of PTA, NIRAF, ICGA, or a combined approach.
Interventions
PTA, NIRAF, ICGA, or a combination of these methods.
Main Outcome Measures
Incidence of postoperative transient and permanent hypocalcemia.
Results
From 582 identified records, 32 studies, including 13,299 TT patients (6386 with benign and 6913 with malignant conditions), met the inclusion criteria. PTA was associated with a higher incidence of transient postoperative hypocalcemia (OR = 1.98; 95% CI: 1.42-2.77; I2 = 84%). Conversely, NIRAF (OR = 0.45; 95% CI: 0.35-0.57; I2 = 0%) and ICGA (OR = 0.22; 95% CI: 0.07-0.69; I2 = 0%) showed reduced incidences of transient hypocalcemia. The combined NIRAF and ICGA approach, evaluated in 2 studies, yielded inconclusive results (OR = 0.62; 95% CI: 0.28-1.37).
Conclusions and Relevance
Intraoperative use of NIRAF and ICGA significantly decreased the incidence of transient hypocalcemia following TT, whereas PTA did not demonstrate similar efficacy. Minimal effects on permanent hypocalcemia were observed across interventions. Further research is necessary to clarify the effectiveness of the combined NIRAF and ICGA approach.

Keywords
Introduction
Hypocalcemia is the most common complication among patients who have undergone total thyroidectomy (TT), causing symptoms ranging from mild to severe or even prolonging hospitalization.1-3 A recent systematic review and meta-analysis found that transient hypocalcemia occurs in 19% to 38% of patients undergoing TT, with permanent hypocalcemia developing in 3% of these cases. 4 Initial symptomatic postoperative hypocalcemia is linked to a higher risk of persistent hypocalcemia. 5 The leading causes may be inadvertent injury to the parathyroid gland autotransplantations (PTAs) through devascularization or accidental resection. 4
Various strategies are implemented to mitigate the adverse effects caused by decreased serum calcium levels. Vitamin D, calcium supplements, or steroids are administered preoperatively or postoperatively.6-8 In addition to medical therapies, intraoperative interventions such as autotransplantation of the PTAs, imaging with near-infrared autofluorescence (NIRAF), or indocyanine green angiography (ICGA) are considered feasible for preventing postoperative hypocalcemia.
Identifying and preserving the PTAs are crucial for preventing postoperative hypocalcemia. PTA is a traditional method where the glands are removed and reimplanted beneath muscles, allowing them to adhere to host tissues and potentially restore function. 9 In contrast, NIRAF employs light emission to identify PTAs intraoperatively, helping distinguish healthy from diseased glands and preventing hypocalcemia. 10 ICG, an FDA-approved dye, enhances visualization by making tissues fluoresce, allowing surgeons to assess gland vascularization and perfusion, thus ensuring gland viability and reducing the risk of hypocalcemia after surgery. 11 All 3 techniques aim to prevent post-TT hypocalcemia by either preserving the function of the PTAs or ensuring their vascular supply during surgery.
Postoperative hypocalcemia remains a significant complication following TT, yet the literature presents inconsistent findings regarding the effectiveness of various intraoperative interventions. Wei et al 12 examined the effects of PTA in patients with carcinoma undergoing TT and central neck dissection (CND) and indicated that PTA reduces the incidence of permanent hypoparathyroidism, while others report no effect on the rates of postoperative hypocalcemia or hypoparathyroidism in a population of predominantly benign pathology undergoing TT. 13 NIRAF has been shown to decrease postoperative hypocalcemia but does not reduce hypocalcemia-related readmission rates. 14 ICGA aids in assessing parathyroid viability but may increase the rate of PTA during TT. 15 Since 2019, several reviews have explored the advantages and disadvantages of these interventions; however, they suffer from significant methodological limitations, such as incomplete study inclusion, limited quality assessment, and inclusion of other thyroid surgeries (eg, lobectomies, near-total thyroidectomies). This study aims to synthesize data from multiple studies focusing specifically on TT, providing a comprehensive evaluation of the impact of these interventions on both transient and permanent hypocalcemia rates.
Methods
Overview
The study employed a systematic review and meta-analysis following Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines, 16 searching Medline, Embase, and Cochrane databases up to February 2024. Eligible studies included randomized controlled trials (RCTs), cohort studies, and case–control studies involving adults undergoing TT. Data extraction focused on study design, patient demographics, surgical interventions, and hypocalcemia outcomes. Statistical analysis was performed using Review Manager (RevMan) version 5.4.1 (Cochrane, London, UK), calculating pooled odds ratios and mean differences (MDs) with a random-effects model. The risk of bias was assessed using the Newcastle-Ottawa Scale (NOS) 17 and Cochrane Risk of Bias tool 18 for included studies, ensuring methodological rigor and quality.
Search Strategy
This systematic review and meta-analysis was conducted in accordance with the PRISMA guidelines 16 and assessing the Methodological Quality of Systematic Reviews (AMSTAR) Guidelines. 19 The study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO). We systematically searched Medline via PubMed, Embase, and the Cochrane Database of Systematic Reviews without starting publication date restrictions through February 4, 2024. The keywords used were thyroidectomy, hypocalcemia, autotransplantation, autofluorescence, and indocyanine green (eTable 1 in Supplemental Material). No language restrictions were imposed during the initial search. We also searched the reference lists of all included articles and recent reviews on thyroidectomy, postoperative hypocalcemia, and its treatment to identify additional relevant articles. The institutional review board waived written informed consent because the study used previously published and deidentified data.
Study Selection
Eligible studies included original investigations that examined the association between the incidence of postoperative hypocalcemia and intraoperative interventions, including PTA, NIRAF, and ICG, among adult patients (aged ≥18 years) who underwent TT with or without CND and lateral neck dissection (LND). RCTs, cohort studies, case–control studies, and quasi-experimental studies were included. Studies exclusively reporting on patients younger than 18 years, undergoing surgeries other than TT (eg, lobectomy or hemithyroidectomy), or those that did not report the incidence of hypocalcemia were excluded. However, RCTs that reported only postoperative calcium levels were still included in calculating secondary outcome results. Two investigators (H.-W.H. and S.-H.H.) independently screened the remaining titles and abstracts of the articles for inclusion in the full-text review. In cases of disagreement about the selection of articles, the corresponding author (J.-W.C.) was consulted to make the final decision.
Data Extraction and Outcomes
Data of interest were subsequently extracted by consensus by 2 investigators (H.-W.H. and S.-H.H.). Conflicts were generally resolved through discussion. The corresponding author (J.-W.C.) would decide if a consensus still needed to be reached. Data extracted included reference details (author names and publication years), study design, baseline characteristics of the study population (number of patients in the study, ages, sex ratios, and confirmed pathologies), types of surgery, types of intraoperative interventions, definitions of hypocalcemia, numbers of patients with transient and permanent hypocalcemia, and follow-up times.
The primary outcomes of interest were the incidence of postoperative hypocalcemia after TT with various intraoperative interventions. The secondary outcomes included mean postoperative calcium levels. When both serum calcium and corrected serum calcium levels were available, the corrected levels were selected. Most articles defined hypocalcemia as a calcium level less than 8 mg/dL (or 2 mmol/L). However, to ensure the comprehensiveness of our study, we also included studies that defined hypocalcemia with other calcium levels or associated symptoms. Transient hypocalcemia, noted within 6 months postoperatively, was defined according to the first postoperative calcium profile selected for this study. Permanent hypocalcemia was defined as lasting 6 months or longer.
Risk of Bias
We assessed the quality of the included studies and evaluated the risk of bias using the NOS 17 for cohort studies and case–control studies, and Cochrane Risk of Bias tool 18 for RCTs. Studies achieving an overall score of 7 points were considered high quality. Two independent investigators (H.-W.H. and S.-H.H.) conducted the risk of bias assessments. Discrepancies in the results were resolved by consensus.
Statistical Analysis
This study used RevMan version 5.4.1 for data analysis, calculating pooled odds ratios, MDs, and 95% confidence intervals (CIs) with a random-effects model to produce forest plots for dichotomous and continuous outcomes. Heterogeneity was assessed using the Higgins I² statistic, 20 with I² values of 25%, 50%, and 75% representing low, moderate, and high heterogeneity, respectively. Mean calcium levels were evaluated with means and standard deviations; if unavailable, standard deviations were estimated from medians, ranges, and interquartile ranges following Wan et al 21 For studies with diverse designs, results were compared across all studies and restricted to RCTs and cohort studies. A 2-tailed P value of ≤.05 indicated statistical significance.
Results
Study Characteristics
A preliminary search identified 579 records. Duplicate assessment was performed both automatically and manually. We screened the reference lists, identifying and adding 3 studies. Titles and abstracts were reviewed against the inclusion criteria, resulting in 148 records eligible for full-text assessment. Of these, 116 were excluded for not meeting the inclusion criteria. Ultimately, 32 eligible studies were identified and independently reviewed, comprising 8 RCTs, 20 cohort studies, 3 case–control studies, and 1 quasi-experimental study (Figure 1).9,12,13,22-51

PRISMA flow diagram.
Table 1 summarizes the study design, patient population and characteristics, surgical techniques, pathology, intraoperative interventions, and follow-up time. The sample sizes of the studies varied from 58 to 2477. In total, 13,299 patients who underwent TT with or without CND, and LND were included in our study. Of these, 6386 patients (48.0%) were diagnosed with benign pathology, and 6913 patients (52.0%) were diagnosed with malignant pathology. These patients received one of the following interventions: PTA, NIRAF, ICGA, combined use of NIRAF and ICGA, or no intervention. The mean age ranged from 40.0 to 58.0 years, and the evaluation time ranged from 1 day postoperatively to 5 years.
Summary of Studies Included in the Meta-analysis of the Effect of Intraoperative Interventions on Hypocalcemia in Patients Undergoing Total Thyroidectomy.

Abbreviations: CND, central neck dissection; ICGA, indocyanine green angiography; LND, lateral neck dissection; NA, not applicable; NIRAF, near-infrared autofluorescence; PTA, parathyroid gland autotransplantation; TT, total thyroidectomy.
PTA Group
Fifteen studies investigated the PTA group compared with the control group,9,12,13,22-29,31,34,37,41,43 comprising 9183 patients. The PTA group included 4694 patients (51.1%), while the control group comprised 4489 patients (48.9%). The overall incidence of postoperative transient hypocalcemia was higher in the PTA group compared with the control group (953/2851, 33.4% vs 1104/3,855, 28.6%), with a pooled odds ratio of 1.98 (95% CI: 1.42-2.77) for the random-effects model (between-study heterogeneity, I2 = 84%; τ2 = 0.33; df = 13; Figure 2). The incidence of postoperative permanent hypocalcemia was similar between the 2 groups (49/2121, 2.3% vs 69/2227, 3.1%), with a pooled odds ratio of 1.20 (95% CI: 0.63-1.66) for the random-effects model (between-study heterogeneity, I2 = 29%; τ2 = 0.16; df = 9; Figure 3). Four studies compared the mean calcium level, with a MD of −0.08 mg/dL (95% CI: −0.14 to 0.01) for the random-effects model (between-study heterogeneity, I2 = 34%; τ2 = 0.00; df = 3; Figure 4).

Forest plots comparing incidence of posttotal thyroidectomy transient hypocalcemia between patients with and without intraoperative PTA, NIRAF, ICGA, and combined use of NIRAF and ICGA.
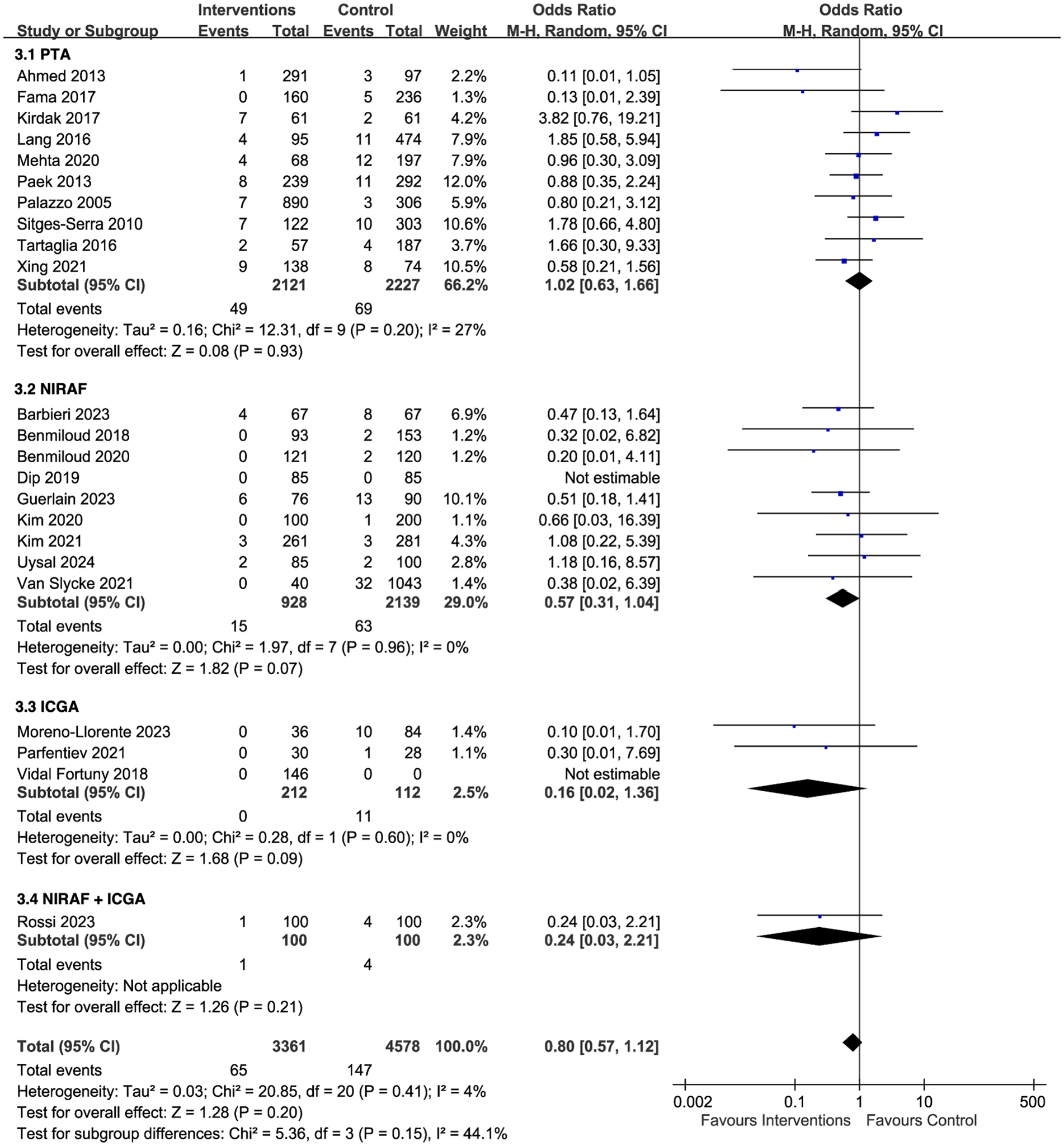
Forest plots comparing incidence of posttotal thyroidectomy permanent hypocalcemia between patients with and without intraoperative PTA, NIRAF, ICGA, and combined use of NIRAF and ICGA.

Forest Plots comparing posttotal thyroidectomy mean calcium levels between patients with and without intraoperative PTA, NIRAF, ICGA, and Combined Use of NIRAF and ICGA.
NIRAF Group
Twelve studies reported on the NIRAF group versus the control group,30,33,35,36,38,39,42,44-47,49 comprising of 3412 patients. The NIRAF group included 1099 patients (32.2%), while the control group included 2313 patients (67.8%). The overall incidence of postoperative transient hypocalcemia was lower in the NIRAF group compared with the control group (139/1099, 12.6% vs 601/2313, 26.0%), with a pooled odds ratio of 0.45 (95% CI: 0.35-0.57) for the random-effects model (between-study heterogeneity, I2 = 0%; τ2 = 0.00; df = 11; Figure 2). The incidence of postoperative permanent hypocalcemia was similar between the 2 groups (15/928, 1.6% vs 63/2139, 2.9%), with a pooled odds ratio of 0.57 (95% CI: 0.31-1.04) for the random-effects model (between-study heterogeneity, I2 = 0%; τ2 = 0.00; df = 7; Figure 3). Seven studies compared the mean calcium level, with a MD of 0.21 mg/dL (95% CI: 0.10-0.32) for the random-effects model (between-study heterogeneity, I2 = 76%; τ2 = 0.02; df = 6; Figure 4).
ICGA Group
Three studies compared the outcomes of the ICGA group and the control group,32,40,48 comprising a total of 324 patients. The ICGA group included 212 patients (65.4%), whereas the control group consisted of 112 patients (34.6%). The overall incidence of postoperative transient hypocalcemia was lower in the ICGA group compared with the control group (4/212, 1.9% vs 27/112, 24.1%), with a pooled odds ratio of 0.22 (95% CI: 0.07-0.69) for the random-effects model (between-study heterogeneity, I2 = 0%; τ2 = 0.00; df = 1; Figure 2). No patients in the ICGA group had permanent hypocalcemia, while the control group had an incidence of 9.8% (11/112). The pooled odds ratio was 0.16 (95% CI: 0.02-1.36) for the random-effects model (between-study heterogeneity, I2 = 0%; τ2 = 0.00; df = 1; Figure 3). Three studies compared the mean calcium level, with a MD of 0.19 mg/dL (95% CI: −0.19 to 0.57) for the random-effects model (between-study heterogeneity, I2 = 90%; τ2 = 0.07; df = 1; Figure 4).
NIRAF + ICGA Group
To precisely evaluate the effectiveness of the combined use of NIRAF and ICGA, we identified 2 articles for subgroup analysis.45,49 There was no significant difference in the mean calcium level between the combined NIRAF and ICGA group and control group, with a MD that was 0.25 mg/dL (95% CI: −0.03 to 0.54) for the random-effects model (between-study heterogeneity, I2 = 81%; τ2 = 0.03; df = 1; Figure 4). Only 1 article 50 discussed the incidence of transient (Figure 2) and permanent (Figure 3) hypocalcemia between the combined NIRAF and ICGA group and the control group. The result showed no significant differences between the 2 groups.
Subgroup Analysis
To address heterogeneity across study designs, we conducted subgroup analyses comparing all outcome measures from all designs with those from only RCTs and cohort studies. Results from RCTs and cohort studies were consistent with those from all designs (see eFigures 1-3 in Supplemental Material).
Quality Assessment
The risk of bias for included studies is detailed in eTable 2. Among 22 cohort studies, 13 had low bias risk (NOS scores 7-9), while 9 had moderate risk (NOS scores 4-6). All case-control studies, including 1 quasi-experimental study, were low-risk. Of the 8 RCTs, 3 were low-risk and 5 had some concerns. Publication bias was visually assessed using funnel plots (eFigures 4-6 in Supplemental Material).
Discussion
This systematic review and meta-analysis identified 32 eligible studies from an initial 582 records, comprising 13,299 patients undergoing TT. The quality assessment of the included studies indicated a low-to-moderate risk of bias. Compared with the control group, the PTA group showed a higher incidence of transient hypocalcemia with significant heterogeneity and a lower mean calcium level with moderate heterogeneity. The NIRAF and ICGA groups had a lower incidence of postoperative transient hypocalcemia with no heterogeneity. Moreover, the NIRAF group showed a higher mean calcium level than the control group, with significant heterogeneity. However, none of the intraoperative interventions significantly impacted the incidence of permanent hypocalcemia compared with no intervention. The combined effect of NIRAF and ICGA on the incidence of hypocalcemia was inconclusive.
The PTA, NIRAF, and ICGA techniques are all intraoperative procedures designed to enhance the surgeon’s ability to identify, assess, or preserve the PTAs in real time during thyroid surgery. Although these interventions are performed during surgery, each one has a distinct role, with PTA serving as a rescue measure for potentially compromised glands, while NIRAF and ICGA are used to protect and assess gland function. eTable 3 in Supplemental Material lists the purpose, mechanism, invasiveness, focused outcome, common use, and involved technology among these 3 intraoperative procedures.
Wang et al 52 synthesized the results of 25 articles investigating the effect of PTA on postoperative hypoparathyroidism. It concluded that PTA was associated with both transient and protracted hypoparathyroidism, defined as postoperative hypoparathyroidism lasting 1 and 6 months, respectively. Interestingly, the incidence of transient hypoparathyroidism was higher when 2 or more PTAs were autotransplanted than when 1 or no PTAs were autotransplanted. 52 Recently, fewer articles have focused on the effectiveness of PTA. By contrast, many studies have demonstrated that routine PTA in patients undergoing thyroid surgery may be a risk factor for transient hypocalcemia with even lower calcium levels.4,22,53 It is believed that it takes time for the ectopic PTAs to regain adequate function. Moreover, only a limited number of studies have shown a significant drop in the incidence of permanent hypocalcemia between patients with and without PTA. 24 Currently, PTA is mainly used as compensation when the PTAs are severely damaged during surgery. Our study demonstrated results similar to those of Wang’s study, 52 although we focused on calcium levels instead of parathyroid hormone (PTH) levels to investigate clinical correlations. Calcium levels are more straightforward and play a key role in clinical management. Although PTA has been widely used to preserve parathyroid function, it should be cautioned that the surgical technique itself may cause transient hypocalcemia.
Conversely, NIRAF has been shown to reduce the risk of post-TT hypocalcemia. Wang et al 54 performed a meta-analysis including 7 articles. NIRAF may help identify PTAs during thyroid surgery and assist in lowering the incidence of hypocalcemia at 1 day postoperatively. Still, it was not associated with a reduction at 6 months postoperatively. A meta-analysis performed by Weng et al 55 included patients undergoing TT without CND or LND in 6 articles. The study concluded that NIRAF is favorable for the 2180 participants regarding transient and permanent hypocalcemia. Another meta-analysis by Lu et al, 56 including 8 articles, also suggested that NIRAF had a beneficial effect on thyroid surgery by reducing the possibility of transient and permanent hypocalcemia. Barbieri et al 57 analyzed 13 articles and proved that NIRAF and ICG were effective in thyroid surgery. However, these studies included patients undergoing thyroidectomies other than TT, which might influence the actual effect of these intraoperative interventions. Recent meta-analyses58,59 of RCTs show that using NIRAF during TT significantly reduces postoperative hypocalcemia rates compared to non-NIRAF methods. However, results regarding permanent hypocalcemia and parathyroid dysfunction remain conflicting.
Compared with previous studies, our study focused on NIRAF and its clinical utilization to evaluate its effect more precisely on patients undergoing TT rather than lobectomy or near-TT. We did not exclude those with CND and LND, as comprehensive resection of the neck region may contribute to a higher risk of damage to the PTAs. Consistent with previous studies, we found NIRAF to be an efficient tool for patients undergoing TT to lower the possibility of postoperative transient hypocalcemia.
Though NIRAF shows a promise for the future due to its proven effectiveness, its sensitivity in detecting PTAs should also be considered. Ladurner et al 60 analyzed 205 PTAs from 117 patients and found that 179 glands (87.3%) showed a typical bluish-violet color. Lerchenberger et al 61 indicated that 64 of 78 PTAs from 50 patients showed the classic color, demonstrating a sensitivity of 82.0%. The higher sensitivity of NIRAF represents a greater chance of discovering PTAs, resulting in a lower likelihood of intraoperative damage.
ICGA was first described by Vidal Fortuny et al to assess the blood perfusion of PTAs. 62 According to Moreno-Llorente et al, the incidence of hypocalcemia was nearly 20% lower in patients with ICGA compared to those without ICGA (5.6% vs 26.2%). 48 Similarly, Parfentiev et al demonstrated a post-TT hypocalcemia incidence of 6.7% and 17.9% for those with and without ICG, respectively, on postoperative days 5 to 10. 40 Specifically, Vidal Fortuny et al 32 reported in a RCT that 146 out of 196 patients undergoing thyroid surgery who presented with at least 1 well-perfused PTA on ICG angiography had no incidence of hypocalcemia, in contrast to that 11 of the 50 patients who developed hypocalcemia when no PTA was identified during surgery. Currently, no synthesized data demonstrate the effect of ICGA on post-TT hypocalcemia. In our meta-analysis, the administration of ICG was associated with a lower incidence of postoperative transient hypocalcemia; however, there was no significant difference in mean calcium levels or the incidence of permanent hypocalcemia.
Since NIRAF provided solid evidence for improving post-TT calcium profile, we expected synergetic effects from the combination of NIRAF and ICGA. However, no significant improvement was observed in either the incidence of hypocalcemia or mean calcium levels.45,49 One study reported a notably higher serum PTH level in the intervention group compared to the control group (21.1 ± 16.0 pg/mL vs 15.0 ± 12.9 pg/mL). 49 A previous study introduced the concept of ICG score, which classified PTAs based on their vascularization. 62 At least 1 PTA with an ICG score of 2 could normalize PTH levels.48,62 At the same time, Rossi et al suggested that 2 or more PTAs with an ICG score of 2 provided a better prognostic index. 49 While ICGA shows promise in predicting PTA damage, conclusions about the combined use of NIRAF and ICGA are limited by the small number of studies and insufficient data. Further research is needed to assess their combined effectiveness.
Although these intraoperative techniques aim to reduce postoperative hypocalcemia, a surgeon's learning curve may also affect outcomes. Wang et al reported better perioperative results with increased experience,63,64 and Das et al highlighted the learning curve’s impact on thyroidectomy complications. 65 Overall, postoperative hypocalcemia can affect quality of life, extending hospital stays, requiring ongoing calcium supplementations, and risking permanent hypoparathyroidism. 66 Identifying interventions linked to lower hypocalcemia rates helps surgeons tailor strategies to reduce this complication. This study also offers evidence-based recommendations for intraoperative interventions, aiding the development of clinical guidelines for managing TT patients.
Limitations
This study has several limitations. First, the patient sample may not reflect typical thyroidectomy cases, as a higher proportion (52%) underwent surgery for cancer, which increases transient hypocalcemia risk, particularly with neck dissections during TT. 67 Demographics, surgical methods, approaches, and surgeon experience also impact hypocalcemia rates, but many studies lacked detailed data on these factors, complicating subgroup analysis. Second, varying definitions of hypocalcemia across studies prevented standardization of calcium cut-offs, potentially affecting incidence rates. Third, differences in postoperative calcium and vitamin D supplementation strategies, often involving calcium gluconate or calcitriol, limited therapeutic standardization. Fourth, this meta-analysis excludes techniques like activated carbon nanoparticle and methylene blue staining, which future research might explore for a broader perspective on intraoperative interventions. Diverse study designs may introduce heterogeneity and bias. Still, we believe including nonrandomized trials enriches our analysis and provides a more comprehensive understanding of the interventions’ effects while maintaining the robustness of our results. Notably, NIRAF and ICGA groups showed low I² values, reflecting similar methodologies and patient profiles, though a low I² suggests limited literature scope. Finally, most studies focused on short-term calcium levels; only 10 out of 32 tracked serum calcium for over 6 months, underscoring the need for further research on long-term hypocalcemia outcomes.
Conclusions
In patients undergoing TT with or without central or LND, PTA is associated with higher incidence of transient hypocalcemia and lower calcium level. NIRAF is associated with a lower incidence of transient hypocalcemia and higher calcium level. ICGA is associated with a lower incidence of transient hypocalcemia. The combined effect of NIRAF and ICGA warrants future investigation.
Supplemental Material
sj-doc-1-ohn-10.1177_19160216251333355 – Supplemental material for Impact of Intraoperative Interventions on Hypocalcemia Post-Total Thyroidectomy: A Meta-Analysis
Supplemental material, sj-doc-1-ohn-10.1177_19160216251333355 for Impact of Intraoperative Interventions on Hypocalcemia Post-Total Thyroidectomy: A Meta-Analysis by Hao-Wei Hsu, Sheng-Hsin Huang, Shao Huai Lee, Shih-Tsang Lin, Mingchih Chen, Ru-Yung Yang, Shyh-Dye Lee and Jeng-Wen Chen in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Author Contributions
Jeng-Wen Chen had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Hao-Wei Hsu: Study concept and design, data curation, interpretation of data, drafting of the manuscript. Sheng-Hsin Huang: Study concept and design, data curation, interpretation of data, drafting of the manuscript. Shao Huai Lee: Interpretation of data, critical revision of the manuscript for important intellectual content, administrative, study supervision. Shih-Tsang Lin: Interpretation of data, critical revision of the manuscript for important intellectual content, obtained funding, administrative, study supervision. Mingchih Chen: Critical revision of the manuscript for important intellectual content, administrative. Ru-Yung Yang: Critical revision of the manuscript for important intellectual content, administrative. Shyh-Dye Lee: Critical revision of the manuscript for important intellectual content, administrative. Jeng-Wen Chen: Study concept and design, data curation, analysis and interpretation of data, critical revision of the manuscript for important intellectual content, obtained funding, administrative, technical, or material support, study supervision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This study was supported by the National Science and Technology Council of the Republic of China (Taiwan) under grant NSTC 110-2511-H-567-001-MY2, NSTC 112-2410-H-567-001-MY3 and, in part, funded by Cardinal Tien Hospital under grant CTH113A-2202. This study was also supported by Cardinal Tien Junior College of Healthcare and Management under grant CTCN-109C-09. No additional external funding was received for this study.
Role of the Funder/Sponsor
The funders had no role in the design and conduct of the study; data collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.