
Abstract
Objective
Surgical training programs have a high prevalence of trainee stress and burnout. Formal mentorship programs (FMP) have been shown to alleviate these factors and improve quality of life (QOL) in short-term follow-up. This study aims to determine the long-term effects of an FMP on the well-being of a single-center cohort of surgical trainees.
Methods
A voluntary FMP was established at a surgical training program comprised 8 resident physicians. To quantitatively measure stress and burnout, the Perceived Stress Survey (PSS) and Maslach Burnout Inventory (MBI) were administered at baseline, 3, 6, 9, 12, 18, and 24 months. The World Health Quality of Life-Bref Questionnaire (WH-QOL) was administered at baseline, 12 and 24 months.
Results
Baseline levels of stress and burnout were high among all residents with an average PSS of 18.5 and MBI of 47.6, 50.6, and 16.5 for the emotional, depersonalization, and personal achievement domains respectively. After FMP implementation, PSS was reduced to 7.9 at 12 months (P = .001). These scores were sustained at 24 months (6.8, P = 1). MBI scores improved in emotional exhaustion (14.9, P < .0001), depersonalization (20.1, P < .0001), and personal achievement (40.1, P < .0001) at 12 months. All these benefits were sustained at 24 months. Baseline overall WH-QOL scores reflected low QOL (71.9). These significantly improved at 12 months (37.5, P = .002) with further improvement by 24 months (17.2, P = .03).
Conclusion
Long-term follow-up of a previously successful academic surgical FMP showed lasting improvements in stress, burnout, and overall QOL, despite new life challenges.

Introduction
Over time, increasing attention has been drawn to burnout among healthcare professionals. Burnout is defined by emotional exhaustion, depersonalization, and a low sense of personal accomplishment. 1 Burnout is particularly problematic in the realm of medicine as it leads to increased levels of stress and poor quality of life (QOL) within the healthcare professional, ultimately negatively impacting patient quality of care. Physicians experience a lack of motivation, less productivity, and more personal dysfunction, and as a result, residency education suffers. 1
Within surgical training programs, burnout has been described at various levels of tenure, from the resident trainee, 1 to the academic staff, 2 to even the chairs of programs. 3 In a recent study by Golub et al, 1 a large cross-sectional questionnaire of all US Otolaryngology-Head and Neck Surgery (OTO-HNS) residents revealed that 86% of trainees had either moderate or high levels of burnout. Stressors in order of decreasing frequency included insufficient time for exercise, little extracurricular time, difficulty eating healthily, low salary, and lack of sleep. 1 Needless to say, the high rates of burnout among residents and practicing physicians are alarming.
Given that the problem of physician burnout is so prevalent, attention must shift to implementing solutions to this problem. One proposed solution is mentorship.4,5 In fact, OTO-HNS residents describe mentorship as either important or critical to their learning. 6 In a survey of the Young Physicians Section, the greatest expressed need was for mentorship. 7 Despite this expressed need, a cross-sectional study looking at the prevalence of mentorship in OTO-HNS training programs in the United States found that the majority of such programs do not have a mentorship program in place. 6
We have previously found a high degree of baseline stress and burnout among residents in an academic surgical training program. After the implementation of a formal mentorship program (FMP) however, trainees experienced improvement in stress levels, burnout, and QOL. They captured the effects of this mentorship program for a duration of 1 year. 8 While the results of their study were promising, it raises the question of whether the benefits of mentorship continue to be sustained long-term, especially in light of the changing challenges that arise with personal life as well as shifting challenges as one progresses through residency training. More specifically, the long-term follow-up was meant to seek if there is sustaining of the program, its mentors, and benefits to its mentees over a longer period of time. The aims of this study were therefore to capture the long-term follow-up of a group of residents in an academic surgical training program undergoing an FMP.
Methods
Study Inclusion
This study was approved by the Health Research Ethics Board at the University of Alberta, prior to the introduction of the FMP. At the time of implementation, all post-graduate years (PGY) 1 to 4 as well as the academic staff of the OTO-HNS program at the University of Alberta were invited to participate. Participation and withdrawal from this study were completely voluntary. All staff and residents invited to participate in the program accepted, but since there were more staff than residents, not all staff served as mentors.
Pre-Intervention
Prior to the execution of the FMP, residents were meeting with their program director on a bi-annual basis. Further mentorship, whether that be formal or informal, was sought individually by each trainee. This process was neither required nor standardized.
Formal Mentorship Structure
With respect to the data included in this study, the FMP was initiated on July 1, 2015 and finished on June 30, 2017. A tiered mosaic model of mentorship was implemented (Figure 1). In this model, residents were assigned one main mentor (MM) who was to address a diverse realm of support including research, clinical and operative skills as well as personal development. In addition, residents were free to seek supplemental mentors (SM) who could provide expertise in a specific area depending on their academic interests or personal needs. Residents met with their MM monthly and with their SM as needed. Meetings could be formal or informal, and a variety of discussions, from career planning to personal well-being, were encouraged.

Tiered mosaic model of formal resident mentorship program.
Intake Form
Prospective mentors and mentees all filled out an intake form. This was meant to elucidate their personality, areas of expertise, and interest in the mentorship program. Data from this form was de-identified and utilized by the FMP committee (see below). The PGY2-4 residents chose their own mentors from a list provided to them, whereas the PGY1 residents were matched to a mentor, as guided by the intake form. This match was made utilizing each individual’s personality and academic interests. At the end of the trainee’s first year of residency, the mentorship relationship was terminated, and the resident was free to choose to continue mentorship with their previously assigned mentor or initiate a new MM relationship.
Governance
An FMP committee was established to direct the workings of the program. The FMP committee conducted annual evaluations of the MM to the mentee, during which they reviewed residents’ satisfaction with their mentor and their burnout and stress data. Should there be worsening or lack of improvement in stress or burnout scores, intervention was taken. The FMP committee also served to resolve any disputes among mentors and mentees. Overall, the committee upheld the goals and objectives of the program.
Outcomes
The primary outcome was the well-being of the trainee participating in the FMP as measured by validated questionnaires. The Maslach Burnout Inventory-Human Services (MBI), Perceived Stress Scale (PSS), and the World Health Organization Quality of Life – Bref (WHO-QOL) surveys were completed at baseline to assess residents’ levels of burnout, stress, and QOL. The MBI is a 22-item validated questionnaire that evaluates the main 3 domains of burnout: emotional exhaustion, depersonalization, and personal accomplishment. 9 The PSS is a validated 10-item questionnaire that evaluates stress levels. 10 The WH-QOL is a validated 26-item tool that measures overall QOL as broken down into 4 subdomains: physical health, psychological, social relationships, and environment. 11
The MBI and PSS were repeated at 3, 6, 9, 12, 18, and 24 months. The WHO-QOL survey was done at baseline, 12 and 24 months.
The secondary outcome was the overall satisfaction of residents toward the FMP as measured on a Likert-style satisfaction scale. This was measured at baseline, 12 and 24 months.
All residents kept their respective PGY years despite the time lapse within the paper. For example, PGY 1 residents were at the end of their PGY 2 year by the end of the 24-month survey point. To minimize the Hawthorne effect on study participants, residents were not informed of their scores on the aforementioned questionnaires.
Statistical Analysis
Descriptive statistics were used for residents’ parameters. Continuous data was expressed as means and analyzed using analysis of variance. Comparisons of proportions were performed using the Chi-squared test. Level significance was set as P < .05. Analyses were performed with SPSS Statistics 21.0 (SPSS Inc, Chicago, IL, USA).
Results
Participant Variables
There was a total of 8 residents that participated in this study (n = 5 males, n = 3 females). They were equally distributed between PGY 1-4 with 2 residents in each year (Table 1). The mean age was found to be 29.1 years (range 26-33). With respect to future career plans, 3 (37.5%) wished to pursue an academic practice and 50% of the residents wished to pursue fellowship training (Table 1).
Demographics of Participants.
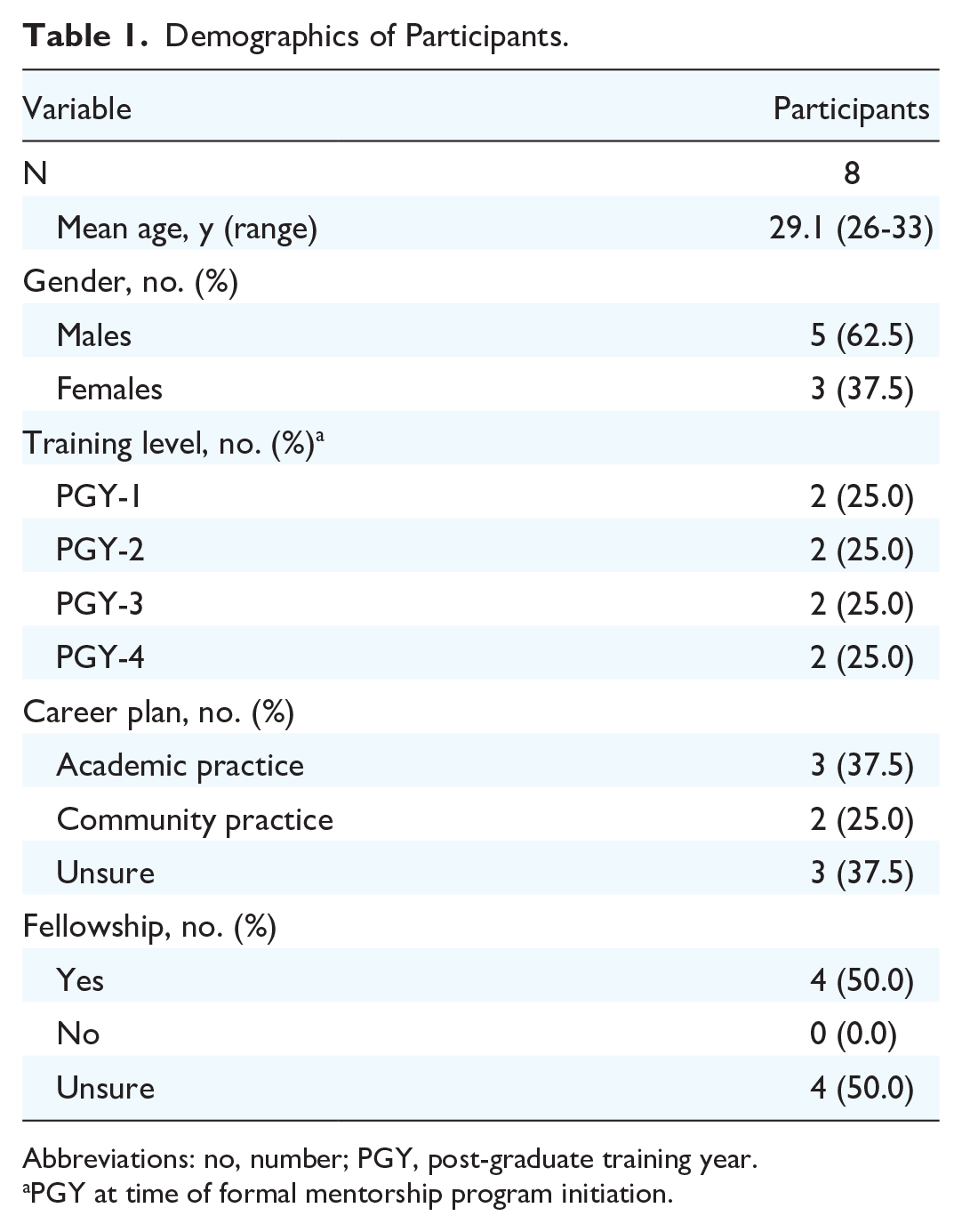
Abbreviations: no, number; PGY, post-graduate training year.
PGY at time of formal mentorship program initiation.
Burnout and Stress Outcomes
Baseline levels of stress and burnout were found to be high for all PGY years but highest for PGY 2 residents within the PSS scores (Table 2) and MBI (Table 3).
PSS10 Scores by PGY.
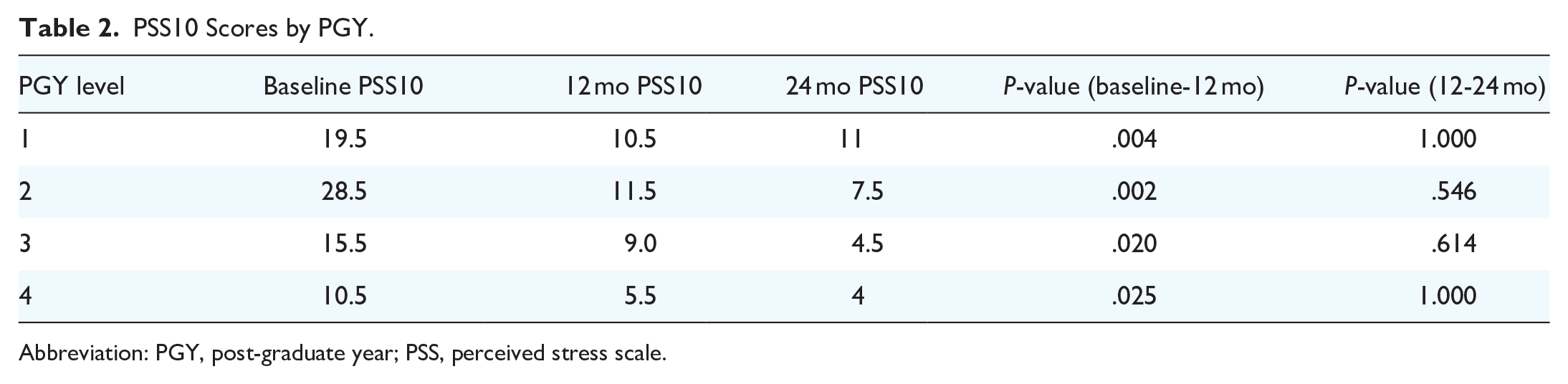
Abbreviation: PGY, post-graduate year; PSS, perceived stress scale.
MBI Scores by Post-Graduate Training Year.

Abbreviations: DEP, depersonalization; EE, emotional exhaustion; MBI, Maslach Burnout Inventory; PA, personal accomplishment; PGY, post-graduate year.
Table 4 shows the average PSS and MBI scores for the whole cohort. Compared to the baseline, the MBI changed from 47.6, 50.6, and 16.5 for emotional exhaustion, depersonalization, and personal accomplishment to 14.9, 20.1, and 40.1 at 12 months respectively (P < .0001). This subsequently changed to 13.3, 17.4, and 42.5 at 24 months. However, the change was not statistically significant for the emotional exhaustion domain (13.3, P = .061) and personal accomplishment (42.5, P = .168) compared from 12 to 24 months post-implementation of the FMP. This plateau in benefit from 12 to 24 months was seen in all the PGY years for MBI scores.
Average MBI and PSS Scores.

Abbreviations: MBI, Maslach Burnout Inventory-Human Services; PSS, Perceived Stress Scale.
PSS was found to be 18.5 at baseline and dropped to 7.9 (P = .001) at 12 months and again to 6.8 at 24 months. The change from 12 to 24 months, however, was not found to be statistically significant (P = 1.0). This plateau in benefit from 12 to 24 months was seen in all the PGY years for PSS scores.
QOL Outcomes
WH-QOL overall scores were high at baseline (71.9) corresponding with a low QOL (Table 5). The domain at the baseline with the lowest QOL was the environment at 69.9. There was a statistically significant improvement in overall QOL at 12 months (37.5, P = .002) and again at 24 months (17.2, P = .029). There was sustained improvement in all domains from 12 to 24 months except the psychological domain which did improve from 12 to 24 months but was not statistically significant (41.1 vs 34.4, P = .307). When the overall QOL score was broken down by PGY year (Table 6), however, there was statistically significantly sustained improvement at 24 months compared to 12 months for the PGY 1 (50.00 vs 25.00, P = .0450), PGY 2 (43.75 vs 18.75, P = .0280), and PGY 3 (43.75 vs 12.5, P = .0010). PGY 4 was the only year without sustained improvement (18.75 vs 18.75, P = 1.000).
Average WH-QOL Scores.

Abbreviations: QOL, quality of life; WH-QOL, World Health Quality of Life-Bref Questionnaire.
WH-QOL Overall QOL by Post-Graduate Training Year.

Abbreviations: PGY, post-graduate year; QOL, quality of life; WH-QOL, World Health Quality of Life-Bref Questionnaire.
Participant Satisfaction
Overall satisfaction for the FMP was sustained throughout the duration of FMP from baseline to 12 months and from 12 to 24 months as shown in Table 7. Residents were most satisfied by having provided a role model, feeling more supported, and having someone to turn to in times of difficulty.
Resident Satisfaction Likert Scale.

Staff Satisfaction
Staff satisfaction for the FMP was captured with a Likert scale. Staff generally had positive sentiments toward the program such as acting as a role model and feeling connected to trainees. These scores did not significantly change throughout the duration of the program.
Discussion
Medical residency training is a well-published stressful endeavor.12-18 Balancing a life of caring for sick patients with one’s personal life as well as meeting demanding learning objectives often leads to high amounts of stress which eventually culminates in burnout. Burnout is exceptionally problematic among medical trainees as it leads to not only poorer patient care but also physical and psychological distress to the physician. One known method of combating the effects of burnout is to provide trainees with mentorship. With its structured and temporal features, mentorship is a natural way of improving resident well-being. We implemented a rigorous FMP in an academic surgical program in 2015, with validated questionnaires to quantify residents’ levels of stress, burnout, and overall QOL. This showed promising results with significant improvements in MBI, PSS, and WH-QOL. 8 This mentorship program is also still ongoing at the institution whose data set is attached to this paper. While there are studies that have shown the short-term benefit of mentorship in different aspects of healthcare learning, the long-term outcomes are less well defined. Concern about the sustainability of resident benefits coupled with mentor fatigue are factors that may decrease benefits over time. Therefore, the purpose of this study was to assess the long-term benefit of the same successful mentorship program over a longer period. More specifically, attention was paid to whether the program and its mentors would be sustained as well as whether there would be a drop-off effect of benefit for the mentees participating in the program.
The residents within our group had a high baseline overall WH-QOL score of 71.9 with scores of 49.6, 57.8, 63.5, and 69.9 for the domains of physical health, psychological health, social relationship, and environment respectively. Our group also had MBI scores for emotional exhaustion, depersonalization, as well as low personal accomplishments within the upper third of normal. These results are not surprising given the known demands of surgical residency training balanced with personal well-being all set in a high-intensity learning environment. It was noted that baseline levels of stress and burnout were found to be high for all PGY years but highest for PGY 2 residents within the PSS scores and MBI. It is possible that the PGY2 year in otolaryngology residency programs often coincides with an increased level of stress due to the increased independence, despite still being a junior resident and the beginnings of solo call coverage. Previous studies from Doolittle et al (2013) 16 as well as Bellieni et al 18 have shown similar and even higher baseline MBI domains within the medical educational landscape.16,18 Within our group, the FMP was found to be beneficial at 12 months where MBI reached the lower third percentile of normal for all 3 subcategories. This result was found in the PSS scale (7.9, P = .001) as well as the WH-QOL survey (37.5, P = .002). These results were sustained for MBI in all domains from 12 to 24 months but did not reach statistical significance in that time frame. This was seen in the PSS survey as well from 12 to 24 months (7.9 vs 6.8, P = 1.0). This is also supported by the overall WH-QOL life score for PGY 4 residents, where there was no improvement from 12 to 24 months (18.75 vs 18.75, P = 1.000). The lack of further statistically significant improvement in MBI, PSS, and WH-QOL overall scores reflects the inherent nature of surgical training. While the FMP helped to provide residents with role models and helped them feel more supported initially, the stress of balancing education and personal life while caring for patients is ongoing. However, the sustained MBI score within the lower third of normal along with PSS shows that the benefit transcends PGY years. This is especially interesting to see within the PGY 4 group who at the end of the 24-month survey had reached their PGY 5 year, where the added stress of career planning and studying for board certification exams come into play. The maintenance of their MBI scores in all domains and the PSS was encouraging as it reflects the ability of the FMP to provide sustained benefit through transition periods with new life stressors.
Overall QOL also improved within our resident group. Overall WH-QOL scores improved from baseline to 12 months (71.9 vs 37.5, P = .002). This further improved from 12 to 24 months (37.5 vs 17.2, P = .029). This improvement was seen in all the WH-QOL domains except for the psychological domain (41.1 vs 34.4, P = .307) which showed sustaining of the score at 12 months with no statistically significant improvement. The psychological domain within the WH-QOL mainly centers on questions around positive feelings, learning, memory and concentration, self-esteem, bodily image, and appearance, as well as negative images. It is the only domain that reflects the resident’s own personal feelings about themselves. The lack of improvement at 24 months from 12 months supports the MBI and PSS findings of sustainability over that same time frame. While residents feel more supported during this time, they still have the baseline natural stress of surgical training. Positive feelings, self-esteem, and clarity of thought are all tied to these and can be reflective of the limitations of the FMP. While the FMP can certainly help with stressors and burnout with improvement in QOL, it cannot entirely remove the natural stressors at play. Curriculum and learning environment development are also vital components to resident well-being and should be considered as well when taking resident learning into account. 19
One limitation of this paper is the lack of a control group, as further discussed below. While not suitable for statistical analysis, given the small sample size, 24-month PGY1 data was compared to baseline PGY3 data. The 24-month PGY1 data had lower PSS and MBI scores compared to the baseline PGY3 data, except in the realm of personal accomplishment. While this observation is limited statistically, this general pattern of results further supports the utility of the mentorship program. It helps distinguish the natural comfort that comes with being in a program for a longer period of time versus the possible benefits of the mentorship program itself.
Despite the benefits of mentorship shown within the literature in reducing the stress levels of trainees, FMP is not widely implemented in most programs and there is great variability in trainees’ mentorship experiences.6,20 Our formal and consistent mosaic model of mentorship with strong overseeing governance is certainly the backbone of the success of the program. The long-term sustained benefit in MBI, PSS, and WH-QOL is coupled with sustained resident satisfaction from 12 to 24 months overall (0.90-0.91, P = 1.000) and in all domains.
In order for an FMP to be successful, not only do mentees need to take their role seriously, 7 such as seeking appropriate guidance and preparing for meetings, but there needs to be mentor interest and time in pursuing such a relationship. Qualities of good mentors have been previously described and they include those individuals who motivate, empower and encourage their mentees, nurture self-confidence, teach by example, offer wise counsel, have a high performance bar, and shine in a reflected light. 21 Mentor burnout must be mitigated, and their own satisfaction is also important. Within our cohort, our residents had sustained overall satisfaction from baseline to 12 to 24 months. The structure of the program with strong systemic support likely helped to sustain overall mentor satisfaction scores over 24 months. The governance committee did not need to intervene at any point during the study. The strong pool of mentors within our group (14 academic staff coupled with 8 residents) allowed one-to-one resident-to-mentor interactions. This decreases time demands and increases how well the mentors get to know their mentees. The benefits of mentorship are not isolated to the mentee. Feelings of personal accomplishment are a protector against high burnout 1 and giving back to the mentees can be protective to the mentors. Moreover, the FMP among residents and their staff function to create a culture of ongoing supportive networks. After all, sometimes, “even the mentors need mentors.” 4
Limitations
This study is not without its limitations. There is no control group so it is difficult to say whether the benefits seen in this study can be attributed to the FMP intervention. Moreover, given that participants are not blinded to the study, they are susceptible to the Hawthorne effect.
Conclusion
Our study provides a long-term follow-up of a previously successful FMP program implemented in an academic surgical training program. There was sustained improvement in stress, burnout, and overall QOL scores over a 2-year period. Consideration should be given to administering FMP in medical training programs where similar issues with resident well-being exist.
Footnotes
Acknowledgements
None.
Author Contributions
SM: involved in the acquisition, analysis & interpretation of data, drafting, and revising work, provides final approval to submit this paper, and agrees to be accountable for all aspects of this work. HS: involved in the conception & design of work, acquisition of data, and revising the work, provides final approval to submit this paper, and agrees to be accountable for all aspects of this work. YA: involved in the conception & design of work, acquisition of data, and revising the work, provides final approval to submit this paper, and agrees to be accountable for all aspects of this work. EDW: involved in the conception & design of work, acquisition of data, and revising the work, provides final approval to submit this paper, and agrees to be accountable for all aspects of this work. HE: involved in the conception & design of work, acquisition of data, and revising the work, provides final approval to submit this paper, and agrees to be accountable for all aspects of this work. HZ: involved in the conception, design, acquisition, analysis of data, and revising of the work, provides final approval to submit this paper, and agrees to be accountable for all aspects of this work. Please address correspondence to: Dr. Han Zhang. Division of Otolaryngology – Head and Neck Surgery, McMaster University, Hamilton, Canada. St. Joseph’s Healthcare 50 Charlton Ave E Hamilton, ON L8N 4A6
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study was approved by the Health Research Ethics Board at the University of Alberta.