
Abstract
Importance
Metastases to the submandibular gland (SMG) from oral cavity primaries are very rare. Hence, a gland-preserving level IB dissection technique is a feasible option without compromising the lymph node yield (LNY).
Objective
To assess the feasibility and noninferiority of the SMG-preserving dissection technique to the conventional en bloc removal of level IB in terms of LNY in patients with cN0 oral squamous cell carcinoma (OSCC) undergoing elective neck dissection.
Design
Parallel-design, single-center, open-label, randomized controlled trial.
Setting
Tertiary care health care center—Department of Otorhinolaryngology-Head & Neck Surgery, AIIMS Rishikesh.
Participants
Thirty-eight (n = 38) participants with 46 (n = 46) neck dissection specimens of OSCC were randomly allocated (1:1) into gland-preserving (n1 = 23) and en bloc (n2 = 23) dissection groups.
Intervention
Elective neck dissection comparing SMG-sparing level IB dissection technique versus en bloc level IB dissection.
Main Outcome Measures
LNY, lymph node density, and level IB operative time in both groups were compared between groups (α < .05).
Results
Median LNY (P = .543) and lymph node density (P = 1.000) in level IB did not show significant differences between the groups. LNY in level IB by gland-preserving technique is also not inferior to the conventional en bloc dissection technique (mean difference = 0.217; 95% CI: [−0.597, 1.032]; P = .593). The mean level IB operative time is significantly longer in the gland-preserving group (P < .001).
Conclusions and Relevance
None of the examined SMGs were involved by the tumor. SMG-preserving technique is noninferior to the traditional technique of level IB clearance and can be used in elective neck dissections without compromising the LNY. Functional neck dissection has greatly evolved to decrease patient morbidity, and this method can be adopted in case-specific situations.
Trial registration
The trial was registered in the Clinical Trials Registry—India (CTRI/2022/05/042344) on May 2, 2023, https://ctri.nic.in/.

Keywords
Key message
Submandibular gland capsule prevents the direct extension of tumor.
Intraglandular lymph nodes are very rarely seen within submandibular gland.
Submandibular gland can be preserved in elective neck dissections.
Introduction
Oral squamous cell carcinoma (OSCC) is the most common head and neck malignancy worldwide. 1 Though metastases to ipsilateral level IB are found in about 39% of untreated patients, 1 the submandibular gland (SMG) has been reported to be involved by the tumor in less than 5% of the cases. 2 SMGs contribute to 70% of the unstimulated salivary flow; 21% of patients develop postoperative xerostomia after unilateral submandibular gland excision in neck dissection. 3 Manipulation of SMG during surgery can cause transient xerostomia noted in 7% of patients who underwent SMG-preserving neck dissection. More than 90% of the individuals with SMG preserved neck dissection had demonstrated intact salivary function. 4 The routes of SMG involvement are as follows: direct extension of the primary tumor, extranodal extension from positive submandibular lymph node, metastasis to intraglandular lymph nodes, and tumor extending along Wharton’s duct 5 (Figure 1). The objective of the inclusion of SMG in conventional level IB dissection is complete oncological clearance. Intraglandular lymph nodes in SMG is rare; hence, an appropriate oncological clearance is achievable by gland-preserving level IB dissection. 6 Postoperative radiotherapy (PORT) further reduces the submandibular salivary flow even if the gland has been preserved. The removal of a functional SMG will be an overcorrection and give more morbidity in those cases where PORT is not indicated. Thorough clinical examination and radiological investigations can identify the candidates for SMG preservation. Retrospective observational studies support the idea of preserving SMG.7-9 However, there is a lack of consensus or high-level evidence regarding this issue. This study aimed to assess the feasibility and noninferiority of the SMG-preserving dissection to the conventional en bloc removal of level IB in terms of lymph node yield (LNY) in patients with cN0 OSCC undergoing elective neck dissection.

Modes of submandibular gland involvement by oral cavity malignant tumor.
Materials and Methods
A parallel-design, single-center, open-label, randomized controlled trial was proposed to test the noninferiority of the gland-preserving level IB dissection to the traditional en bloc level IB dissection.
The institutional ethics committee (AIIMS/IEC/22/20) gave prior approval. The trial is registered in the Clinical Trial Registry—India (CTRI/2022/05/042344).
Patients with OSCC presented to the Department of Otorhinolaryngology-Head & Neck Surgery from February 2022 to January 2023 were subjected to screening evaluation for recruitment. Those who had a primary lesion in/reaching the floor of the mouth, underwent any previous major surgery in the head and neck, received chemoradiotherapy, paramandibular spread of disease, or very extensive disease were excluded from the study since the tumor front will be adjacent to the SMG in cases and level IB might have to be excised along with the primary tumor. Thirty-eight patients with OSCC with cN0, who gave consent for participation, were allocated by simple random method in a 1:1 ratio to one of the 2 groups by using an online open-source research randomizer tool under supervision. 10
All the participants in this study underwent ipsilateral elective neck dissection (I-III). Contralateral neck dissection (I-III) was performed for primary tumors reaching or crossing the midline. In the control group (en bloc excision), level IB was dissected with the submandibular gland and the periglandular soft tissue en bloc. In the study group (SMG-preserving group), level IB dissection was performed in 6 parts: preglandular, postglandular, prefacial, postfacial, deep group, and the submandibular gland (SMG) separately (Figure 2). The SMGs in the study group were examined for any residual or intraglandular lymph nodes. The samples were analyzed, and LNY (ie, number of lymph nodes harvested) and density (LND, ie, the ratio of the number of positive lymph nodes to the number of lymph nodes harvested) of level IB were compared between the groups. Level IB operating time (in minutes) and incidences of marginal mandibular palsy were also evaluated.

Schematic diagram Level IB dissection in the study group [1—preglandular, 2—prefacial, 3—postfacial, 4—postglandular, 5—submandibular gland (SMG), 6—deep (to SMG) group]. SMG, submandibular gland.
The results were analyzed with SPSS for Windows version 26 (IBM Corp., Armonk, NY, USA). Median LNY and LND were compared using the Mann-Whitney U test. The noninferiority was tested by calculating the mean difference between the groups. Mean operative time was compared using an independent samples t-test. The association between marginal mandibular palsy and group allocation was analyzed using χ2 (chi-square) test. A P-value less than .05 was considered to be statistically significant.
Results
A total of thirty-eight (n = 38) participants with OSCC with cN0 neck status were enrolled in the study. Seventeen and 13 participants underwent ipsilateral neck dissection (level I-III) in the study and control groups, respectively, and 8 participants (3 in the study group and 5 in the control group) underwent bilateral neck dissection (levels I-III). Hence, a total of forty-six (n = 46) neck dissection specimens, with 23 in each group, were finally analyzed.
The mean age of the participants was 46.81 + 12.25 years. 86.8% of the participants were males. The subsites of the primary lesion in decreasing order of frequency were oral tongue—15 (39.5%), buccal mucosa—12 (31.6%), alveolar ridge—4 (10.5%), hard palate—3 (7.9%), retromolar trigone—2 (5.3%), and mucosal lip—2 (5.3%) (Table 1).
Comparison of Baseline Characteristics.
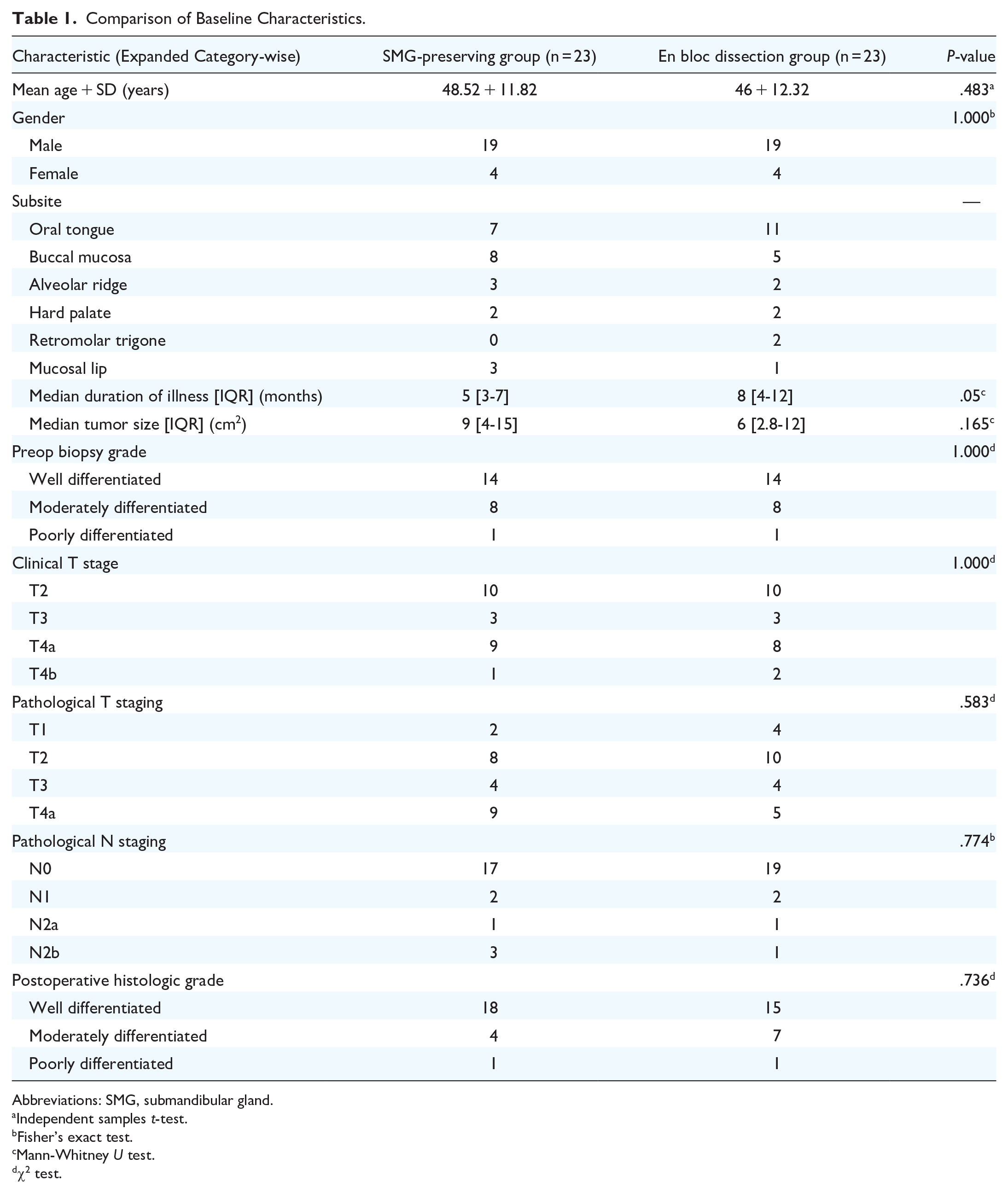
Abbreviations: SMG, submandibular gland.
Independent samples t-test.
Fisher’s exact test.
Mann-Whitney U test.
χ2 test.
There were no significant differences in terms of LNY (P = .543) and lymph node density (P = 1) between the groups and the various subsites. The SMG-preserving technique is not inferior to the traditional en bloc dissection in terms of LNY, mean difference = 0.217, 95% CI: [−0.597, 1.032] (P = .593). The median operative time in the gland-preserving group was significantly longer than the traditional technique (P < .001). Using the mean differences between the 2 groups, a post hoc power analysis has been performed using the G*Power software version 3.1.9.7. The computed power (1−β) of the statistical test was lower (13.3%). All the submandibular glands in both the groups are free of tumor, and no intraglandular lymph nodes have been found in any SMG. None of the SMGs in the study group revealed any residual lymph nodes. The comparison of data between the 2 groups is summarized in Table 2.
Comparison of Outcome Variables Between the 2 Groups of the Study Population.

Abbreviations: LNY, lymph node yield; SMG, submandibular gland.
Independent samples t-test.
Mann-Whitney U test.
χ2 test.
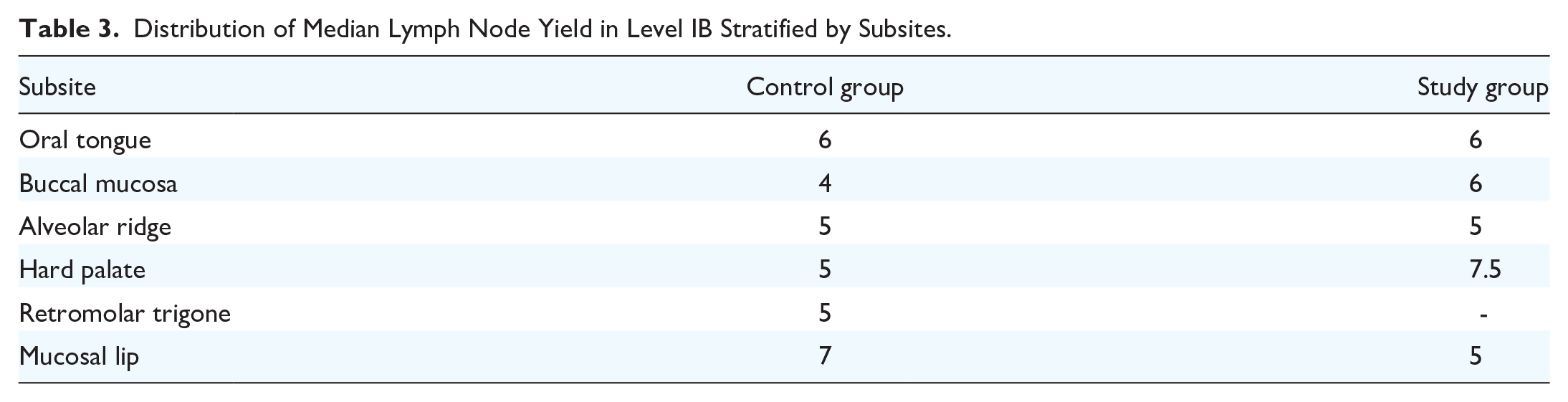
The LNY obtained by the gland-sparing technique is almost the same as that obtained by the en bloc dissection method (Table 3).
Distribution of Median Lymph Node Yield in Level IB Stratified by Subsites.
Postoperative radiotherapy was required in 6 patients in view of high-risk pathological behavior. One of the 4 positive nodes in level IB (4/257) examined showed extranodal extension, but none of the SMG is involved by the tumor (Table 4).
Nodal Characteristics of the 4 Patients Who Received Radiotherapy.
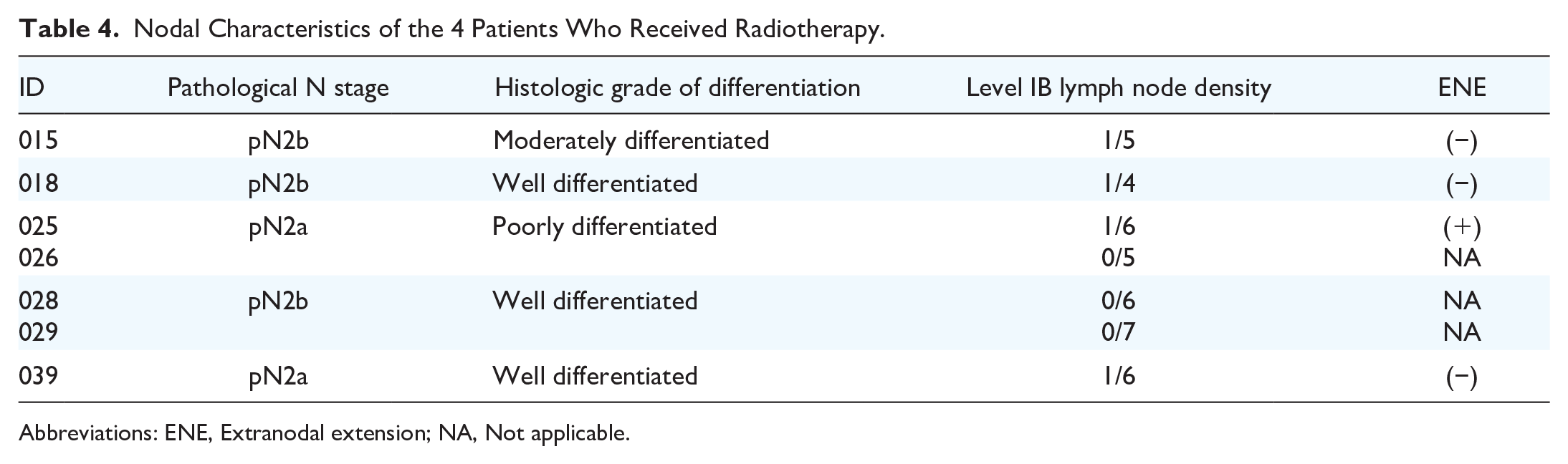
Abbreviations: ENE, Extranodal extension; NA, Not applicable.
Discussion
Our study aimed to prove the noninferiority of the SMG-preserving technique of level IB dissection to the traditional en bloc level IB dissection in terms of LNY. LNY is taken as a surrogate marker for the quality of the neck dissection performed. 11 Historically, many changes in practice happened since the radical neck dissection was performed as an adjunct in head and neck malignancies. Functional neck dissection was initially described by Suárez in 1962, to preserve nonlymphatic structures in N0 nodal status and resulted in a significant reduction in postoperative morbidity and improved functionality. 12
Li et al., in their systematic review and meta-analysis, have concluded that the adequate LNY for unilateral neck dissection is 18 and is a better prognostic indicator during follow-up. LNY has been in use for checking the quality standards of surgical procedures since the past. 13
Given the chance of extranodal extension from a positive node penetrating the tough fibrous capsule, it is relatively rare. Still, the intraoperative nature of lymph nodes plays a significant role in the decision to preserve the SMG. In our study, reactive-appearing oval, firm, enlarged nodes present in the periglandular fibrofatty tissue were separated and sent for analysis as per protocol. Group allocation conversion did not happen since there was no gross capsular breach. Level IB positivity rate in our study was 8.6%. The literature review revealed a wide range of this parameter (6%-32%) since the studies had considerable heterogeneity. Iocca et al. in a systematic review and meta-analysis included and analyzed retrospective studies and systematic reviews and meta-analyses, which included patients with OSCC separately. A pooled incidence of 1.2% and 1.6% of SMG involvement by the tumor was found in retrospective reviews and meta-analyses (I2 = 57.5%), respectively. 14 None of the SMGs was found to be involved by the tumor in our study.
Operative time duration is a poor measure of quality check of the procedure since it is interacted by various factors—surgeon, procedure, and environment. The dissection technique involves the preservation of the mylohyoid muscle, lingual artery, facial artery, lingual nerve, submandibular ganglion, and hypoglossal nerve apart from SMG in the study group. The learning curve will greatly affect the outcome since these impose technical nuances required for gland preservation strategy, and it has no established standard guidelines. Our study showed a significant difference in mean operative time between the groups.
A literature review was performed to extract similar and supportive studies. Retrospective studies that have been carried out in patients with OSCC who underwent neck dissection suggest that the SMG is very rarely involved by the tumor.7-9,12,13,15-17 Floor of mouth involvement predisposes the SMG to be at high risk of direct tumor extension, and the inclusion of the gland is oncologically suggestive of an R0 resection margin. 8 Lymphoid aggregates or lymph nodes within gland substances are proven to be very rare. Some studies proposed that lymphatic drainage of the oral cavity bypasses the SMG. 18 Other factors associated with gland involvement include poor differentiation of the tumor and perineural/lymphovascular invasion.1,9
A prospective study comparing locoregional control and disease-specific survival has found no significant difference between gland-sparing technique and en bloc dissection. 19 Small local defects can be closed using submandibular glandular flaps, as described by Zeng et al., with decreased postoperative morbidity. In their study, after a median follow-up period of 14 months, there was no local site residual or recurrence. 9
Based on the results, candidates for the gland-sparing technique can be selected based on preoperative tumor characteristics such as T staging and histological grading. Further research is needed in line to address the neck when postoperative radiotherapy is required in a patient who has undergone a gland-sparing neck dissection. PORT by intensity-modulated radiotherapy has the option for adjusting the clinical target volume to spare the SMG functionality.20,21
Limitations
The low statistical power of our study is due to the limited number of enrolled participants. Since there is no consensus for preserving SMGs in elective neck dissections, SMGs were removed and examined in both groups. The study compared the feasibility of using the SMG-preserving technique by analyzing the ultimately-removed SMGs. Also, follow-up protocols are needed to implement the method on a large scale. The learning curve is another limitation to gaining technical expertise in preserving SMG with minimal intraoperative handling so that postoperative functionality is spared.
Conclusion
This study was conducted to generate evidence for the rationale of preserving the SMG during elective neck dissection in patients with cN0 OSCC, as there is no consensus on this topic. Preserving functionality in SMGs can be adopted as part of elective neck dissection in selected patients with OSCC, with technically no difference in LNY.
Footnotes
Acknowledgements
Not applicable.
Author Contributions
G.V.: Review of literature, protocol, data collection, analysis, manuscript. A.M.: Review of literature, data collection, manuscript. B.J.: Protocol, data collection, analysis, manuscript review. P.D.: Protocol, study design, specimen analysis, manuscript review. A.K.: Protocol, study design, literature review, analysis, manuscript review. A.K.T.: Protocol, data collection, study design, manuscript review. S.K.P. and A.H.: Study design, manuscript review. K.S.M.: Review of literature, data collection, manuscript review. V.S.: Protocol, data collection, review of literature, manuscript. N.R.: Data collection, review of literature. A.S., A.C.Y, and M.R.P.: Review of literature, manuscript. R.S.: Data collection, review of literature, manuscript.
Consent for Publication
The consent for using the data in research purpose and publication was obtained.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
A prior approval was obtained after submitting the protocol to the Institutional Ethics Committee, AIIMS Rishikesh (AIIMS/IEC/22/20). The participants were explained regarding the nature of the study, and an informed consent form was obtained before enrolling the patients in the study.