
Abstract
Background
The outcomes of recent advancements in pediatric tracheostomy remain unclear. This study was conducted to identify the trends in pediatric tracheostomy in Taiwan.
Methods
This population-based survey was conducted using data from Taiwan’s National Health Insurance Research Database. We identified inpatients younger than 18 years who had undergone tracheostomy in Taiwan between 2000 and 2019. The study period was divided into subperiods (2000-2004, 2005-2009, 2010-2014, and 2015-2019). We analyzed patient characteristics and trends related to age, gender, hospital level, surgical indications, hospital stay duration, and mortality rates. The trends were analyzed for all pediatric patients (age <18 years) and infants (age <1 year).
Results
This study included 2465 pediatric patients (mean age: 8.7 ± 6.9 years; boys: 64%). The incidence of pediatric tracheostomy decreased from 3.3 events per 100,000 individuals in 2000 to 2.1 events per 100,000 individuals in 2019 (P for trend < .001). The proportion of infants who received tracheostomy increased from 22.8% in 2000-2004 to 32.5% in 2015-2019 (P for trend = .06). The proportion of pediatric patients who received tracheostomy at medical centers increased and those at regional hospitals or district hospitals decreased (74.7%-81.0% vs 25.3%-19.0%, P for trend = .003). The proportion of pediatric patients with trauma or brain injury as a surgical indication decreased from 36.6% to 28.7% (P for trend = .001). The duration of intensive care unit (ICU) stays increased from 30 days in 2000-2004 to 50 days in 2015-2019 (P for trend < .001), and that of hospital stay increased from 58 days in 2000-2004 to 71 days in 2015-2019 (P for trend = .001). The 5-year mortality rate slightly decreased from 38.0% in 2000-2004 to 33.3% in 2005-2009 and 31.0% in 2010-2014 (P for trend = .006).
Conclusions
Our findings revealed that during the study period, the number of pediatric patients receiving tracheostomy decreased, but the proportion of infants receiving tracheostomy increased. The trends in pediatric tracheostomy indicated extended ICU stay, prolonged hospital stay, and reduced 5-year mortality rates.
Introduction
Tracheostomy involves the introduction of a cannula into the trachea of a patient.1,2 In children, upper airway obstruction caused by inflammatory diseases, congenital anomalies, or conditions that require long-term intubation are the indications for tracheostomy.1,2 Children undergoing tracheostomy constitute a highly complex cohort that has a continual reliance on tracheostomy and associated medical technology for long-term survival. Pediatric tracheostomy and postoperative care remain challenging, and children undergoing tracheostomy are at high risk of adverse events and mortality.3-6
Over the years, substantial advances have been made in pediatric tracheostomy.7-16 In the 1970s and 1980s, airway obstruction due to acute inflammation was the most common indication for pediatric tracheostomy. 11 Currently, most clinicians consider ventilator dependence to be an indication for pediatric tracheostomy, and upper airway obstruction is less frequently considered an indication for this procedure. 9 With advancements in techniques, equipment, care bundles, and caregiver skills, pediatric tracheostomy has been performed more frequently, with lower risks of perioperative and long-term complications.1,17-19 Muller et al conducted a population-based study in the United States using data from 2000 to 2012, which revealed an increase in the duration and cost of hospital stay during the study period, as well as regional disparities in rates and outcomes. 15 Few population-based studies have analyzed trends in the long-term outcomes of recent advancements in pediatric tracheostomy.
Researchers worldwide have increasingly conducted analyses using data from national databases.15,20-28 The use of national databases to conduct population-based surveys reduces the risk of referral bias and increases the accuracy of information on clinical practices.15,20-27 Using population-based data, researchers have analyzed the trends in pediatric tracheostomy in the United States,15,20-24 Canada, 25 Japan,26,27 and Taiwan. 28 In Taiwan, the National Health Insurance (NHI) program was introduced in March 1995; this program covers >99% of Taiwan’s entire population (approximately 23.9 million).29-31 The National Health Insurance Research Database (NHIRD) comprises the insurance claim data of the entire insured population, and this database can be used by researchers for conducting population-based epidemiological analyses of diseases and procedures.30,31 The present study is an extension of our previous NHIRD study on pediatric tracheostomy in Taiwan. 28
This study aimed to identify trends in pediatric tracheostomy in Taiwan. From the NHIRD, we identified pediatric patients who had undergone tracheostomy in Taiwan between 2000 and 2019. The trends in age, gender, hospital level, surgical indications, perioperative care, and mortality rates in the study cohort were analyzed. Evidence suggests that a considerable proportion of children undergoing tracheostomy are aged <1 year at the time of tracheostomy tube placement. 3 Therefore, we analyzed trends for all pediatric patients (age <18 years) and infants (age <1 year).
Materials and Methods
Ethical Approval
This study was approved by the Ethics Committee of Taipei Hospital, Ministry of Health and Welfare, Taiwan (approval number: TH-IRB-0018-0027). The EQUATOR guidelines and Essentials of Wiring Biomedical Research Papers were followed. The personal data of patients are deidentified in the NHIRD. Hence, the requirement for informed consent was waived.
Database
This retrospective cohort study was conducted using claim data from the NHIRD. Taiwan’s NHI program is a single-payer health insurance system. Enrollment in the NHI program is obligatory, and copayments are affordable. The NHIRD is managed by the Health and Welfare Data Science Center of the Ministry of Health and Welfare. Taiwan. We applied to the relevant authorities for obtaining insurance claim data for the period from 2000 to 2019; the data were made available through the National Health Informatics Project. Disease diagnoses were confirmed using relevant codes from the International Classification of Diseases, Ninth Revision, Clinical Modification before December 31, 2015, and the International Classification of Diseases, Tenth Revision, Clinical Modification after 2015.30,31
Patients and Incidence of Pediatric Tracheostomy
Pediatric patients who had undergone tracheostomy in Taiwan between 2000 and 2019 were identified from the NHIRD by using NHI reimbursement codes. If a patient was hospitalized for tracheostomy more than once during the study period, data pertaining to the patient’s first hospitalization were analyzed. Data on the numbers of all pediatric patients and infants who underwent tracheostomy during the study period were obtained from a web-based report published by the Department of Statistics, Ministry of the Interior. 32 The incidence of pediatric tracheostomy in Taiwan is presented as the number of events per 100,000 individuals in a given year. 28
Covariates and Outcomes
Statistical models were adjusted for the following covariates: age, gender, hospital level (medical center vs regional or district hospital), and surgical indications. The study cohort was divided into the following age groups: infants (<1 year), toddlers (1-2.9 years), preschool children (3-5.9 years), school children (6-11.9 years), and adolescents (12-17.9 years). 28 Surgical indications were identified using inpatient diagnoses made during the index hospitalization for tracheostomy; these indications included trauma or head injury, congenital anomalies, respiratory or pulmonary disorders, neurological disorders, and neoplasm or malignancy. 28 Some patients had ≥2 indications for tracheostomy. The study outcomes were the duration of hospital stay, the duration of intensive care unit (ICU) stay, and the rate of mortality. Prolonged hospitalization was defined as hospitalization for >1, >3, and >6 months. We evaluated the rates of in-hospital, 1-month, and 5-year mortality. Data on the date and cause of death were linked using the Taiwan Death Registry database, which is managed by the Health and Welfare Data Science Center.
Statistical Analysis
Statistical analyses were performed using SAS (version 9.4; SAS Institute, Cary, NC, USA). This population-based study included all patients during the study period to reduce referral bias. A Poisson model was used to analyze the linear trends in the incidence of pediatric tracheostomy during the study period. The natural logarithm of the population size in a given year was used as an offset variable, the number of pediatric patients undergoing tracheostomy was used as a response variable, and the study year was used as an explanatory variable. Linear trends in patient characteristics and outcomes across the study subperiods (2000-2004, 2005-2009, 2010-2014, and 2015-2019) were examined using one-way analysis of variance (by applying a linear contrast) for continuous variables (eg, age) or the Cochran–Armitage test for categorical variables (eg, gender). 33 Across the subperiods, in-hospital outcomes such as the hospital stay duration and in-hospital mortality rate were compared using a logistic regression model, and the 5-year mortality rate was analyzed using a Cox proportional-hazards model. To reduce the possible confounding bias, the aforementioned regression analyses were further adjusted for age, gender, hospital level, and surgical indications. All analyses were performed separately for all pediatric patients and infants. A P value of <.05 indicated statistical significance.
Results
Study Cohort
This study included 2465 pediatric patients (mean age: 8.7 ± 6.9 years; Table 1). Of them, 622 (25.2%) were infants, 244 (9.9%) were toddlers, 190 (7.7%) were preschool children, 331 (13.4%) were school children, and 1078 (43.7%) were adolescents. Approximately 64.1% of the patients were boys. In the study population, 76.4% underwent tracheostomy at medical centers and 23.6% at regional or district hospitals. The median duration of ICU stay was 37 (interquartile range: 16-77) days and that of hospital stay was 62 (interquartile range: 34-109) days. The proportions of patients who were hospitalized for >1, >3, and >6 months were 75.9%, 49.4%, and 31.8%, respectively. The rates of in-hospital, 1-month, and 5-year mortality were 13.2%, 11.1%, and 28.9%, respectively.
Basic Characteristics in the Pediatric Patients (Aged <18 Years) Who Underwent Tracheostomy by Different Study Periods.

Abbreviations: ICU, intensive care unit; NA, not applicable.
The potential follow-up duration of patients admitted between 2015-2019 was less than 5 years; Data were presented as frequency (percentage), mean ± standard deviation, or median [25th percentile, 75th percentile].
Incidence of Pediatric Tracheostomy in Taiwan
Supplemental Table 1 presents detailed information on the number of pediatric patients undergoing tracheostomy and the incidence of pediatric tracheostomy in Taiwan between 2000 and 2019. The incidence of pediatric tracheostomy decreased significantly from 3.3 events per 100,000 individuals in 2000 to 2.1 events per 100,000 individuals in 2019 (P for linear trend < .001; Figure 1A). However, no significant change was observed in the incidence of infant tracheostomy during the study period (7.6 and 9.1 events per 100,000 individuals in 2000 and 2019, respectively; P for linear trend = .118; Figure 1B).

Number and incidence of tracheostomy for (A) all pediatrics (<18 years) and (B) infants (<1 year) in Taiwan from 2000 to 2019.
Covariates and Outcomes in All Pediatric Patients
In pediatric patients, no significant between-subperiod difference was observed in the trend related to age or gender. The proportion of patients undergoing tracheostomy at medical centers increased from 74.7% in 2000-2004 to 81.0% in 2015-2019, and the proportion of patients undergoing tracheostomy at regional hospitals or district hospitals decreased from 25.3% in 2000-2004 to 19.0% in 2015-2019 (P for trend = .003). Regarding surgical indications, the number of pediatric patients with trauma or brain injury decreased from 36.6% in 2000-2004 to 28.7% in 2015-2019 (P for trend = .001), and the number of pediatric patients with congenital anomalies increased from 23.3% in 2000-2004 to 33.3% in 2015-2019 (P for trend < .001). Furthermore, the duration of ICU stay increased from 30 days in 2000-2004 to 50 days in 2015-2019 (P for trend < .001), and that of hospital stay increased from 58 days in 2000-2004 to 71 days in 2015-2019 (P for trend = .001). The proportion of patients who were hospitalized for >6 months increased from 29.9% in 2000-2004 to 39.0% in 2015-2019 (P for trend = .003). The rate of in-hospital mortality did not vary significantly across the subperiods. However, the rate of 1-month mortality decreased significantly from 13.7% in 2000-2004 to 10.9% in 2015-2019, and that of 5-year mortality decreased from 38.0% in 2000-2004 to 31.0% in 2010-2014 (Table 1).
Multivariate regression was performed to identify the associations between the study subperiods and outcomes in all pediatric patients (Table 2). The rates of hospitalization for >1, >3, and >6 months were higher in 2015-2019 than in 2000-2004 [odds ratio: 1.67, 1.44, and 1.43, respectively; 95% confidence interval (CI): 1.24-2.25, 1.12-1.84, and 1.11-1.85, respectively]. The rate of 5-year mortality in all pediatric patients was significantly lower in 2010-2014 than in 2000-2004 (hazard ratio: 0.71; 95% CI: 0.59-0.86; Figure 2A).
The Association Between Study Periods and the Risk of Outcomes in the Pediatric Patients (Aged <18 Years) Who Underwent Tracheostomy.

Abbreviations: CI, confidence interval; HR, hazard ratio; OR, odds ration.
Adjusted for age, gender, hospital level, and indications for tracheostomy.
The potential follow-up duration of patients admitted between 2015-2019 was less than 5 years.
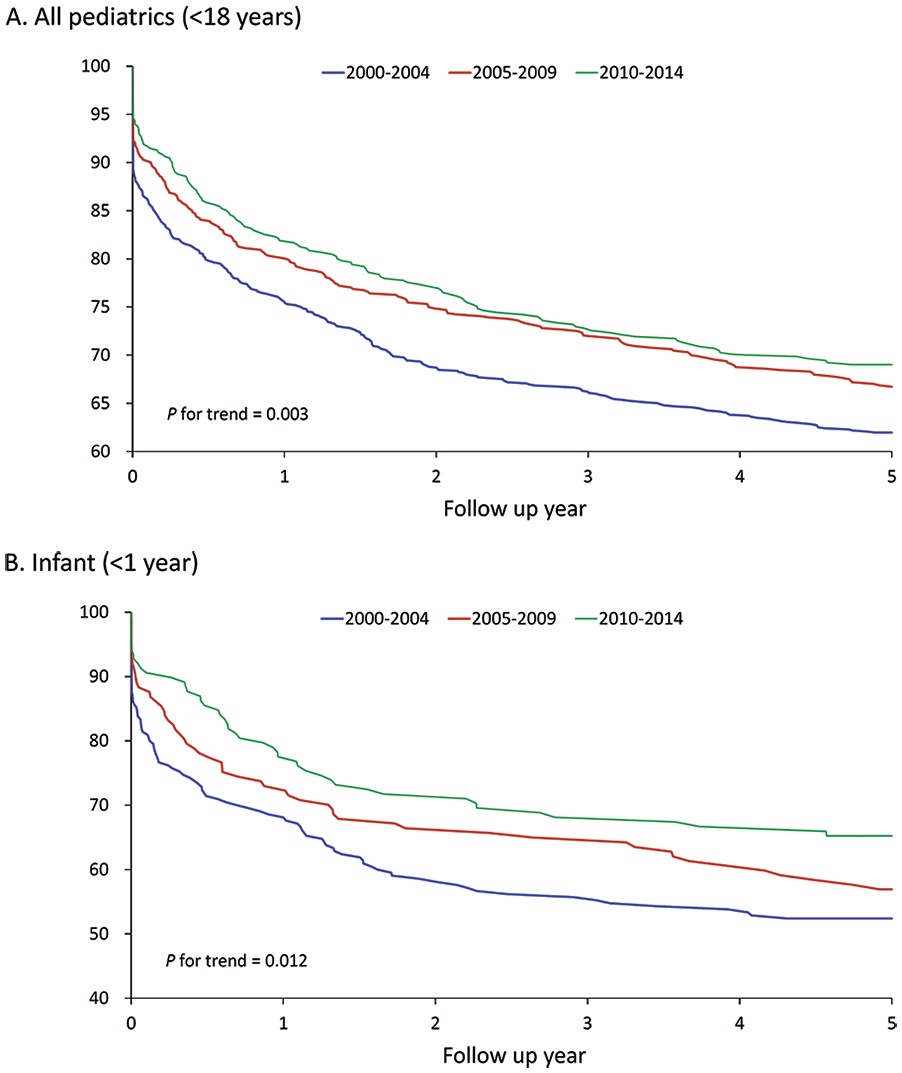
The Kaplan-Meier survival curves of 5-year mortality stratified by years in (A) all pediatrics, <18 years and (B) infants, <1 year. The patients who received tracheostomy during 2015-2019 were not analyzed because they did not have sufficient follow-up duration of 5 years.
Covariates and Outcomes in Infants
The infants’ mean age at the time of tracheostomy decreased significantly from 0.32 years in 2000-2004 to 0.22 years in 2015-2019 (P for trend = .002; Table 3). The proportion of patients undergoing tracheostomy at medical centers was consistent throughout the study period (≥95% in all subperiods). The duration of ICU stay increased significantly from 71.5 days in 2000-2004 to 100 days in 2015-2019 (P for trend = .046), and that of hospital stay increased from 77.5 days in 2000-2004 to 118 days in 2015-2019 (P for trend = .007). In addition, significant increases were noted in the proportions of infants who were hospitalized for >1, >3, and >6 months. The rate of in-hospital mortality remained consistent throughout the study period. However, the 1-month mortality rate decreased significantly from 18.6% in 2000-2004 to 10.9% in 2015-2019 (P for trend = .015), and the 5-year mortality rate decreased significantly from 47.6% in 2000-2004 to 34.8% in 2010-2014 (P for trend = .019; hazard ratio: 0.67; 95% CI: 0.47-0.94; Table 4, Figure 2B).
Basic Characteristics in the Infant Patients (Aged <1 Years) Who Underwent Tracheostomy by Different Study Periods.

Abbreviations: ICU, intensive care unit; NA, not applicable.
Not available due to the regulation of the Taiwan Health and Welfare Data Science Center; Data were presented as frequency (percentage), mean ± standard deviation, or median [25th percentile, 75th percentile].
The potential follow-up duration of patients admitted between 2015-2019 was less than 5 years.
The Association Between Study Periods and the Risk of Outcomes in the Infant Patients (Aged <1 Years) Who Underwent Tracheostomy.

Abbreviation: CI, confidence interval; HR, hazard ratio; OR, odds ratio.
Adjusted for age, gender, hospital level, and indications for tracheostomy.
The potential follow-up duration of patients admitted between 2015-2019 was less than 5 years.
Discussion
Study Strength and Clinical Implications
In this population-based survey, we identified long-term trends in the characteristics and postoperative outcomes of pediatric patients undergoing tracheostomy in Taiwan. Previous studies on trends in pediatric tracheostomy have primarily analyzed changes in surgical indications.7-16 One study indicated trends toward reduced risks of postoperative complications 12 and increased duration and cost of hospital stay in patients undergoing tracheostomy in the United States. 15 Researchers worldwide have been working to facilitate medical decision-making, preoperative evaluation, family education, efficient surgical procedures, and multidisciplinary postoperative care. 34 Few studies have analyzed long-term outcomes and mortality rates in pediatric patients undergoing tracheostomy. To the best of our knowledge, this is the first study to identify a decreasing trend in the 5-year mortality rate after pediatric tracheostomy. Our findings highlight that efforts toward improving tracheostomy have increased patient survival after pediatric tracheostomy. Future studies should focus on optimizing long-term care and resolving problems pertaining to decannulation.
Trends in Indications for Tracheostomy
Tracheostomy is an ancient surgical procedure. 35 This procedure was first performed by Caron in 1766 to remove a bean. 35 Pediatric tracheostomy has since evolved,7-16 and the most apparent change is related to its surgical indications. In the 1970s, infections such as laryngotracheobronchitis and epiglottitis were the most common indications for tracheostomy.11,13 Owing to improvements in the care strategies for patients with these infections and increases in the survival periods of premature infants and patients with congenital anomalies, pediatric tracheostomy is currently the most commonly performed in patients with prolonged ventilator dependence, upper airway obstruction, or hypotonia secondary to neurological disorders.9-14,16 Most studies analyzing the trends in pediatric tracheostomy are hospital-based surveys.9-14,16 The present study was conducted using claim data from the NHIRD. Therefore, data on patient’s comorbidities, indications for hospitalization, and indications for tracheostomy (eg, prolonged ventilation) may not have been reliably recorded. 28 A population-based study revealed a significant reduction in the proportion of pediatric patients undergoing tracheostomy, which was attributed to trauma or brain injury, reflecting the enhancements in Taiwan’s health policies 36 and health care system.29-31
Trends Related to Age
We defined infant patients (aged <1 years) as a solitary age group according to 2 previous prestigious studies by Muller et al and Lewis et al, which demonstrated that infants had a high rate of the procedure, long hospital stays, and high mortality.15,20 Our previous population-based study in Taiwan enrolled 2300 patients younger than 18 years with tracheostomy of which 584 patients (25.4%) were infants. 28 In Taiwan, we also observed tracheostomy in infants was more commonly indicated by congenital anomalies, had longer ICU stays, had longer hospital stays, and had a higher mortality rate than other age groups did. 28 In contrast, tracheostomy in adolescents was mostly indicated for trauma and head injury. 28 Therefore, we chose infant patients in their own category.
The gradual changes in indications for tracheostomy may have resulted in changes in the mean age of children undergoing this procedure.7,10 Palmer et al observed a gradual increase in the number of young individuals undergoing tracheotomy. 7 A national database survey conducted in the United States revealed a significant reduction in the rate of tracheostomy from 2000 to 2012, although no significant change was noted in the mean age of patients. 15 However, the aforementioned study did not separately analyze the data of infants. Our study is the first to analyze the trends in both pediatric and infant tracheostomy procedures and to compare the trends for all pediatric patients and infants. The number of patients undergoing tracheostomy and the incidence of tracheostomy decreased for all pediatric patients but remained consistent for infants throughout the study period (Figure 1A and B). Furthermore, the mean age remained consistent for all pediatric patients but decreased for infants (Tables 1 and 3). These findings indicate the effects of global initiatives aimed at optimizing pediatric tracheostomy and reveal a decreasing trend in the mean age of pediatric patients undergoing this procedure. 34
Trends in Hospitalization Duration and Outcomes
Pediatric tracheostomy is associated with prolonged hospitalization.15,20,26,28 National surveys have demonstrated that the mean and median durations of hospitalization in the United States are 50.2 and 37 days, respectively.15,20 A Japanese study conducted using nationwide insurance claim data reported that the median duration of hospital stay for pediatric tracheostomy was 5.8 months. 26 However, the present study revealed the mean and median durations of hospital stay were 97.6 and 62 days, respectively, indicating a trend toward prolonged hospitalization in Taiwan. These findings are consistent with those of a national survey conducted in the United States by Muller et al, who reported a gradual increase in the duration of hospital stay. 15 In young patients undergoing tracheostomy, the surgical procedure is typically complex and requires prolonged hospitalization.
Determining whether advancements in pediatric tracheostomy have led to reductions in the risks of postoperative complications and mortality is important. However, few studies have clarified the outcomes of recent advancements in this procedure.12,15 In their 30-year survey conducted in Switzerland, de Trey et al identified a trend toward a reduced risk of complications after tracheostomy. 12 A national database survey conducted in the United States revealed no annual variation in the rate of in-hospital mortality; however, the survey provided no data on the rate of long-term mortality. 15 The present study is the first population-based, longitudinal study with a 20-year follow-up period. Our findings are promising and reveal a trend toward a reduced risk of long-term mortality after pediatric tracheostomy.
Hospital Level
Hospital level in Taiwan is designated through the hospital accreditation system. Each hospital that applied for accreditation is subject to an expert team’s on-site inspection. 37 Hospitals with a higher accreditation level usually possess advanced diagnostic and therapeutic equipment along with comprehensive scope of clinical specialties, making them more capable of treating patients with complicated severe conditions. 38 In Taiwan, medical centers are the highest-ranked hospitals, followed by regional hospitals and district hospitals.37,38 Our analysis of the trend of pediatric tracheostomy showed the proportion of pediatric tracheostomy at medical centers increased and the proportion at regional hospitals or district hospitals decreased. This finding was in accordance with trends of pediatric tracheostomy toward young ages and indicated by congenital anomalies. Young children with congenital anomalies usually require care in medical centers for tracheostomies. Regional hospitals and district hospitals may also transfer these children to medical centers because of insufficient medical equipment or specialists.
Hospital-Based Studies Versus Population-Based Studies
Most studies on pediatric tracheostomy have been conducted using data from a single institution.7-14,39-41 However, the use of national databases for research purposes has gained prominence.15,20-28 Hospital-based studies provide clear details on surgical indications, hospital courses, and complications, whereas population-based studies provide reduced referral bias and national-level insights, and they examine pediatric tracheostomy using large samples and long-term follow-up data. In summary, hospital-based and population-based studies together provide useful information for clinical practice.
Comparisons with Other Healthcare Systems
We compare outcomes and trends in pediatric tracheostomy in Taiwan 29 with those in other similar healthcare systems globally.42-44 Healthcare systems in Taiwan and Canada are single-payer, publicly insured, and government-administered systems.29,43 In contrast, healthcare systems in the United States and Japan are multipayer covered by employer-sponsored health insurance and publicly funded health care for the elderly and low-income people.42,44 The in-hospital mortality in the United States, 15 tracheostomy-related mortality in Canada, 45 and the mortality rate in Japan 26 were similar to those in our previous population-based study in Taiwan, 28 implying pediatric tracheostomy outcomes may not be significantly differed between single-payer and multipayer health system. Of note, a recent 2023 study in the United States by Van Horn et al reported readmission after pediatric tracheostomy was higher in publicly insured compared with children with private insurance. 46 However, the role of insurance status on other outcomes (eg, mortality) in pediatric tracheostomy remains unclear.
Global trends of pediatric tracheostomy are toward a shift of surgical indication,9-14,16 performed in younger ages7,10 with longer hospitalization duration, 15 and lower complications. 12 These trends have been observed in Taiwan 28 and other similar healthcare systems.7-16 Furthermore, the present study is the first one to report trend of mortality in pediatric tracheostomy in a longitudinal, population-based study.
Future Direction
This population-based study provides great knowledge for pediatric and general otolaryngologists, respirologists, intensivists, neonatologists, and policymakers. Our findings also bring insights into other similar healthcare systems for health reform. Furthermore, the quality of care in Taiwanese children with tracheostomy still needs to be improved. The government may launch additional children’s health care improvement programs. Our National health database study can provide information for the design of an improvement program. Future research should also investigate strategies for continually improving the quality of care and outcomes in pediatric tracheostomy
Limitations
This study had some limitations. First, surgical indications were identified using relevant diagnostic codes from the International Classification of Diseases, Ninth Revision, Clinical Modification or International Classification of Diseases, Tenth Revision, and Clinical Modification, which are not necessarily consistent with the patient’s medical charts. Second, the NHIRD does not provide information on disease severity or surgical details. Third, comprehensive data on postoperative care could not be analyzed and minor postoperative complications may not have been recorded in the NHIRD. Finally, although we identified a decreasing trend in the 5-year mortality rate after pediatric tracheostomy, we could not analyze the causes of death because the NHIRD does not provide reliable information on this.
Conclusion
In this population-based study, we identified the trends in pediatric tracheostomy in Taiwan between 2000 and 2019. We found that the proportion of pediatric tracheostomy decreased but the proportion of infant tracheostomy increased during the study period. Furthermore, the durations of ICU stay and hospital stay for tracheostomy increased and the 5-year mortality rate decreased for all pediatric patients and infants. However, the in-hospital mortality rate remained consistent throughout the study period.
Supplemental Material
sj-docx-1-ohn-10.1177_19160216241293069 – Supplemental material for Trend of Pediatric Tracheostomy in Taiwan: A Population-Based Survey from 2000 to 2019
Supplemental material, sj-docx-1-ohn-10.1177_19160216241293069 for Trend of Pediatric Tracheostomy in Taiwan: A Population-Based Survey from 2000 to 2019 by Kun-Tai Kang, Chia-Hsuan Lee, Che-Yi Lin and Wei-Chung Hsu in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Acknowledgements
This study was conducted using data from the National Health Insurance Research Database. Thus, we are thankful to the National Health Insurance Administration, the Ministry of Health and Welfare, and the National Health Research Institutes. Notably, data interpretation and conclusions do not represent the opinions of any of the aforementioned institutes. This manuscript was edited by Wallace Academic Editing. The authors would like to thank the anonymous reviewers and the editors for their comments.
Author Note
Some findings from this study were presented at the 2023 Annual Meeting & OTO Experience organized by the American Academy of Otolaryngology—Head and Neck Surgery between September 30 and October 4, 2023, in Nashville, Tennessee, USA.
Author Contributions
K.-T.K. and W.-C.H. conceptualized and designed the study. K.-T.K. and C.-H.L. collected and analyzed the data. K.-T.K. and C.-H.L. drafted the manuscript. C.-Y.L. and W.-C.H. reviewed the manuscript. All authors have read and approved the final version of this manuscript.
Availability of Data and Materials
Raw data in the National Health Insurance Research Database can be requested from the National Health Insurance Administration, Ministry of Health and Welfare, Taiwan. The database is managed by the National Health Research Institutes.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Taipei Hospital, Ministry of Health and Welfare (grant number: 201906), National Taiwan University Hospital (grant number: NTUH. 112-S0226), and Ministry of Science and Technology (grant number: MOST 111-2314-B-002-193-MY3). The funders had no role in study design, data collection or analysis, publication decisions, or manuscript preparation. No additional external funding was received for this study.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Taipei Hospital, Ministry of Health and Welfare, Taiwan (approval number: TH-IRB-0018-0027). Personal data of all patients are deidentified in the National Health Insurance Research Database. Hence, the requirement for informed consent was waived.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.