
Abstract
Background
Conductive or mixed hearing loss with an intact tympanic membrane is a group of diseases characterized by similar clinical symptoms. Definitive diagnosis depends on the findings of exploratory tympanic surgery. Cone-beam computed tomography (CBCT) has great potential for middle ear imaging. This study evaluated the diagnostic value of CBCT for conductive or mixed hearing loss with an intact tympanic membrane.
Methods
CBCT and high-resolution computed tomography (HRCT) imaging data were collected from patients with an intact eardrum who received medical treatment in our hospital for conductive or mixed hearing loss from October 2020 to May 2023. The imaging characteristics and diagnostic values of CBCT and HRCT were analyzed.
Results
A total of 137 patients who met the inclusion criteria and underwent CBCT were enrolled, including 89 with otosclerosis, 41 with ossicular chain interruption, and 7 with tympanosclerosis. CBCT clearly displayed a middle ear focus, such as low-density lesions located in the fissula ante fenestram, ossicular chain malformation or dislocation, and tympanic calcification foci. The area under the curve values for otosclerosis, ossicular chain interruption, and tympanic sclerosis were 0.934, 0.967, and 0.850, respectively. CBCT was more effective than HRCT for visualizing the lenticular process, incudostapedial joint, and stapes footplate.
Conclusions
CBCT of the middle ear demonstrated higher-quality imaging to improve the diagnosis of conductive or mixed hearing loss with an intact tympanic membrane. Therefore, CBCT is recommended for further investigation of noninflammatory diseases of the middle ear with no special findings on HRCT.

Background
Conductive or mixed hearing loss with an intact tympanic membrane is a group of diseases with similar complaints and clinical features, often involving the ossicular chain, including otosclerosis, tympanosclerosis, congenital ossicular chain malformation, and traumatic ossicular chain interruption. Some cases may also be accompanied by a cholesteatoma or inner ear malformation. The main complaint is mostly hearing loss, which may be accompanied by tinnitus. Physical examination shows a normal external auditory canal and intact eardrum. The tympanic immittance diagram shows an A, As, or Ad curve. 1 The preoperative diagnosis is based on the typical history, physical examination, and audiometry results. However, the final diagnosis relies on tympanic exploratory surgery. High-resolution computed tomography (HRCT) is usually performed before ear surgery because it clearly shows temporal bone structures. According to the scanner and protocol, the HRCT scan thickness ranges from 0.4 to 0.8 mm. HRCT is superior for ossicular chain scanning; however, as its utility is affected by resolution, the imaging quality of the stapes requires improvement, especially in patients with tympanic lesions. 2 Thus, radiologists and otologists require more efficient stapes imaging methods to improve the accuracy of preoperative imaging diagnosis of diseases involving the stapes.
Cone-beam computed tomography (CBCT) was developed by Arai and colleagues as a small computed tomography (CT) device for dental application and was first used for the diagnosis and follow-up of oral diseases. 3 CBCT imaging uses a conical X-ray beam to obtain information within the scanning range by rotating 360º. Compared to traditional CT, CBCT has advantages such as a low scanning dose, high spatial resolution, and flexible post-reconstruction. In addition to dentistry, CBCT has been used in head and neck imaging, nasal imaging, and target delineation in conformal radiotherapy.4-6 In their comparative study of CBCT and multi-slice spiral computed tomography (MSCT), Kemp et al. scanned 5 cadavers and reported that compared to MSCT, CBCT had better image quality and a ≥66% lower scanning dose. 7 Our previous comparative analysis of CBCT, HRCT, and micro-CT scans of 15 cadavers showed that stapes imaging with CBCT was superior to that with HRCT, indicating that CBCT could be a candidate for ear imaging in clinical use. 8 Therefore, in the present study, we recruited patients with ossicular chain disease to evaluate the feasibility and effectiveness of CBCT for the diagnosis of conduction or mixed hearing loss with an intact tympanic membrane.
Methods
This study was approved by the Ethics Review Committee of the First Affiliated Hospital of Guangxi Medical University (approval number: 2023-E521-01). From October 2020 to May 2023, patients who underwent CBCT scanning at our center were recruited and their medical history, surgical findings, and HRCT data were collected. The imaging characteristics and findings of the middle ear on CBCT were described, and the diagnostic value of CBCT for patients was evaluated using intraoperative exploration as the gold standard.
Patient Inclusion Criteria
This study enrolled patients who met the following criteria: (1) patients who underwent HRCT and who agreed to undergo CBCT; (2) patients with available CBCT data without motion or metal artifacts; and (3) patients who also underwent exploratory surgery to confirm the final diagnosis.
CBCT and HRCT Scanning Protocols
CBCT was performed using a NewTom ViGo instrument (NewTom, Evo, Italy). The patients’ heads were fixed gently in a bracket while standing. The protocol was as reported by Casselman et al. 9 The specific protocols were as follows: field of view, 15 ×5 cm Hires; tube voltage, 110 kV; tube current, 9.53 to 26 mA; exposure time, 4.3 seconds; scanning time, 18 seconds; thickness, 0.15 mm; and matrix, 1020 × 1020. All imaging data were exported, and NewTom Viewer software (version 10.1.0; NewTom) was used to read the files.
HRCT scanning was performed using a GE CT instrument (LightSpeed VCT XT; GE Healthcare, Chicago, IL, USA) with a pitch of 1.0, tube voltage of 140 kV, tube current of 140 mA, 512 × 512 matrix, spiral time of 1.0 seconds, thickness of 0.625 mm, and scanning time of 4.5 to 5.5 seconds. The image data were saved in the Digital Imaging and Communications in Medicine format and the observation parameters were set to a window width of 4000 and a window level of 700. The imaging terminals were used for file viewing.
Assessment of the Diagnostic Value of CBCT for Conduction or Mixed Hearing Loss with Intact Tympanic Membrane Diseases
The CBCT and HRCT images were reviewed independently by an otologic resident with 5 years of experience (Wenwen Zhou) and an associate chief otologist with 7 years of experience (Lei Liu), who were blinded to the patient’s detailed medical history and audiological findings. The pathological changes observed in the axial coronal position on CBCT were described, including the affected areas and abnormalities in important structures of the middle ear, such as the ossicular chain or the facial nerve. The patients’ HRCT findings were also reviewed to simultaneously describe the positive findings. We designed a checklist for the investigators collecting data to use for interpreting HRCT and CBCT data (Supplemental Table 1). The imaging diagnoses were confirmed by a chief radiologist. If the 2 investigators did not agree on the diagnosis, the final diagnosis was made by the chief physician of the radiology department (Muliang Jiang) after a discussion with the imaging diagnosis team.
All patients underwent microscopic tympanic exploration by 2 authors (Songhua Tan and Anzhou Tang) to identify the final diagnosis and perform artificial ossicular chain reconstruction. The diagnostic values of HRCT and CBCT for conduction or mixed hearing loss in patients with intact tympanic membrane disease were evaluated by comparison with the results of tympanic exploration surgery. The diagnostic rates of HRCT and CBCT were calculated, and the receiver operating characteristic (ROC) curves were plotted for CT-based diagnosis.
Statistical Analysis
RStudio (based on R4.2.1; R Foundation for Statistical Computing, Vienna, Austria) was used for statistical analysis and visualization. The distributions of patient ages are described using means ± standard deviations. The chi-square test was used to compare the diagnostic rates of HRCT and CBCT. The R package “pROC” was used to plot ROC curves. Statistical significance was set at P < .05.
Results
Baseline Patient Information
This study enrolled 137 patients (146 ears) who met the criteria, including 57 men and 80 women, with an average age of 35.38 ± 12.68 years. The patients included 89 with otosclerosis (96 ears), 41 with ossicular chain interruption (43 ears), and 7 with tympanosclerosis (7 ears). Ossicular chain interruption was present in 31 ears with isolated congenital ossicular chain malformation, 6 with congenital cholesteatoma, and 6 with traumatic ossicular chain interruption. Regarding ossicular chain reconstruction, 3 ears underwent ossicular chain relief without a prosthesis, 21 were implanted with a total ossicular replacement prosthesis, 8 were implanted with a partial ossicular replacement prosthesis, 107 were implanted with a piston, 6 were implanted with a CliP Piston (Heinz Kurz GmbH, Dusslingen, Germany) malleovestibulopexy prosthesis, and 1 underwent cochlea implantation.
Characteristics of Healthy Ears in CBCT Imaging
The CT scan and pure tone audiometry outcomes indicated that 29 patients had unilateral involvement. Subsequently, 29 healthy ears were observed using CBCT to determine the normal characteristics of the middle ear. HRCT and CBCT images of the healthy ear are shown in Figure 1.

Axial HRCT and CBCT images of a healthy ear. (A-E) HRCT images of a healthy ear: (A) manubrium layer of the malleus; (B) incudomalleal joint layer; (C) stapes crus layer; (D) footplate layer; (E) layers of the incudomalleal joint and vertical segment of the facial nerve. (F-J) CBCT images of a healthy ear. (F) manubrium layer of the malleus; (G) incudomalleal joint layer; (H) stapes crus layer; (I) footplate layer; and (J) layers of the incudomalleal joint and vertical segment of the facial nerve.
Characteristics of Conductive or Mixed Hearing Loss Ears with Intact Tympanic Membrane in CBCT Imaging
CBCT of patients with otosclerosis showed low- or mixed-density sclerosis foci in the fissula ante fenestram, pericochlea, and footplate (Figure 2). According to the location of the foci, the patients were divided into those with fissula ante fenestram type (70 cases), which only presented as isolated foci in the fissula ante fenestram (Figure 2A and B), and mixed type (13 cases), with foci found in both the fissula ante fenestram and pericochlear area (Figure 2C), including 4 cases with the typical “double ring sign” (Figure 2D) and 2 cases of occlusive otosclerosis with “biscuit footplate” (Figure 2E). According to the audiological results and intraoperative findings combined with the CBCT manifestations, the patients were divided into 85 and 4 cases of active and inactive otosclerosis, respectively (Figure 2F). In inactive cases, preoperative CBCT showed non-abnormal foci in the fissula ante fenestram, footplate, pericochlea, round window, semicircular canal, or internal auditory canal. Ossicular chain malformations, dislocations, or tympanosclerosis were excluded during exploratory surgery, and the final diagnosis was otosclerosis (inactive phase). In addition, CBCT of 2 non-surgical ears without hearing loss showed sclerotic foci in the fissula ante fenestram, thus confirming subclinical otosclerosis.

CBCT imaging of otosclerosis. (A) Fenestral otosclerosis: isolated low-density foci in the fissula ante fenestram (arrow); (B) fenestral otosclerosis: isolated mixed-density foci in the fissula ante fenestram (arrow); (C) fenestral and cochlea otosclerosis: low-density foci in the fissula ante fenestram involving the cochlea (arrow); (D) typical “double ring sign” (white arrow: foci in the fissula ante fenestram; red arrow: foci around the cochlea); (E) biscuit footplate of obliterative otosclerosis (arrow); and (F) inactive otosclerosis.
Figure 3 shows the typical CBCT findings in patients with partial ossicular chain interruption or tympanosclerosis. Patients with isolated ossicular chain malformations exhibited a partial absence of the ossicular structure, often observed in the long process of the incus, lenticular process, and stapes crus. Among patients with congenital cholesteatoma, 4 ears showed abnormal soft tissue density in the tympanic cavity, with 2 ears showing new bone formation in the tympanic cavity. In this study, patients with ossicular chain dislocation had a history of trauma, with the incudostapedial joint being the most affected. Patients with tympanosclerosis showed abnormal calcification in the tympanic cavity or membrane, which could wrap around the ossicles and cause ossicular chain fixation.
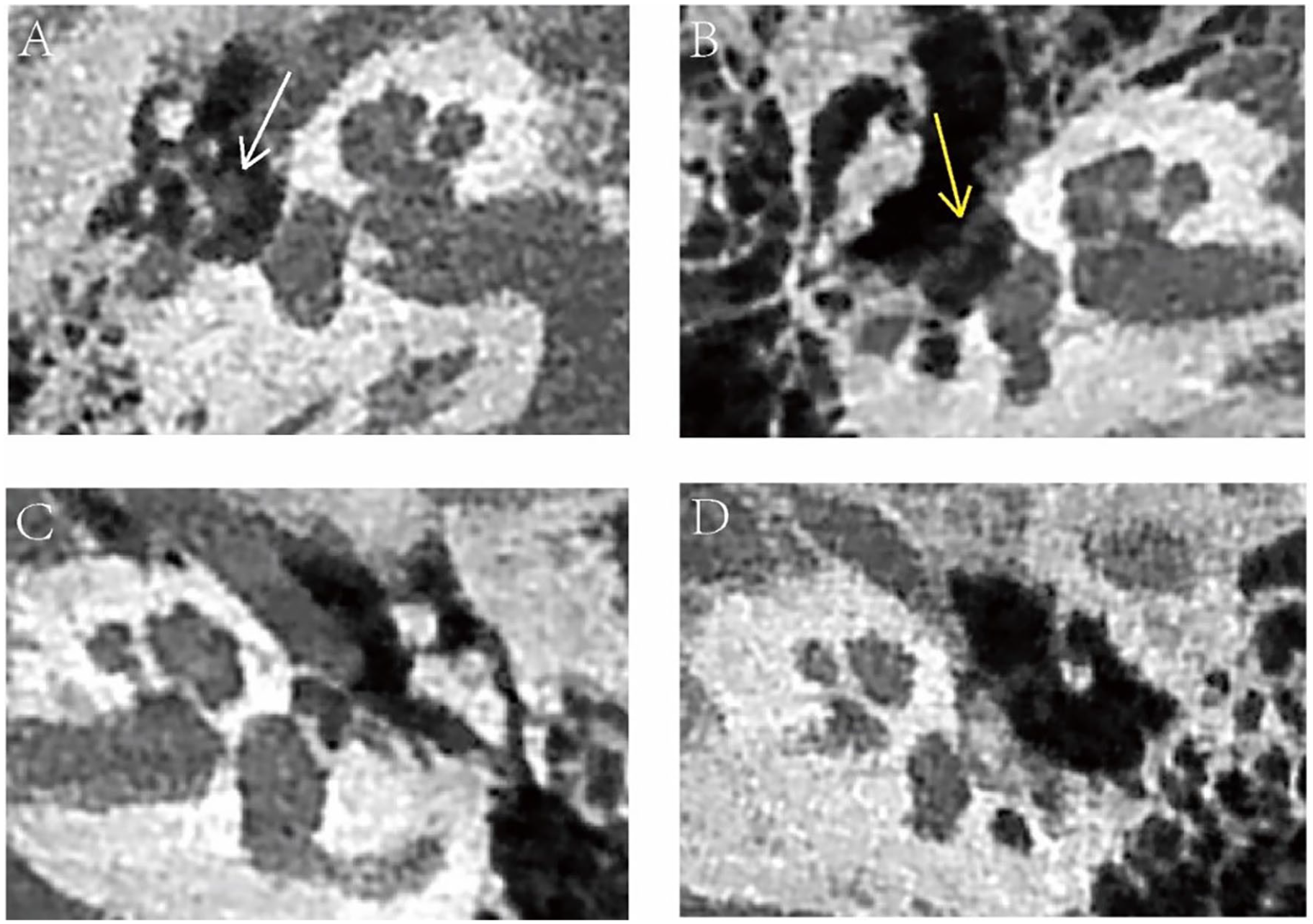
CBCT imaging of ossicular chain interruption and tympanosclerosis. (A) Congenital cholesteatoma with ossicular chain malformation: soft tissue in the tympanic cavity (white arrow); (B) isolated ossicular chain malformation: the long process is absent, with the facial nerve hanging above the footplate (yellow arrow); (C) dislocation of the incudomalleal joint; and (D) tympanosclerosis: the stapes crus is absent and replaced by high-density and irregularly shaped tympanic sclerosis lesions.
Diagnostic Efficacy of CBCT in Ears with Conductive or Mixed Hearing Loss and Intact Tympanic Membranes
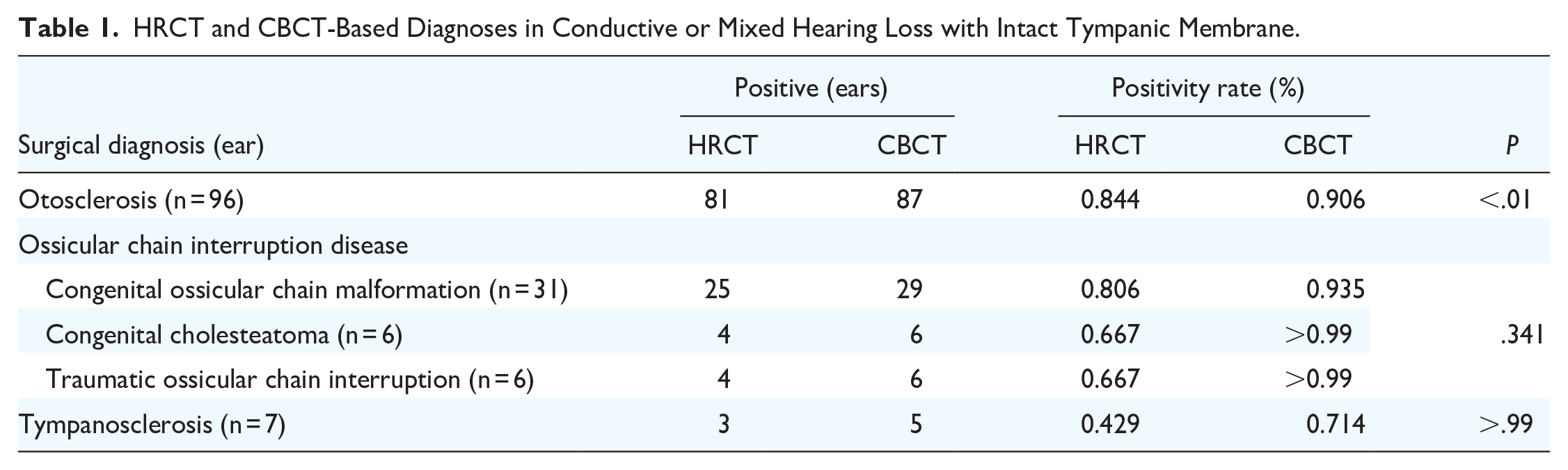
The kappa coefficients of the imaging diagnosis result between the 2 investigators indicated a good consistency, with values of >0.75 (Supplemental Table 2). Table 1 presents the CT results and positive diagnoses for 137 patients. CBCT showed a high positive diagnostic rate for otosclerosis, ossicular chain interruption disease, and tympanosclerosis. We observed a statistically significant difference in the diagnostic rate of otosclerosis for CBCT compared to HRCT (P < .01).
HRCT and CBCT-Based Diagnoses in Conductive or Mixed Hearing Loss with Intact Tympanic Membrane.
The results of diagnostic efficacy analysis of HRCT and CBCT for the diagnosis of otosclerosis, ossicular chain interruption disease, and tympanosclerosis showed that CBCT had better diagnostic efficacy than HRCT in the diagnosis of ossicular chain interruption disease (Table 2, P = .018).
Diagnostic Efficacy of HRCT and CBCT in Otosclerosis, Ossicular Chain Interruption Disease, and Tympanosclerosis.

Abbreviations: AUC, area under the curve; CBCT, cone-beam computed tomography; CI, confidence interval; HRCT, high-resolution computed tomography.
Table 3 shows the diagnostic rates of each site using HRCT and CBCT for ossicular chain interruption diseases involving multiple ossicles or ossicular joints.
HRCT and CBCT-Based Diagnoses in Cases with Ossicular Chain Interruption Diseases Involving Multiple Ossicles or Ossicular Joints.

Abbreviations: CBCT, cone-beam computed tomography; HRCT, high-resolution computed tomography.
Further analysis of the diagnostic efficacy of HRCT and CBCT was performed at sites with significant differences in diagnostic rates, such as the lenticular process, incudostapedial joint, stapes crus, and footplate. The results showed that the diagnostic efficacy of CBCT was superior to that of HRCT for the lenticular process, incudostapedial joint, and footplate (P < .05; Table 4). The ROC curves are shown in Figure 4.
Diagnostic Efficacy of HRCT and CBCT for the Stapes and Circumambient Structures.
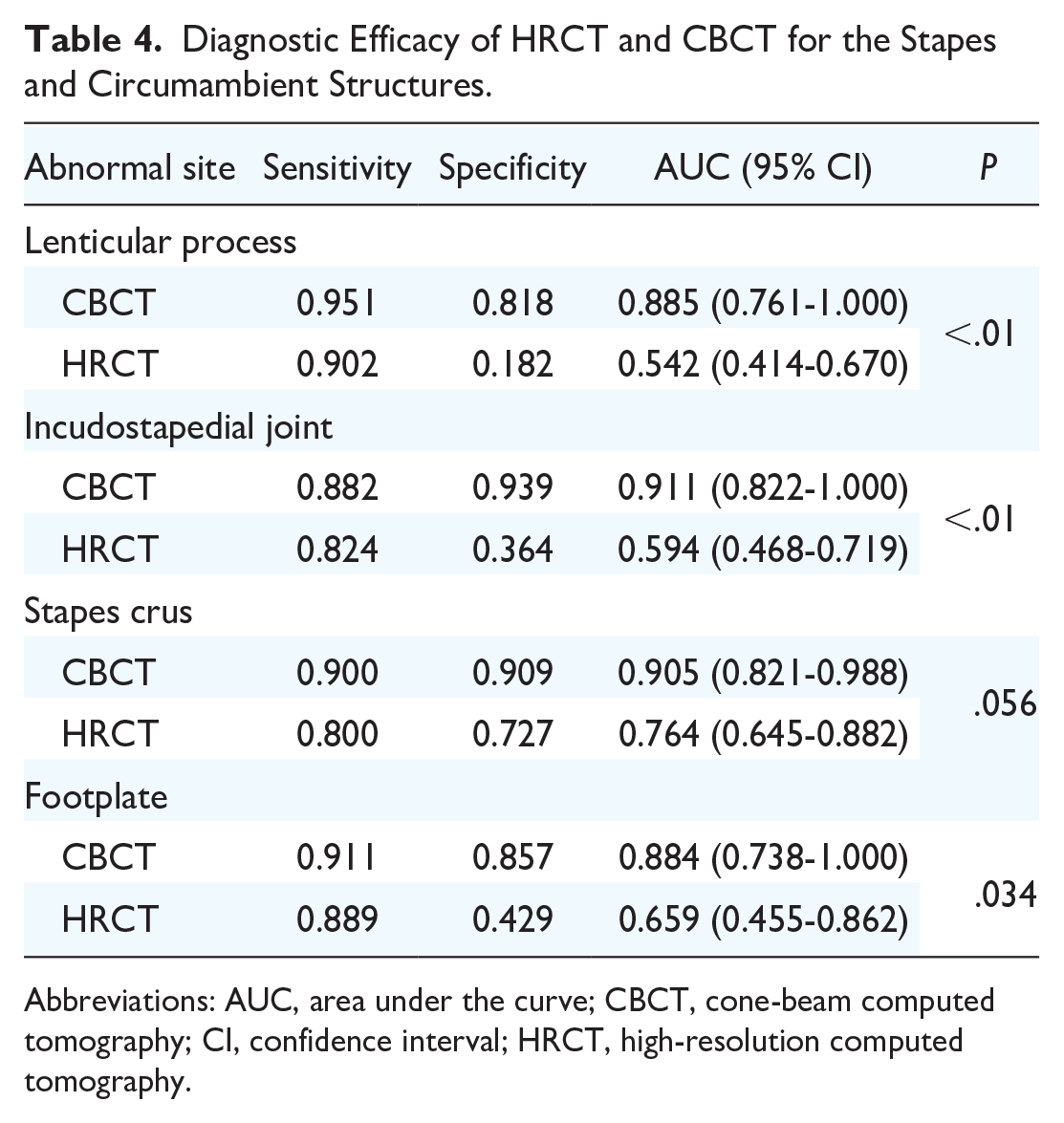
Abbreviations: AUC, area under the curve; CBCT, cone-beam computed tomography; CI, confidence interval; HRCT, high-resolution computed tomography.

ROC curves of the efficacy of diagnosis by HRCT and CBCT. ROC curves of the lenticular process (A), incudostapedial joint (B), and footplate (C).
Discussion
The temporal bone contains the external, middle, and inner ear. Temporal bone HRCT is a non-invasive tool used to comprehensively evaluate anatomical characteristics and diseases. HRCT can reveal the involvement of the ossicular region and allow the formulation of individualized surgical plans. HRCT is also an optional follow-up examination performed after ear surgery. Patients may require HRCT after middle ear surgery due to prosthetic failure, cholesteatoma recurrence, or inflammation. 10 Otologists may be cautious about HRCT during follow-up because of the radiation dose and medical costs. 11 However, the radiation dose for CBCT is only 1/10 to 1/3 that of HRCT, and the medical costs are reduced by 1/2 to 2/3, which is a significant advantage for follow-up after ear surgery.12,13
In ear imaging, the disadvantages of CBCT scans include motion artifacts and non-uniform observational conditions. In our study, the patients were mostly in a standing or sitting position during the CBCT examination. Motion artifacts may occur if the head cannot be held still, especially in children and the elderly. Walliczek et al. found that approximately 3.7% of children undergoing CBCT must be rescanned because of motion artifacts. 14 Fixation devices can help reduce unnecessary radiation exposure caused by motion artifacts. 15 In addition, while the use of CBCT in ear imaging is increasing, scanning protocols and standard observational layers have not yet been unified. Based on the existing literature and our imaging findings, the CBCT scan protocol for the temporal bone has been proven feasible. 9 Regarding the important observation layers in HRCT, CBCT has shown excellent middle and inner ear imaging.
We previously demonstrated that CBCT was superior for the assessment of bony structures, such as the ossicles and ossicular joints, but inferior for the evaluation of the cochlear axis, bone spiral plates, and basement membrane. 8 Compared to HRCT, CBCT has a low resolution in soft tissue, indicating that CBCT may be inadequate for the diagnosis of inner ear malformations, such as type II incomplete cochlear partition. 16 Since most of the patients undergoing cochlear implantation in our tertiary center are children aged <5 years who cannot successfully complete CBCT scanning while standing without motion artifacts, additional data are needed to demonstrate the value of CBCT in the diagnosis of inner ear malformation.
Conductive or mixed hearing loss with intact tympanic membrane diseases, including otosclerosis, ossicular chain malformations (which can also accompany inner ear malformations), ossicular chain interruption, tympanosclerosis, and congenital cholesteatoma, is sometimes difficult to diagnose using HRCT. 17 The diagnostic sensitivity of the HRCT axial plane for otosclerosis varies and its accuracy improves after stapes multiplane reconstruction.18-20 Redfors et al. previously reported that CBCT is equivalent to MSCT for otosclerosis diagnosis and is a candidate radiological tool. 21 In the present study, we found that CBCT was very sensitive to active otosclerotic foci in the stapes crus, footplate, and fissula ante fenestram. Even tiny foci with negative HRCT findings can appear as low- or mixed-density areas. Within the cohort of patients with otosclerosis in the present study, while CBCT of 9 ears was negative, these cases were ultimately diagnosed with inactive otosclerosis based on history and intraoperative findings. The inactive stage of otosclerosis showed no abnormal bone absorption or remodeling, and the bone had the same density as the surrounding labyrinthine bone. Therefore, imaging diagnosis is difficult regardless of whether HRCT or CBCT is used. A combination of medical history and intraoperative exclusion of malformations or inflammation is often required to reach a final diagnosis. Our comparison of the positivity rates between HRCT and CBCT showed that CBCT was significantly more sensitive for the diagnosis of otosclerosis. The results of a subsequent ROC curve analysis incorporating ossicular chain interruption and tympanosclerosis showed no statistically significant differences in the diagnostic efficacies of HRCT and CBCT for the diagnosis of otosclerosis. The inconsistent results of the positive rate comparison and ROC analysis indicate that HRCT and CBCT have similar diagnostic efficacies in otosclerotic diseases; both can effectively exclude non-otosclerosis cases, while CBCT is more sensitive in positive cases.
Ossicular chain interruption includes congenital or acquired causes mainly caused by trauma or otitis media. Interruption can occur at any site of the ossicular chain, either in the ossicular or ossicular joints. Furthermore, patients with congenital ossicular chain malformations with moderate-to-severe mixed hearing loss may also have inner ear malformations; thus, caution is required during artificial ossicular reconstruction to avoid fatal sensorineural deafness. 22 HRCT can reveal not only ossicular abnormalities but also those of the facial nerve or inner ear. 23 Zhang et al. demonstrated the inefficiency of HRCT for ossicular chain malformation diagnosis, with a sensitivity of only 62.1%, with stapes anomalies with or without an incus anomaly the most frequent occurrences. 24 We defined the final diagnosis as positive if at least one abnormality in the ossicular chain site was detected on HRCT. In addition to determining the final diagnosis, we analyzed the positivity rates for different malformation sites by HRCT and CBCT. The results showed that the diagnostic efficacy of CBCT was superior to that of HRCT in the diagnosis of malformations of the lenticular process, incudostapedial joint, and footplate. Malformations were more likely to occur in the long process of the incus and stapes. Thus, incus and stapes images collected by CBCT can be used to properly identify malformations and inform the selection of appropriate prostheses.
Traumatic ossicular chain interruptions include ossicular dislocation and fracture. Dislocation often occurs in the incudostapedial or incudomalleal joints, while footplate dislocation is rare. Fractures can involve the stapes crus or the long process of the incus. 25 While total luxation or fracture is easy to diagnose based on trauma history and typical CT imaging, subluxation of the ossicle or joint may be missed on CT. In this cohort, a patient with mild conductive hearing loss whose coronal HRCT showed a roughly normal incudomalleal joint, while coronal CBCT showed suspected subluxation was confirmed during tympanic exploration surgery. The diagnosis of ossicular joint subluxation is challenging using CT, and multiplanar or curved reconstruction can help achieve a positive diagnosis. 26
Among the sequelae of otitis media, tympanosclerosis and cholesterol granulomas are characterized by hearing loss with an intact tympanic membrane. HRCT findings in patients with tympanosclerosis include high-density calcification in the tympanic membrane or cavity, which can wrap around the ossicle or ossicular joint. Larem et al. reported the effectiveness of HRCT in the diagnosis of ossicular tympanosclerosis, with a sensitivity of 96.8% and a specificity of 98%, which were higher than those in the present study. 27 However, our study included only a few cases of tympanosclerosis and more cases must be collected to clarify the diagnostic advantages of CBCT. Thicker scans or multiplanar reconstructions should be conducted if the sclerosis only wraps around the incudomalleal joint, stapes crus, or footplate, as minute sclerosis is often omitted.
This study evaluated the imaging manifestations of CBCT in healthy ears and ears with conductive or mixed hearing loss with intact tympanic membranes and comprehensively appraised the diagnostic value of CBCT for otosclerosis, ossicular chain interruption, and tympanosclerosis. However, this study was limited by the unbalanced number of different cases. More cases of tympanosclerosis and congenital cholesteatoma must be recruited to further confirm the value of CBCT imaging.
Conclusions
CBCT scanning of the middle ear provides higher-quality imaging for a better diagnosis of conductive or mixed hearing loss with an intact tympanic membrane. Therefore, CBCT is recommended for further diagnosis of noninflammatory diseases of the middle ear with no special findings on HRCT.
Supplemental Material
sj-docx-1-ohn-10.1177_19160216241272384 – Supplemental material for Diagnostic Value of Cone-Beam Computed Tomography in Conductive or Mixed Hearing Loss with Intact Tympanic Membrane
Supplemental material, sj-docx-1-ohn-10.1177_19160216241272384 for Diagnostic Value of Cone-Beam Computed Tomography in Conductive or Mixed Hearing Loss with Intact Tympanic Membrane by Wenwen Zhou, Lei Liu, Di Liu, Muliang Jiang, Guixing Chen, Anzhou Tang and Songhua Tan in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Acknowledgements
We are grateful to the physicians and staff of the Department of Otorhinolaryngology—Head and Neck Surgery of the First Affiliated Hospital of Guangxi Medical University, and the staff and Dr. Xianfang Jiang of the Radiology Department of Guangxi Stomatology Hospital for technical support. Finally, we thank Editage (![]() ) for English language editing.
) for English language editing.
Authors’ Contributions
Wenwen Zhou: Methodology, Data Curation, Writing—Original Draft; Lei Liu: Writing—Review and Editing; Di Liu: Visualization, Investigation; Muliang Jiang: Technical consultation; Guixing Chen: Investigation; Anzhou Tang: Project Administration; Songhua Tan: Funding acquisition.
Availability of Data and Materials
Not applicable.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The authors have no financial relationships or conflicts of interest to disclose.
Funding
This work was supported by the Guangxi Medical and Health Appropriate Technology Development and Application Project (Grant No. S201661).
Ethics Approval and Consent to Participate
This study was approved by the Ethics Review Committee of the First Affiliated Hospital of Guangxi Medical University (approval number: 2023-E521-01)
Sponsorship
None.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.