
Abstract
Background
This study aimed to explore the impacts of different middle-ear mucosal conditions on the outcomes of type I tympanoplasty.
Methods
A retrospective analysis of 164 patients with chronic otitis media was carried out. The patients were divided into 4 groups according to their mucosal condition. Preoperative hearing levels and air-bone gap (ABG) before and after surgery were compared via the Kruskal‒Wallis H test. The chi-squared test and Fisher’s exact test were used to assess the postoperative complications and impact factors of functional success.
Results
Preoperatively, neither the air conduction nor bone conduction values differed significantly among groups with different mucosal conditions. All of the ABG closed dramatically after type I tympanoplasty (P < .05) regardless of the mucosal conditions. The functional success rates were lower when the intratympanic mucosa was moderately or severely edematous compared with mildly edematous or normal (P < .05). The disease course, perforation site, and perforation size, as well as the status of the opposite ear, were not related to the auditory functional outcome. The differences in postoperative reotorrhea and reperforation among the 4 groups were not statistically significant.
Conclusion
Preoperative hearing levels were not affected by middle-ear mucosal conditions. The functional success rate was influenced by mucosal conditions, but hearing levels were significantly enhanced after surgical intervention regardless of the mucosal status. Postoperative complications were not related to the mucosal conditions. Thus, type I tympanoplasty is adoptable for mucosal abnormalities when pharmacotherapy cannot result in a healthy tympanum.

Introduction
Patients with chronic otitis media (COM) commonly have otorrhea or an abnormal tympanic mucosa when they visit an outpatient clinic. Sometimes, these conditions cannot be improved after strictly conservative treatment. Hence, numerous studies have investigated whether tympanoplasty can be implemented for unhealthy conditions and have reported comparisons of surgical outcomes between normal and abnormal tympanic statuses.1-3 In particular, the impact of inflammatory mucosal conditions and promontory granulomas on surgical outcomes remains controversial among otologists.1,4,5 The mucosal condition mostly reflects the ventilation efficiency of the middle ear and mastoid cells. Mucosal hypertrophy, edema, and granulation may predict eustachian tube dysfunction (ETD) or active inflammation. A study reported that the audiologic levels are seemingly poorer in middle ears with mucosal swelling or granulation tissue than in those with a normal mucosa. 6 An abnormal middle ear mucosa may weaken the preoperative audiologic levels and even affect the postoperative outcomes of tympanoplasty. Some researchers have found that abnormal mucosa or ventilation may lower the success rate of tympanoplasty and further affect the long-term outcome.1,4,6 In contrast, numerous reports have stated that removing abnormal mucosa promotes hearing recovery.7,8 However, the severity of the middle-ear mucosal abnormality, invasion of the ossicle chain, and surgical methods were different in these studies. Hence, we attempted to compare the impacts of different grades of mucosal conditions of the middle ear on the outcomes of type I tympanoplasty. This would be beneficial for otologists in decision-making regarding therapeutic schedules when confronting mucosal abnormalities.
Materials and Methods
Study Design and Grouping
A retrospective analysis of 164 patients treated for COM between May 2015 and July 2022 in the Department of Otorhinolaryngology at Xijing Hospital (Air Force Military Medical University) was conducted. All patients underwent type I tympanoplasty. Demographic information and medical record data, including the disease course, surgical ear, perforation size and site, and opposite ear condition, were collected. This research was approved by the Medical Ethics Committee of the First Affiliated Hospital of the Air Force Medical University (No. KY20222123-C-1).
The patients had to meet the following inclusion criteria: age ranging from 16 to 55 years, mild-to-moderate conductive hearing loss, eardrum with pars tensa perforation, and bilateral ears without previous otologic surgery. Patients with ossicular erosion, a diagnosis of adhesive otitis media, eosinophilic otitis media, cholesteatoma, tympanosclerosis or other middle-ear diseases were excluded.
According to the status of the tympanic mucosa and residual tympanic membrane, the subjects were divided into 4 groups: (1) healthy group without mucopurulent discharge; (2) mildly edematous group with an intratympanic mucosal thickness less than 1 mm and with mucoid or mucopurulent discharge; (3) moderately edematous group with an intratympanic mucosal thickness of more than 1 mm but not appearing beyond the residual tympanic membrane; and (4) severely edematous group, in which the intratympanic mucosal thickness or hyperplastic granulation was outside the residual tympanic membrane (Figure 1). During surgery, a House measuring rod with a 1 mm head combing a suction tube with a 1 mm diameter was used to measure the mucosal thickness of the promontory.

Otoscopic images of representative patients in the 4 groups. (a, b) Preoperative and postoperative images of the same patient in Group 1. (c, d) Preoperative and postoperative images of the same patient in Group 2. (e, f) Preoperative and postoperative images of the same patient in Group 3. (g, h) Preoperative and postoperative images of the same patient in Group 4.
Surgical Techniques
All operations were conducted under general anesthesia through a postauricular approach and completed successfully. The temporalis fascia was harvested as graft material and shaped according to the perforation size. The underlay technique was used for the grafting procedure. Gelatin sponges soaked with 1% adrenaline were used to retract the swollen middle-ear mucosa in all patients. The hyperplastic granulation tissues were resected at the level of the normal intratympanic mucosa, and in all cases, biopsy of the granulation tissues ruled out tubercular and other lesions. All procedures were conducted by 1 senior otologist, Dr Chen, who had performed at least 2000 tympanoplasties.
Follow-Up and Outcome Evaluation
All patients underwent pure tone audiometry (PTA) and otoscopy tests and were followed up every 1 to 3 months. The preoperative and postoperative audiometric levels were evaluated by PTA at 0.5, 1, 2, and 4 kHz before and 12 months after surgery. Graft success was defined as an intact graft without perforation, retraction, or lateralization 12 months after surgery. The air-bone gap (ABG) was calculated as the average difference between the air conduction (AC) and bone conduction (BC) thresholds at the 4 frequencies. The ABG gain was calculated as the preoperative ABG minus the postoperative ABG. An ABG ≤20 dB was accepted as functional success. 9
Statistical Analysis
All data were analyzed using SPSS 26.0 software (SPSS Inc., Chicago, IL). The results are presented as the mean ± standard deviation. Quantitative data were analyzed using 1-way analysis of variance. Count data were assessed by using the chi-square test. The Kruskal‒Wallis H test was used to compare the differences in preoperative audiometric levels and preoperative and postoperative ABG among the 4 groups. The chi-squared test and Fisher’s exact test were used to analyze the impact factors of functional success and postoperative outcomes. Differences were considered statistically significant if the P value was less than .05.
Results
One hundred and sixty-four enrolled patients were classified into four groups based on their intratympanic mucosal condition. The disease course was subdivided into 2 categories: more than 5 years and less than 5 years. The clinical characteristics are displayed in Table 1, and there were no significant differences among these groups. The follow-up was over 1 year for all patients (Table 1).
Comparison of Clinical Characteristics.

Table 2 displays the preoperative and postoperative audiometry levels. Neither the BC nor the air conduction threshold significantly differed among the 4 groups. Preoperatively, the ABG values among the 4 groups were not statistically significant. All 4 groups achieved significant improvement after type I tympanoplasty (P < .05).
Comparison of Preoperative and Postoperative Audiometric Levels.

Abbreviations: ABG, air-bone gap; AC, air conduction; BC: bone conduction.
Table 3 demonstrates the related impact factors of auditory function in type I tympanoplasty. The mucosal conditions were found to have significantly influenced the functional success (postoperative ABG ≤20 dB) or failure rate (postoperative ABG >20 dB, P < .05). However, factors including disease course, perforation site and size, and the condition of the opposite ear did not exert dramatic effects on hearing improvement.
Factors Affecting Functional Success.
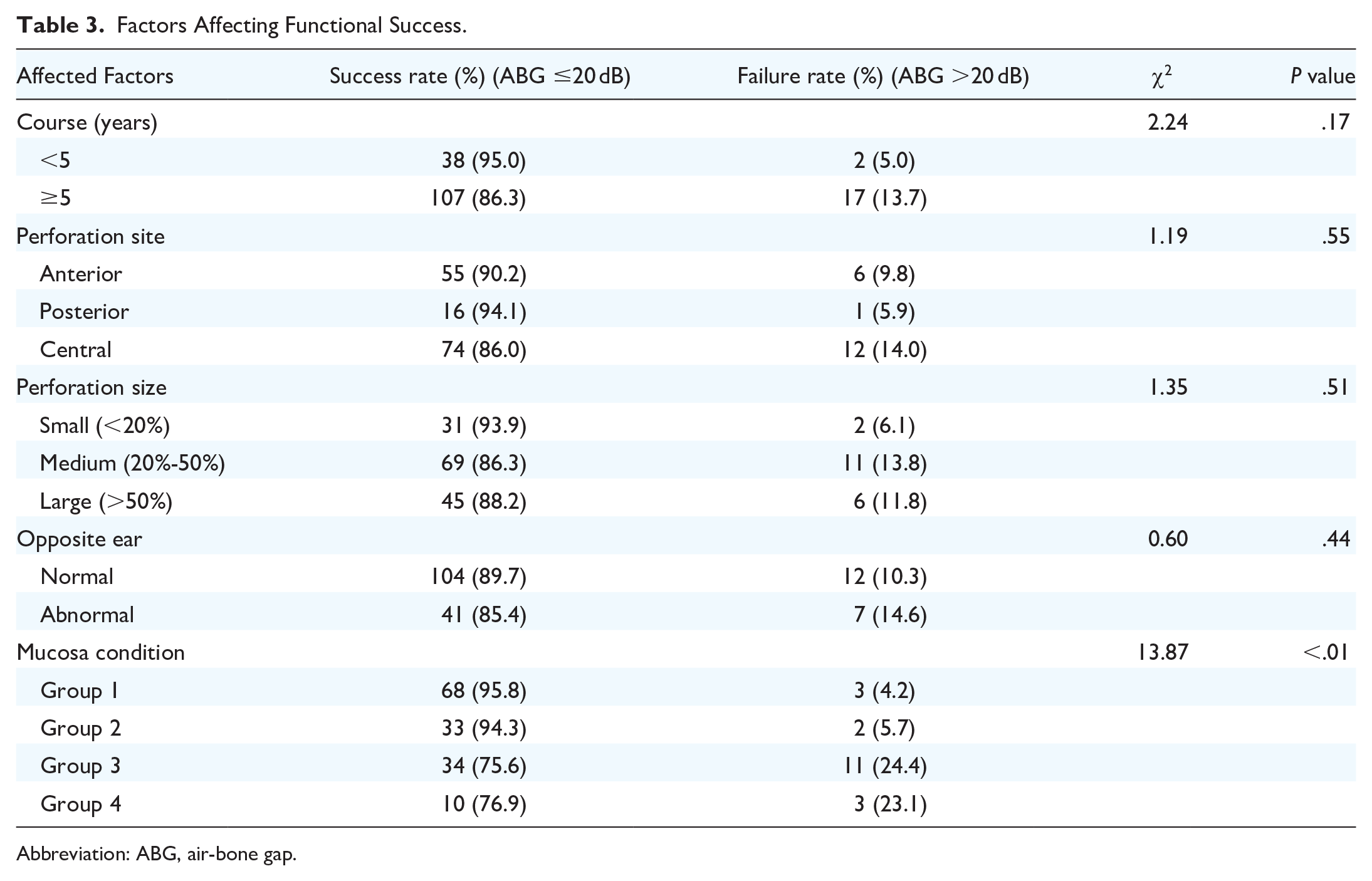
Abbreviation: ABG, air-bone gap.
Table 4 shows the common postoperative complications, including reotorrhea and reperforation. Although both reotorrhea and reperforation occurred frequently in Group 3 and Group 4, the differences among these 4 groups were statistically insignificant.
Postoperative Complication Among Four Groups.

Discussion
There has been great controversy regarding the impacts of inflammatory or abnormal middle-ear mucosal conditions on tympanoplasty outcomes. However, in these reports, either the mucosal abnormalities were confused with discharge, or no further investigation according to the different abnormalities was conducted.1,2 In this study, only type I tympanoplasty and mucosal status were involved. The assessment and classification of mucosal conditions promote an understanding of the various effects on different abnormalities. This will contribute to precise administration of COM, especially in drug refractory cases.
Surgical intervention is a candidate treatment for these cases, but it may be postponed by opponents. Song obtained a better postoperative audiologic outcome with a healthy middle-ear mucosal condition than with an abnormal condition. 1 They attributed this finding to the favorable gas exchange of the middle-ear mucosa and eustachian tube in normal conditions. 1 Mucosal abnormalities may indicate insufficient ventilation or active inflammation in the middle ear.1,3 However, numerous studies presented the opposite opinion. Those researchers claimed that ETD did not adversely affect the outcomes of type I tympanoplasty. They concluded that surgery could exert a positive influence, such as by eradicating the diseased mucosa and mucous plugs to restore the ventilation and pressure of the middle ear.3,10,11 Li et al demonstrated that after type I tympanoplasty, the eustachian tube score assessed by tubomanometry (TMM) was significantly improved in patients with ETD. 10 In the current study, the postoperative ABG closed significantly in every group regardless of the mucosal status. This may have been due to relieving the adverse effects of mechanical blockage and inflammatory mediators through surgical intervention. The inflammatory environment invites mucosal swelling and granulation tissue formation. It may deteriorate ventilation and drainage of the middle ear, which may contribute to anaerobes growing concurrently with aerobes. 12 Pharmacotherapy cannot exert an effective role in this condition. In view of these reasons, type I tympanoplasty is helpful for eliminating this unhealthy cycle of mucosal abnormalities. During surgery, mucopurulent discharge and eustachian tubes are rushed, abnormal mucosa or granulation tissue is managed, and the tympanic membrane is repaired. These operations are conducive to recovering the function and structure of the middle ear.
In this study, the difference in the functional success rate between the healthy condition and the mildly edematous mucosa had no statistical significance. However, the functional failure rate was higher in moderate or severe conditions than in normal or mildly edematous mucosal conditions. These hearing outcomes were generally in accordance with Song’s conclusion: the better the condition of the middle ear, the better was the postoperative hearing improvement. 1 The potential reasons for lower success rates in moderate or severe conditions are as follows: First, we suspected that some innate immunity-related factors may be involved. Type I tympanoplasty removes the edematous mucosa caused by immunoreaction, but this reaction may persist postoperatively and prolong the functional recovery of the tympanic cavity. Second, Minami reported that alteration of the middle-ear microbiome may cause the pathogenesis of COM with active inflammation. 12 Additionally, a review showed that viral/bacterial coinfections in the middle ear are more common than bacterial infections alone. 13 This infection or innate immunity change in the middle-ear mucosa not only may lead to refractory COM but also can seem to extend postoperative recovery. Further investigation of these mechanisms and pathogenesis is worth conducting and will facilitate the treatment of intractable COM.
Given these hearing-related outcomes of our study, pharmacotherapy for diseased mucosal conditions and otorrhea is still recommended. After this regular treatment, most diseased conditions dramatically improve. However, a few intractable cases cannot obtain a satisfying outcome. These cases commonly involve frequent recurrence of active inflammation without an interval for surgery and the presence of granulation hyperplasia or severe polyps. Type I tympanoplasty is proposed for such cases of intractable COM. Moreover, adequate preoperative communication with patients is indispensable for ensuring reasonable expectations.
Reotorrhea and reperforation are the most common complications of type I tympanoplasty. Lee revealed that the incidence of postoperative otorrhea was higher in patients with a preoperative wet middle-ear mucosa than in those with a dry ear. 14 Many reports have illustrated that active inflammation does not lower the graft success rate and even contributes to the vascularization of grafts.14,15 In this study, the rates of reotorrhea and reperforation were higher in moderate or severe edematous conditions than in normal or mildly edematous conditions, but these differences were not statistically significant. This evidence further supports the idea that type I tympanoplasty is available for mucosal abnormalities. This approach is conducive to shortening the pharmacotherapy duration and reducing surgery postponement.
Other prognostic factors of type I tympanoplasty have also sparked discussion among researchers. They include age, disease course, size and site of the perforation, grafting materials, surgical technique, otologist experience, and status of the opposite ear. In the current study, all of the operations were conducted by 1 senior otologist using an underlay technique with temporalis muscle fascia, and the ages of the patients ranged from 16 to 55 years. Consistent with some other studies, this study also showed that there was no relationship between the perforation site and hearing improvement over the follow-up periods.4,16 A study revealed a decreased chance of graft uptake and hearing improvement when the otorrhea duration was more than 5 years. 17 However, an identical effect of disease course was not observed in this study. Mills reported that operations on larger perforations have a lower success rate than operations on smaller perforations. 2 This study was in agreement with Deosthale’s conclusion that perforation size does not affect functional success. 18 An abnormal opposite ear was identified as a negative prognostic factor because it indicates ETD. 19 As TMM developed, it is used for quantitative measurement of eustachian tube function. Li et al found that ETD did not reduce the success rate of type I tympanoplasty as assessed by TMM. 10 Similarly, our results suggested that an abnormal opposite ear would not lower the functional success rate.
Until now, an objective grading system for the tympanic mucosa has been absent. Berg et al supposed that measuring the middle-ear mucosa using spectroscopic techniques is still in an experimental stage. 20 In our study, the subjects were roughly classified into 4 groups based on middle-ear status. This classification method would prevent the disordered management of discharge, swelling, and granulation. It would also be helpful for decision-making and communication with patients with different abnormalities. In the future, a quantitative standard for mucosal abnormalities is necessary. The pathological mechanisms for edematous mucosal conditions need to be further illustrated. Additionally, cases of severe granulation were uncommon. A larger-scale sample would produce a stronger study.
Conclusion
Mucosal abnormalities were further classified based on the thickness of the intratympanic mucosa. The mucosal conditions were found to have significantly influenced the postoperative functional success. However, the postoperative hearing outcomes improved significantly regardless of the mucosal status. Tympanoplasty itself provided a considerable curative opportunity for refractory COM patients who were unresponsive to conservative treatment. Mucosal conditions were not related to postoperative complications. For these reasons, type I tympanoplasty is adaptable for mucosal abnormalities when pharmacotherapy cannot exert a positive outcome. Disease course, perforation site and size and opposite ear status did not affect the functional outcomes of type I tympanoplasty.
Footnotes
Acknowledgements
None.
Author Contributions
The study was designed by YC, and all of the operations were conducted by him. Y.H., R.Y. and X.M. collected data and wrote this manuscript. R.L. and Y.S. performed the statistical analysis. H.S., Y.F. and X.A. participated in the patient follow-up. Some suggestions were provided by D.Z. All authors performed data interpretation and approved the manuscript.
Availability of Data and Materials
The datasets are available from the corresponding author upon reasonable request.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by grants from the National Natural Science Foundation of China (81870719), the Foundation of Shaanxi Province (2023-YBSF-209), Teaching Reform Research Project of Air Force Medical University (KJJYDXYB025), and Xijing Hospital Promotion Project (XJZT21CM10). The funder was supported by Y.H. The funder had no role in the study design; collection, analysis, or interpretation of the data; or the manuscript preparation.
Ethics Approval and Consent to Participate
This research was approved by the Medical Ethics Committee of the First Affiliated Hospital of the Air Force Medical University (No. KY20222123-C-1).