
Abstract
Background
In the emergency department (ED), there are pre-assembled tonsillar hemorrhage trays for management of post-tonsillectomy hemorrhage and peritonsillar abscess. After use, the tray is sent to the medical device reprocessing (MDR) department for decontamination, sterilization, and re-organization, all at a significant cost to the hospital and environment.
Objective
The goal of this project was to reduce unnecessary instruments on the tonsil hemorrhage tray by 30% by 1 year and report on the associated cost and carbon dioxide (CO2) emissions savings.
Methods
This quality improvement project was framed according to the Institute for Healthcare Improvement’s Model for Improvement. ED and Otolaryngology–Head & Neck Surgery staff and residents were surveyed to determine which instruments on the tonsil hemorrhage trays were used regularly. Based on results, a new tray was developed and compared to the old tray using MDR data and existing CO2 emissions calculations.
Results
Tray optimization resulted in a total cost reduction from $1092.63 to $330.21 per tray per year, decreased processing time from 12 to 6-8 minutes per tray, and decreased CO2 emissions from 6.11 to 2.85 kg per year for the old versus new tray, respectively. Overall, the new tray contains half the number of instruments, takes half the time to assemble, produces 50% less CO2 emissions, and will save the hospital approximately $100,000 over 10 years.
Conclusion
Healthcare costs and environmental sustainability are collective responsibilities. Surgical and procedure tray optimization is a simple, effective, and scalable form of eco-action.

Keywords
Background
Common emergency department (ED) visits for tonsillar complaints include post-tonsillectomy hemorrhage and peritonsillar abscess (PTA). Risk of post-tonsillectomy hemorrhage is quoted at 3%-5%, with 1% requiring surgical control. 1 When a patient presents to the ED, it is imperative that both emergency physicians and otolaryngologists have the correct instruments to assess the tonsillar fossa, stop the hemorrhage, and/or temporize the bleed while awaiting set up of the operating room (OR). PTAs are the most common deep infection of the head and neck, 2 with a reported incidence of 10 to 37 per 100,000 people worldwide. 3 Management includes antibiotics, aspiration, and/or incision and drainage.
In the ED, there are preassembled tonsillar hemorrhage trays. These trays include the instruments commonly used to treat posttonsillectomy bleeds or PTAs and help to streamline procedural efficiency. After use, all instruments in the tray are sent down to the medical device reprocessing (MDR) department for decontamination, sterilization, and re-organization. This process requires person-power, electricity, water, and cleaning supplies, all at a significant cost to the hospital.
Climate change is the most significant threat to global health in the 21st century.4,5 The World Health Organization has labeled it “the single biggest health threat facing humanity.” 6 With ongoing climate change and focus on sustainability, it is important to determine ways to reduce waste in healthcare. London Health Sciences Center (LHSC) is one of Canada’s largest acute-care teaching hospitals. LHSC provides tertiary care for a large portion of Southwestern Ontario. The MDR at LHSC processes over 185,000 trays a year. Therefore, it is essential to ensure that the premade trays contain only necessary instruments.7–10
Previous studies have looked at tray optimization in many areas of surgery, including General Surgery, Plastic Surgery, Orthopedic Surgery, Neurosurgery, Vascular Surgery, and Otolaryngology–Head & Neck Surgery (OHNS).7–13 These studies have shown a significant reduction in hospital costs, improved OR set-up time, shorter MDR processing time, better nurse and surgeon satisfaction, improved surgical efficiency, and better patient safety. The purpose of this project was to determine if these findings translate to an ED procedure tray, specifically the LHSC tonsillar hemorrhage tray. The goal was to reduce unnecessary instruments on the tonsil hemorrhage tray by 30% by 1 year (November 2022–October 2023) and report on the associated cost and carbon footprint savings.
Methods
This project was granted REB ethics exemption as a quality improvement project. It was framed according to the Institute for Healthcare Improvement’s Model for Improvement (Table 1) 14 and started with identification of stakeholders. Structure measures included the number of tonsillar hemorrhage trays. Process measures included the number of times the trays were processed annually and the MDR assembly time. Outcome measures included cost and carbon footprint of the new versus old trays. The reporting of this study is consistent with SQUIRE guidelines. 15
Institute for Healthcare Improvement’s Model for Improvement.

The MDR database was used to determine the number of tonsillar hemorrhage trays used at LHSC each year, MDR assembly time, and cost of the trays. A survey of end-users was used to inform the tray optimization strategy. The survey listed each instrument and asked whether the instrument was used never, rarely, half the time, most of the time, or always. Participants included OHNS and ED residents and staff, who received the survey via e-mail. The survey was open for a period of 2 weeks. Following this, a new tonsillar hemorrhage tray was created. The new assembly time, cost, and carbon footprint was compared to that of the old tray. Tray use differences between staff and residents were compared using a Chi squared test.
Carbon footprint estimation was completed using data from an article published by Rizan et al. 9 Rizan et al determined carbon footprint for individual products and instruments used in 5 common operations in the United Kingdom, including tonsillectomy. They estimated carbon dioxide (CO2) emissions for each instrument using data from raw material extraction, transportation to primary processing site, manufacturing, packaging, waste disposal, and steam sterilization. Using this estimation, the carbon footprint for each instrument on the old and new LHSC tonsil hemorrhage tray was totaled and compared.
Results
Major stakeholders identified included: OHNS staff and residents, ED staff and residents, as well as the MDR team. Review of MDR data showed that there were 14 tonsillar hemorrhage trays in circulation at LHSC. From January 2018 to March 2023, MDR processed the trays 505 times, averaging approximately 100 trays processed per year. The MDR assembly time per tray was 12 minutes.
Fifty-five end-users completed the survey: 11 OHNS faculty, 15 OHNS residents, 25 ED faculty, and 4 ED residents. The response rate was 41%, including 100% of OHNS residents. Residents were significantly more likely to use the tray when compared to staff physicians (P < .001). As such, the resident data were used to examine which instruments should be kept on the tray.
The old tray included 18 instruments, reusable towels, and gauze, totaling a cost of $360 (Table 2). Most of the instruments were not OR-grade, and therefore rust and damage quite easily. Our MDR also estimates that 40% of instruments that are used on the ward trays are never actually returned to MDR and instead are lost or accidentally thrown in the garbage and/or sharps bins. As a result, instruments are replaced approximately 3 times per year, which adds up to over $1000 per tray per year, totaling over $15,000 for 14 trays each year. The MDR assembly time is estimated at 12 minutes. Using the Rizan et al study, it was estimated that 6.11 kg of CO2 emissions is generated in the processing of 100 tonsil hemorrhage trays each year.
Cost of Individual Instruments.

Abbreviation: CAD, Canadian dollars.
Figure 1 illustrates how often the individual instruments on the tray were utilized. Instruments identified by the majority of survey respondents as “never used” were targeted for elimination from the tray. It was noted that there was redundancy in some of the instruments, such as a bowl and medicine cup; the duplicates were subsequently removed. A before and after photograph of the trays is displayed in Figure 2. Ten unnecessary instruments were removed from the original tray (tonsil aspirate needle, metal cotton-tip applicator, curved Metz scissors, Allis tissue forceps, Jennings mouth gag, large bowl, tonsil pillar retractor, needle driver, metal Yankauer suction, Rochester Pean long curved forceps). The new tray contains the following instruments: small and large sweetheart retractors, bayonet forceps, long mosquito forceps, Mayo scissors, Kelly forceps, small cup, and gauze. The remaining instruments can now fit in a small kidney basin instead of a large tray; therefore, the new tray requires less disposable wrap when packaged (Figure 3).

Survey results for how often individual tonsillectomy tray instruments were used by residents.

Tonsillectomy tray before (a) and after (b) optimization.
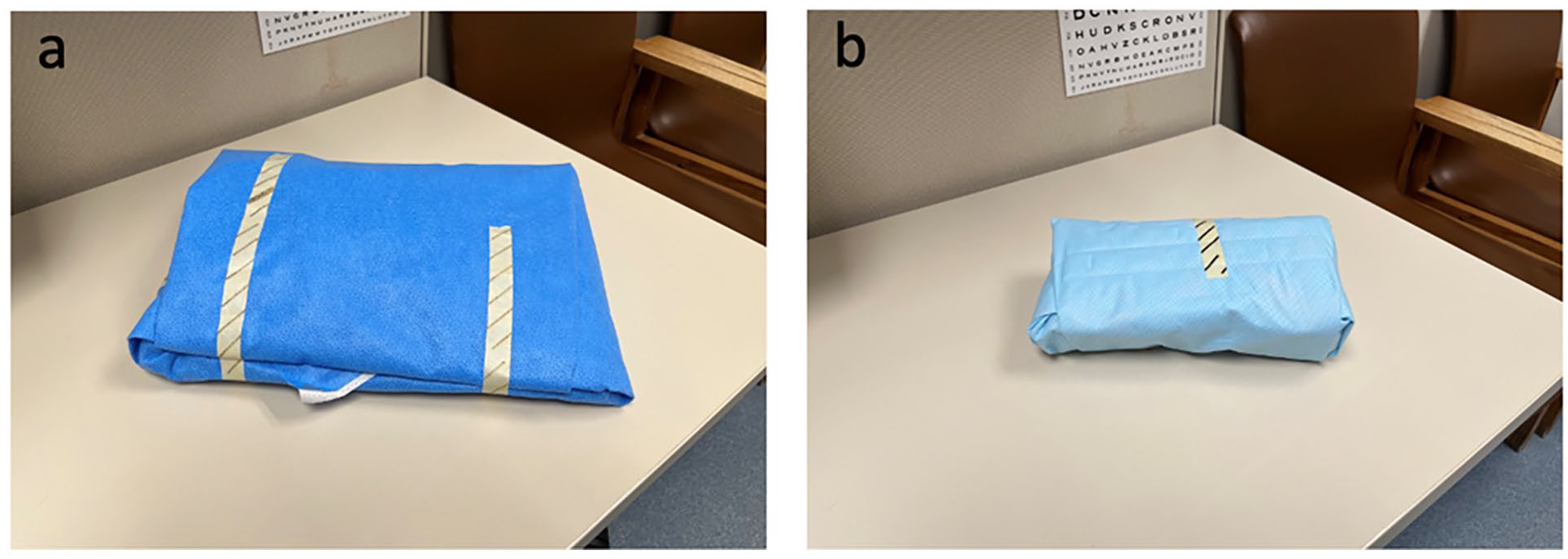
Difference in tray size and packaging before (a) and after (b) optimization.
Table 3 compares the cost, processing time, and carbon footprint differences between the old and optimized tray. The new trays costs 3 times less ($364.21 vs $110.07), requires half the MDR assembly time (12 minutes vs 6-8 minutes), and produces half the carbon emissions (6.11 kg vs 2.85 kg).
Comparison of Old and Optimized Tray.

Abbreviations: CO2, carbon dioxide; MDR, medical device reprocessing.
Discussion
Previous studies have shown that surgical tray optimization can lead to a significant reduction in hospital costs, improved OR set-up time, shorter MDR processing time, better nurse and surgeon satisfaction, improved surgical efficiency, and better patient safety.7–13 The results of our study are consistent with the literature. To the best of our knowledge, this is the first study to focus on ED/ward instrument tray optimization, and report on assembly time, cost, and carbon footprint savings. We surpassed our goal of reducing the number of unnecessary instruments on the tonsillar hemorrhage tray by 30%, reducing the number of instruments by over 50% within the 1-year period. Likewise, the assembly time decreased by one-half, instrument cost savings decreased by one-third, and carbon footprint savings decreased by 50%. Further, the calculated cost savings was purely based on instrument purchase price, so this would likely be an underestimate of true financial savings as we did not factor in the decrease in MDR processing or assembly times. When looking at emissions savings over 10 years, 32.6 kg of carbon emissions can be saved by paring down this single tray at 2 hospitals. This is equivalent to 83.6 miles driven by an average gasoline-powered passenger vehicle. Scaling up this project can have significant impact, as the LHSC MDR processes over 185,000 trays per year.
Several studies have looked at optimizing OR trays in OHNS specifically. Crosby et al 7 investigated instrument use on several surgical trays at a different hospital in London, Ontario. They removed instruments used less than 20% of the time and were able to significantly reduce OR set-up time. Fu et al 11 examined OR tray optimization targeting 5 common OHNS procedures at a hospital in Toronto, Ontario. By reducing trays by 26%, they could save $70,000 over 10 years. The current literature has focused on OR tray optimization, whereas this study is one of the first to look at ED/ward procedure trays.
The “Triple Bottom Line” is a conceptual framework that incorporates the financial, social, and environmental costs of an activity. 16 Numerous physicians, citing a commitment to beneficence and nonmaleficence, have claimed that addressing these costs is part of the moral imperative of healthcare. 17 ORs are responsible for a large percentage of the environmental footprint of a hospital, using 3-6 times more energy than an average unit and producing 20%-30% of a hospital’s total waste. Using a circular economy approach begins with reduction and streamlining instrument trays to avoid excess material use.18–20 In a survey of Canadian Otolaryngologists, Hathi et al showed that although 86% of respondents strongly believed in climate change, only 20% strongly agreed that ORs contributed to the climate crisis, and more than half strongly or somewhat disagreed that the unnecessary contents of surgical trays were routinely assessed at their centers. 21
The limitations of our study include the retrospective reflection required by end-users when completing the survey, which relied on their recall of frequency of instrument use and therefore is unlikely to be completely accurate. Secondly, the Rizan et al study was used for CO2 emissions estimation, and although the sterilization process at LHSC is similar, it is not identical and thus the calculation may not be fully representative. It is worth mentioning that optimizing OR and procedure trays is often not unanimous and requires trade-offs between efficiency, convenience, and safety.
Future directions include repeating the survey after several months of implementing the new tray as a balancing measure to ensure end-user satisfaction and inclusion of necessary instruments, in additional to trialing the new tray in the simulation lab. We can easily adjust the tray as necessary. For example, soon after distribution of the new tray, we realized it was missing the Wieder Tongue Depressor. After a quick email to our MDR team, it was returned to the tray the next week. Further, this quality improvement project will be expanded to optimize other ED and ward procedure trays using similar methodology. Additionally, our MDR reports that nearly 40% of instruments that are used on the ward trays never make it back to MDR, likely due to instruments being lost or thrown away. Another future QI project could focus on increasing surgical instrument return from ward trays to MDR. Lastly, we also plan to share our experience with tray optimization, so other healthcare institutions may use this work to easily improve their procedure trays.
Conclusion
In conclusion, reducing healthcare spending and improving sustainability in healthcare is vital for future generations. Even small physician-led initiatives can make a difference. This project can save LHSC over $100,000 over 10 years, save tray assembly time in MDR, and help reduce LHSCs carbon footprint. The combined effect of numerous small projects can have a large impact on the long-term. Healthcare costs and environmental sustainability are collective responsibilities. Surgical and procedure tray optimization is a simple, effective, and scalable form of eco-action.
Footnotes
Acknowledgements
Thank you to Maria Franco, Suzanne Schwabb, and Catherine Linwood, from the LHSC MDR Department, for there help with the MDR data, as well as organizing the implementation of the optimized tonsil hemorrhage tray.
Author Contributions
K.V.O. was a major contributor in the development of the project and survey, writing the manuscript, and preparing the figures. E.M. was a major contributor in the statistical analysis and writing and editing of the manuscript. S.B. was a contributor in the distribution of the survey and writing and editing of the manuscript. J.S. was a contributor in the development of the project, survey distribution, writing the manuscript, and was the main editor of the manuscript. All authors read and approved the final manuscript.
Availability of Data and Material
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This project was granted REB ethics exemption as a quality improvement project.