
Abstract
Background
Adenotonsillectomy is one of the most common surgical procedures worldwide. The current standard for securing the airway in patients undergoing adenotonsillectomy is endotracheal tube (ETT) intubation. Several studies have investigated the use of the laryngeal mask airway (LMA) in this procedure. We conducted a systematic review and meta-analysis to compare the safety and efficacy of the LMA versus ETT in adenotonsillectomy.
Method
Databases were searched from inception to 2022 for randomized controlled trials and comparative studies. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed. The primary outcome is the rate of perioperative respiratory adverse events (PRAEs). Secondary outcomes included the rate of conversion to ETT, desaturations, nausea/vomiting, and surgical time. A subgroup analysis, risk of bias, publication bias, and Grading of Recommendations Assessment, Development, and Evaluation (GRADE) assessments were also performed.
Results
Twelve studies were included in the analysis (4176 patients). The mean overall conversion to ETT was 8.36% [95% confidence interval (CI) = 8.17, 8.54], and for the pediatric group 8.27% (95% CI = 8.08, 8.47). The mean rate of conversion to ETT secondary to complications was 2.89% (95% CI = 2.76, 3.03) while the rest was from poor surgical access. Overall, there was no significant difference in PRAEs [odds ratio (OR) 1.16, 95% CI = 0.60, 2.22], desaturations (OR 0.79, 95% CI = 0.38, 1.64), or minor complications (OR 0.89, 95% CI = 0.50, 1.55). The use of LMA yielded significantly shorter operative time (mean difference −4.38 minutes, 95% CI = −8.28, −0.49) and emergence time (mean difference −4.15 minutes, 95% CI = −5.63, −2.67).
Conclusion
For adenotonsillectomy surgery, LMA is a safe alternative to ETT and requires less operative time. Careful patient selection and judgment of the surgeon and anesthesiologist are necessary, especially given the 8% conversion to ETT rate.

Keywords
Background
Tonsillectomy with or without adenoidectomy is one of the most common procedures performed worldwide.1,2 In 2010 alone, 399,000 tonsillectomies were performed in the United States, with 72.4% occurring in children under 15 years of age. 3 The most common indications for this surgery in pediatric patients include obstructive sleep-disordered breathing and recurrent throat infections 4 while additional indications include intolerance to multiple antibiotics, a history of 2 or more peritonsillar abscesses, and periodic fever, aphthous stomatitis, pharyngitis, and adenitis. 4 Although generally considered a safe procedure, complications from tonsillectomy can occur, including pain, dehydration, hemorrhage, and dysphagia.5,6
Traditionally, endotracheal tube (ETT) intubation has been the standard of care in securing the airway in pediatric patients undergoing adenotonsillectomy. However, the use of a laryngeal mask airway (LMA) is an alternative option that has been shown to decrease operative time and potentially allow for a larger number of surgical cases to be completed. 7 Unlike an ETT, an LMA forms a seal above the laryngeal inlet and does not pass through the glottis, making insertion easier and reducing the risk of trauma to the oral cavity or larynx.7,8 The LMA has been shown to be a safe alternative to ETT intubation in many surgeries, including abdominal, otologic, and oral surgery.9-11 It can allow for improved hemodynamics during induction and emergence, better airway management, reduced anesthetic requirements, decreased coughing and sore throat as well as improved oxygenation during emergence. 12
However, the use of an LMA is subjected to potential risks, such as laryngospasm and aspiration, which may require conversion to ETT intubation. 13 Surgical exposure with an LMA, which takes up more space than a standard ETT, may lead to increased obstruction when the mouth gag is opened, and may also necessitate conversion to an ETT.
Given the potential benefits of using an LMA in adenotonsillectomy, it is important to further investigate the safety profile of this technique. This systematic review aims to evaluate the current literature on the safety and efficacy of using an LMA compared to traditional ETT intubation in adenotonsillectomy. By doing so, this review can inform clinical decision-making and potentially improve patient outcomes and increase surgical efficiency.
Methods
This systematic review and meta-analysis was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplemental Figure 1).
Study Selection
We included randomized controlled trials (RCTs), controlled nonrandomized clinical trials, prospective and retrospective comparative cohort studies, case-control studies, observational studies, and case series with 5 or more patients. Case series with less than 5 patients and case reports were not included. Only studies with both an experimental group and a control group were included. We also included patients of any age and gender. We only included studies in patients undergoing tonsillectomy with or without adenoidectomy and patients undergoing adenoidectomy only. We excluded any study that had additional procedures performed except for myringotomy and ear tube placement during their adenotonsillectomy.
The intervention was the use of the LMA or an attempt to use an LMA device even if conversion to endotracheal intubation was performed. All types of LMA were included. The comparator was ETT intubation, the current standard of care for adenotonsillectomy.
Outcomes Measures
The primary endpoint was the incidence of perioperative respiratory adverse events (PRAEs). Complications known as PRAEs were grouped together and included apnea, bronchospasm, desaturations, and laryngospasm. This was chosen as a primary endpoint as it is a cumulative measure that measures airway complications perioperatively. Secondary endpoints included the rate of conversion to ETT as well as all other complications reported such as coughing, gagging, kinking issues, stridor, and obstruction from mouth gag insertion, transient hypoxia, nausea, and vomiting. Since many articles reported on transient hypoxia, nausea, and vomiting, we have chosen to group these variables and analyze them as minor complications. Desaturations were also analyzed separately as many PRAE events can ultimately lead to desaturations when severe. This can therefore provide an alternative measure to respiratory/airway events encountered during the surgery. We also reported on measures of operative time, induction time, and emergence time. We did not include studies that did not include outcomes related to complications associated with the anesthetic technique or the surgery.
Electronic Searches
The search was not restricted by date and was searched to November 23, 2022. MEDLINE, EMBASE, Web of Science, Cochrane CENTRAL, clinicaltrials.gov, MedRxiv, and preprints.org were searched using the search strategy developed by a medical librarian in Table 1.
Databases Searched and Search Strategy Used.

Selection of Studies
Literature search results were uploaded to Covidence systematic review software (Veritas Health Innovation, 2022) for evaluation through a 2-step screening process. The first step consisted of assessing abstracts and excluding irrelevant articles as well as obtaining full-text reports for articles that pass this step. The second stage consisted of full-text reviews to evaluate for inclusion criteria.
Both steps were completed by 2 independent reviewers (S.K. and D.Z.P.) and conflicts were resolved by discussion. A rationale for the exclusion of full-text review articles was provided.
Data Extraction and Management
Using a standardized form, both reviewers extracted data independently for each included study using data extraction templates developed a priori. We first extracted patient characteristics, indications for surgery, and country of origin. We then extracted the type of intervention used, medications used for anesthesia, and all outcomes related to our primary and secondary endpoints. When including rates of conversion to ETT, the reason for conversion was also extracted if provided. For the PRAEs, if a patient had more than one PRAE then those were counted separately and the number of PRAEs reported conveys the number of total events between all patients included.
Assessment of Risk of Bias in Included Studies
To assess for any bias, a risk of bias analysis was performed for each of the included studies. For observational studies,14-17 the Newcastle-Ottawa scale (NOS) was used. For RCT,8,11,18-23 the Cochrane 2.0 risk of bias tool 24 was used.
Measures of Treatment Effect
The extracted data were imported into Review Manager 5.4.1 (The Cochrane Collaboration. For each outcome, a forest plot was generated to measure the treatment effect using the odds ratio (OR). We used the inverse variance statistical method with a random effects analysis model. All data were presented with 95% confidence intervals (CIs). Studies were then sorted by effect size on forest plot. Heterogeneity was assessed using Tau squared, chi squared, and I squared. The overall effect was measured using the Z value.
Assessment of Reporting Biases
To assess for any publication bias, a funnel plot was generated with the PRAE data to assess for any asymmetry using Jasp (University of Amsterdam). In addition, an Egger’s test was performed to assess for publication bias using the R terminal (R Foundation). PRAE data were used for the publication bias as this was our primary outcome.
Subgroup Analysis and Investigation of Heterogeneity
A subgroup analysis was performed to better understand the heterogeneity between studies when present. The analysis compared articles including only pediatric patients to articles including adult and pediatric patients.
Sensitivity Analysis
Finally, to better understand the strength of the results presented, all outcomes were judged using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology. This analysis was performed using GRADEpro (Evidence Prime). The quality of the outcomes was then reported as high, moderate, low, or very low. Of note, since our review included both RCT and observational studies, the quality of evidence used for GRADE analysis was set to that of the study with the lowest quality of evidence which in our case was observational.
Results
Description of Studies
The literature search yielded 240 articles, and after screening and full-text review, 12 were included in this systematic review (Figure 1). From the articles included, there were a total of 4176 participants. Eight studies were RCTs,8,11,18-23 3 were cohort studies,15-17 and 1 was a retrospective case series. 14 A full description of the study design and outcomes reported for each study is summarized in Table 2.

PRISMA flow diagram for study selection using Covidence. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study Characteristics and Participants’ Demographics.
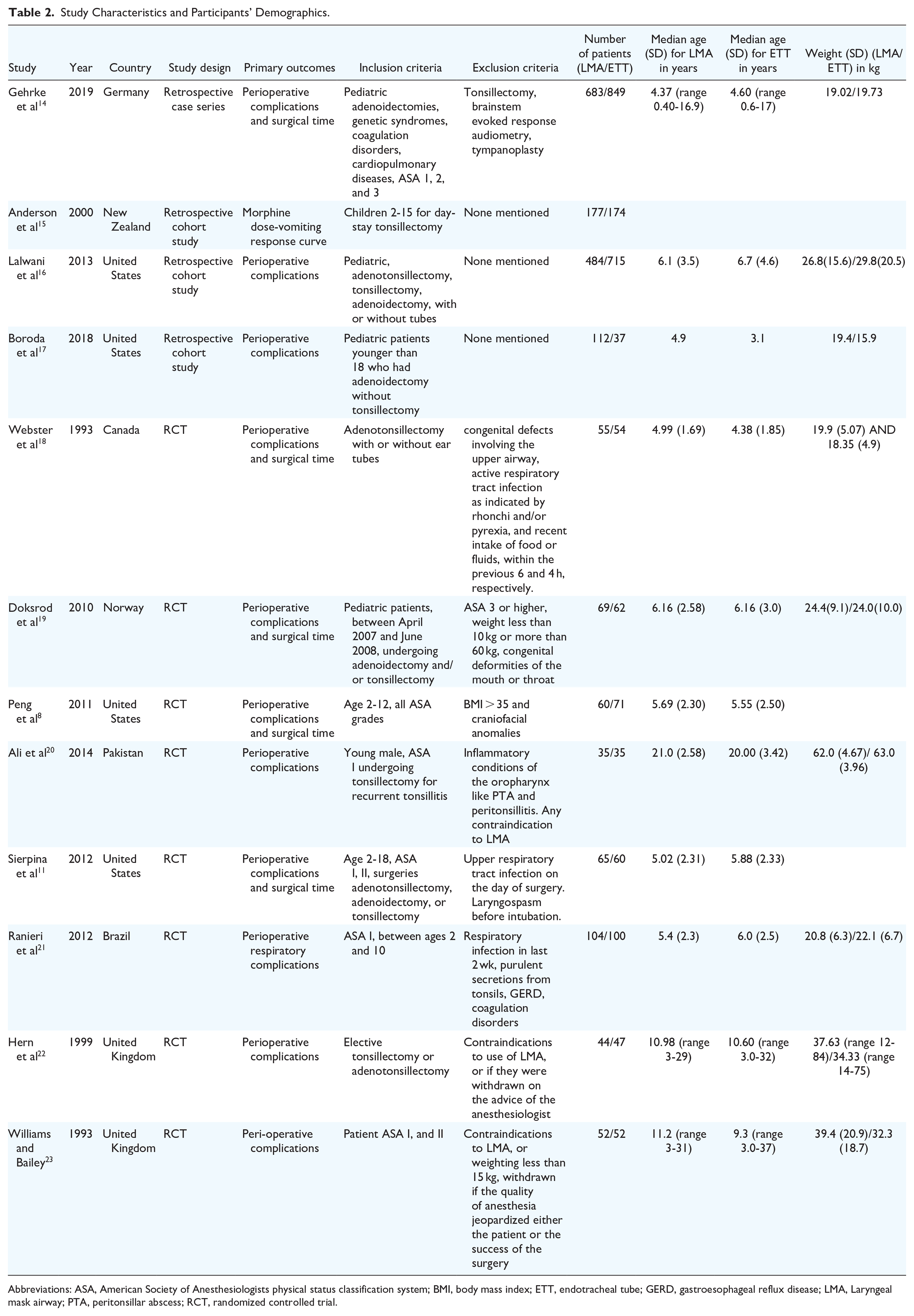
Abbreviations: ASA, American Society of Anesthesiologists physical status classification system; BMI, body mass index; ETT, endotracheal tube; GERD, gastroesophageal reflux disease; LMA, Laryngeal mask airway; PTA, peritonsillar abscess; RCT, randomized controlled trial.
Risk of Bias in Included Studies
A risk of bias analysis was performed in all studies included. RCTs were analyzed using Cochrane 2.0 risk of bias tool assessment (Supplemental Figure 2a). Of those studies, 3 had a low overall risk of bias, 4 had some concerns for bias, and 1 had a high risk of bias. The study by Williams published in 1993 was found to have a high risk of bias secondary to missing outcome data as participants who were converted from LMA to ETT were not analyzed in their LMA group. For the observational studies, the NOS was used to assess for bias. A low risk of overall bias was found for all 3 studies included (Supplemental Figure 2b).
Perioperative Respiratory Adverse Events
In our analysis, PRAEs included the sum of bronchospasms, laryngospasms, desaturations, and persistent hypoxia. Our analysis shows no significant difference in PRAEs (OR 1.16, 95% CI = 0.60, 2.22; sample size 3710) between the LMA and ETT groups. There was also no significant difference when looking at the pediatric group alone with an OR 1.02 (95% CI = 0.50, 2.12; sample size 3445). The heterogeneity was 0.64 and the overall effect was 0.43 (Figure 2a) This analysis was also repeated after removing the one study with a high risk of bias and still did not show any significant difference between the LMA and ETT in terms of PRAEs (Figure 2b).

(a) Forest plot comparing the total number of PRAEs between the LMA and ETT as an odds ratio. The peds group includes only pediatric patients and the mixed group includes both pediatric as well as adult patients. (b) Forest plot comparing the total number of PRAEs between the LMA and ETT as an odds ratio excluding the data from the study by Williams 1993. The peds group includes only pediatric patients and the mixed group includes both pediatric as well as adult patients. (c) Conversion rate from LMA to ETT shown as a percentage of all intubations in the total group as well as the pediatric group. The error bars represent the standard deviation. (d) Forest plot comparing the total number of minor complications between the LMA and ETT as an odds ratio. (e) Forest plot comparing the total number of desaturations between the LMA and ETT as an odds ratio. The peds group includes only pediatric patients and the mixed group includes both pediatric as well as adult patients. (f) Forest plot comparing the intubation time between LMA and ETT. (g) Forest plot comparing the extubation time between LMA and ETT. (h) Forest plot comparing the total operative time between LMA and ETT. PRAE, perioperative respiratory adverse events; LMA, laryngeal mask airway; ETT, endotracheal tube.
Conversion Rate
The overall mean conversion rate from LMA to ETT was 8.36% (95% CI = 8.17, 8.54; sample size: 1759) and the conversion rate for the pediatric-only group was 8.27% (95% CI = 8.08, 8.47; sample size: 1632). Conversions that were performed secondary to complications were 2.89% (95% CI = 2.76, 3.03) while the rest were performed secondary to issues with surgical access. In the pediatric group, the conversion secondary to complications was 2.43% (95% CI = 2.22, 2.64) and the rest were performed secondary to surgical access issues (Figure 2c).
Minor Complications
Minor complications were defined as episodes of nausea, vomiting, transient pain, and transient hypoxia as reported by the different studies. Overall, there was no significant difference between LMA and ETT with OR 0.89 (95% CI = 0.50, 1.55; sample size: 2449). Heterogeneity was 0.37 and the overall effect was 0.42. For the pediatric group, there was also no significant difference with OR 0.97 (95% CI = 0.54, 1.74; sample size: 2379 participants; Figure 2d).
Desaturations
In terms of desaturations experienced perioperatively or while admitted in the hospital postoperatively, there was no significant difference between the LMA and ETT with OR 0.79 (95% CI = 0.38, 1.64; sample size: 3506). Heterogeneity was 0.31 and overall effect was 0.63. There was also no significant difference in the pediatric group with an OR of 1.17 (95% CI = 0.18, 7.57; sample size: 3241; Figure 2e).
Efficiency Measures
There was no significant difference between intubation time comparing the LMA and ETT with a mean difference of 0.37 minutes favoring the LMA (95% CI = −0.01, 0.75; sample size: 371). Heterogeneity was 0.05 and the overall effect was 1.89 (Figure 2f). For extubation time, the LMA was significantly faster than the ETT with a mean difference of 4.15 minutes (95% CI = 2.67, 5.63; sample size: 262). The heterogeneity was 0.01 and the overall effect was 5.49 (Figure 2g). For total operating room time, the LMA was significantly faster than the ETT with a mean difference of 4.38 minutes (95% CI = 0.49, 8.28; sample size: 262). The heterogeneity was 0.00 and the overall effect was 2.21 (Figure 2h).
Publications Bias and GRADE Analysis
To assess for publication bias, a funnel plot was generated and did not show any evidence of significant asymmetry (Supplemental Figure 3). In addition, Egger’s test was performed and generated a Z value of 0.708 and a P value of .479.
On GRADE analysis, each variable was assessed for overall certainty. Conversion to ETT and total operating room time both had high certainty on assessment and the total PRAEs had moderate certainty. Minor complications, desaturations, nausea/vomiting, and extubation time all had low certainty on the GRADE assessment (Supplemental Figure 4).
Discussion
Our systematic review and meta-analysis of 12 studies including 4176 patients suggest that the LMA is a safe alternative to ETT in adenotonsillectomy. There was no statistically significant difference in the number of PRAEs, desaturations, and minor complications between the LMA and ETT in patients undergoing tonsillectomy. Similarly, no difference was seen in the pediatric subgroup.
The use of ETT in adenotonsillectomy is the current standard practice. Our study found, when LMA is used, the conversion rate from LMA to ETT was 8.36% (8.27% of cases for the pediatric subgroup). However, the majority of the conversions were secondary to surgical access and positioning issues and not secondary to complications. The conversion secondary to complications was 2.89% (2.43% for the pediatric population). This suggests that most conversions, when necessary, are performed in a safe and controlled setting. The number of conversions secondary to access may decrease as surgeons and anesthesiologists become more comfortable with using the LMA with this type of procedure. In addition, careful patient selection may also help reduce the rate of conversions. Based on our clinical experience, we believe excluding patients with a known difficult airway, age less than 2, a high body mass index (BMI), and craniofacial abnormalities may help in both reducing complications as well as issues with surgical access.
The LMA has been shown to be an efficient alternative to ETT in different surgeries. A 1995 meta-analysis shows that the LMA helps improve induction and emergence hemodynamics as well as decrease coughing and sore throat postoperatively. 12 More recent meta-analyses show significantly fewer pharyngolaryngeal complications after thyroidectomy 25 as well as significantly lower instances of laryngospasm, cough, dysphagia, and dysphonia in laparoscopic surgery for the LMA when compared to the ETT. 26 The LMA also helps reduce the narcotic requirement during surgery which is especially beneficial in the pediatric population. 27 In addition, our analysis shows that the LMA may improve operative time likely by improving the ease and efficiency of extubation and emergence. With evidence of decreased cardiopulmonary stimulation and ease of emergence, the LMA could potentially be beneficial for patients with reactive airway disease or comorbidities that predispose patients to PRAEs. 8
However, there are some limitations to the LMA especially as it relates to adenotonsillectomy. First, the LMA does not protect against aspiration. If excessive bleeding is encountered during the surgery, the risk of aspiration would be greater with an LMA. However, our review did not find aspiration to be a concern in patients treated with LMA. The second concern is issues regarding tube obstruction leading to difficulties with ventilation. It is hypothesized that this could be secondary to a lower depth of anesthesia resulting in reflex laryngeal closure with mouth gag opening, 18 mechanical compression of the device, or displacement of the epiglottis. 8 One potential solution could be to use a half-size smaller LMA to improve surgical access and decrease rates of obstructions as suggested in the study by Peng et al. 8 It is also beneficial to use a mouth gag that includes a groove for the LMA, such as the Boyle-Davis, which often provides more space for the tube before causing an obstruction. In addition, the use of a reinforced flexible LMA may be especially useful in this procedure as it may help decrease rates of mechanical tube obstruction with mouth gag opening. 20 In our clinical experience, we have found that a regular reinforced LMA fared better than a flexible LMA. We believe more studies comparing the different types of LMA available would help optimize success in this procedure.
Overall, the data used in this meta-analysis were extracted from articles with a low or medium risk of bias. Only one article included in the analysis had a high risk of bias. To resolve possible confounders secondary to these data, the analysis as it relates to safety measures was repeated omitting the data from the one article with a high risk of bias. This new analysis still did not show any significant differences between LMA and ETT in terms of PRAEs, desaturations, or minor complications.
There are multiple limitations to this review. First, our analysis of PRAEs did yield moderate to substantial heterogeneity with a tau score of 0.64. This can be secondary to the different types of LMAs used in the different studies in addition to the different types of procedures performed. In addition, most studies only counted a PRAE once while one study allowed a patient to have multiple PRAEs. 18 Not all studies included PRAEs measured postoperatively which likely also contributed to the heterogeneity seen in this outcome. There was not enough data provided from the studies to perform a subgroup analysis based on the procedure performed, that is, adenotonsillectomy, tonsillectomy, or adenoidectomy alone. In addition, we were unable to control for additional procedures such as myringotomy and ear tube placement. Second, another limitation stems from the different exclusion criteria in the different studies. Many studies excluded patients with congenital deformities of the head and neck as well as patients with a high BMI. This does affect the generalizability of the study as it relates to the use of LMA in adenotonsillectomy. In that sense, the surgical team and anesthesiology team need to be mindful of who would be a good candidate for the use of LMA. Third, the measure of efficiency as they relate to total operating room time, intubation time, and extubation time had small sample sizes, especially when compared to the total participants in this study. This is secondary to many articles reporting outcomes relating to adverse events but very few reporting outcomes of efficiency. In addition, while total operative time and extubation time were measured similarly in the articles compared, intubation time was not. One article measured it from the time of induction to intubation, 18 another from the time of entering the operating room to intubation, 19 and the last one from the time of removing the face mask to intubation. 8 This likely contributed to the heterogeneity seen in those values as well.
Finally, another limitation is the limited difference in total operating room time between both groups. While using the LMA significantly reduces total operating room time, it only does so by about 4 to 5 minutes on average. It is important to note that since this analysis was performed as intention-to-treat analysis, this also includes patients who were intended for LMA and converted to ETT and therefore had a longer total operating room time.
Our findings highlight the LMA as a safe and efficient alternative to ETT in select adenotonsillectomy patients which provides additional airway management options for surgeons and anesthesiologists. Future prospective studies would help compare LMA and ETT by controlling for potential confounding patient factors. At our center, LMA use is being investigated with surgeries done in more efficient minor procedure rooms, which have been previously shown to be cost effective. 28
Conclusion
The use of the LMA in adenotonsillectomy is a safe and efficient alternative to ETT intubation in most adult and pediatric patients. Careful patient selection and judgment of the surgeon and anesthesiologist are paramount. Conversion to ETT may be necessary in approximately 8% of patients. Future research should focus on determining which patients may be suitable candidates for consideration of LMA for airway management during adenotonsillectomy, and ways to anticipate and/or decrease the potential need for conversion to ETT.
Supplemental Material
sj-docx-1-ohn-10.1177_19160216241263851 – Supplemental material for The Safety of the Laryngeal Mask Airway in Adenotonsillectomy: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-ohn-10.1177_19160216241263851 for The Safety of the Laryngeal Mask Airway in Adenotonsillectomy: A Systematic Review and Meta-Analysis by Sami Khoury, Dorsa Zabihi-Pour, Jacob Davidson, Raju Poolacherla, Gopakumar Nair, Abhijit Biswas, Peng You and Julie E. Strychowsky in Journal of Otolaryngology - Head & Neck Surgery
Supplemental Material
sj-docx-2-ohn-10.1177_19160216241263851 – Supplemental material for The Safety of the Laryngeal Mask Airway in Adenotonsillectomy: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-ohn-10.1177_19160216241263851 for The Safety of the Laryngeal Mask Airway in Adenotonsillectomy: A Systematic Review and Meta-Analysis by Sami Khoury, Dorsa Zabihi-Pour, Jacob Davidson, Raju Poolacherla, Gopakumar Nair, Abhijit Biswas, Peng You and Julie E. Strychowsky in Journal of Otolaryngology - Head & Neck Surgery
Supplemental Material
sj-docx-3-ohn-10.1177_19160216241263851 – Supplemental material for The Safety of the Laryngeal Mask Airway in Adenotonsillectomy: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-3-ohn-10.1177_19160216241263851 for The Safety of the Laryngeal Mask Airway in Adenotonsillectomy: A Systematic Review and Meta-Analysis by Sami Khoury, Dorsa Zabihi-Pour, Jacob Davidson, Raju Poolacherla, Gopakumar Nair, Abhijit Biswas, Peng You and Julie E. Strychowsky in Journal of Otolaryngology - Head & Neck Surgery
Supplemental Material
sj-docx-4-ohn-10.1177_19160216241263851 – Supplemental material for The Safety of the Laryngeal Mask Airway in Adenotonsillectomy: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-4-ohn-10.1177_19160216241263851 for The Safety of the Laryngeal Mask Airway in Adenotonsillectomy: A Systematic Review and Meta-Analysis by Sami Khoury, Dorsa Zabihi-Pour, Jacob Davidson, Raju Poolacherla, Gopakumar Nair, Abhijit Biswas, Peng You and Julie E. Strychowsky in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Acknowledgements
We gratefully thank Brad Dishan (London Health Sciences Center Clinical Librarian) for his help in developing the search strategy.
Author Contributions
S.K. contributed to the conception and design of the paper, extracted and analyzed the data, and drafted the manuscript. D.Z.P. extracted and analyzed the data. J.D. contributed to the conception and design and revised the manuscript. R.P., G.N., and A.B. contributed to the design of the paper and revised the manuscript. P.Y. and J.E.S. contributed significantly to the conception and design of the paper, reviewed the analysis and made significant revisions to the manuscript.
Availability of Data and Materials
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Not applicable.
Registration
Registered through PROSPERO with ID—CRD42022378232.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.