
Abstract
Background
The diagnosis and treatment of head and neck cancer (HNC) is associated with several life-altering morbidities including change in appearance, speech, and swallowing, all of which can significantly affect quality of life and cause psychosocial stress.
Commentary
The aim of this narrative review is to provide an overview of the evidence on psychosocial interventions for patients with HNC. Evidence regarding screening tools, psychological interventions, smoking and alcohol cessation, and antidepressant therapy in the HNC population is reviewed.
Conclusion
There is a large body of evidence describing various psychosocial interventions and several of these interventions have shown promise in the literature to improve psychosocial and health outcomes in the HNC population. Psychosocial interventions should be integrated into HNC care pathways and formal recommendations should be developed.

Background
The treatment of head and neck cancer (HNC) often involves intense multimodal therapy including surgery, radiation, and chemotherapy. These therapeutic strategies can lead to challenges with form and function including speech and swallowing. 1 Quality of life is often severely affected, and a patient’s body image, communication, and social interactions may be compromised. As such, rates of psychological distress are high among HNC patients.2,3 Compared to other cancer populations, HNC patients are more likely to experience depression, anxiety, and psychosocial distress.4-8 In one study of over 50,000 patients with a new diagnosis of HNC, the proportion of patients with mental health disorders increased from 20% to 30% after diagnosis. 9 The physical visibility of HNC itself and the associated social implications are intricately tied to the anxiety that several patients experience. Sources of anxiety and depression in HNC have been associated with the fear of cancer recurrence, loss of occupation, and loss of social status.10,11 Furthermore, the rates of suicide in patients with HNC are 3 times higher than those of the general population and they carry the highest rates of self-harm relative to other cancer sites.4,12,13 Within head and neck oncology, mental health is an extremely important factor to consider given that psychiatric conditions have been shown to modulate treatment response, adherence to therapy, and serve as an important risk factor in overall survival.5,9 While different interventions exist, there are no formal recommendations or consensus guidelines for HNC patients experiencing psychosocial distress. The current literature describes the efficacies of different interventions in a multidisciplinary HNC team, but there is no cohesive summary of these interventions framed in a clinically relevant format. The goal of this narrative review was to provide a succinct, clinically applicable overview of the current state of evidence on psychosocial interventions for HNC patients and highlight gaps in the literature and potential avenues for future research. A brief summary of the various interventions discussed can be found in Table 1.
Summary of Interventions to Reduce Psychosocial Burden in HNC Patients.
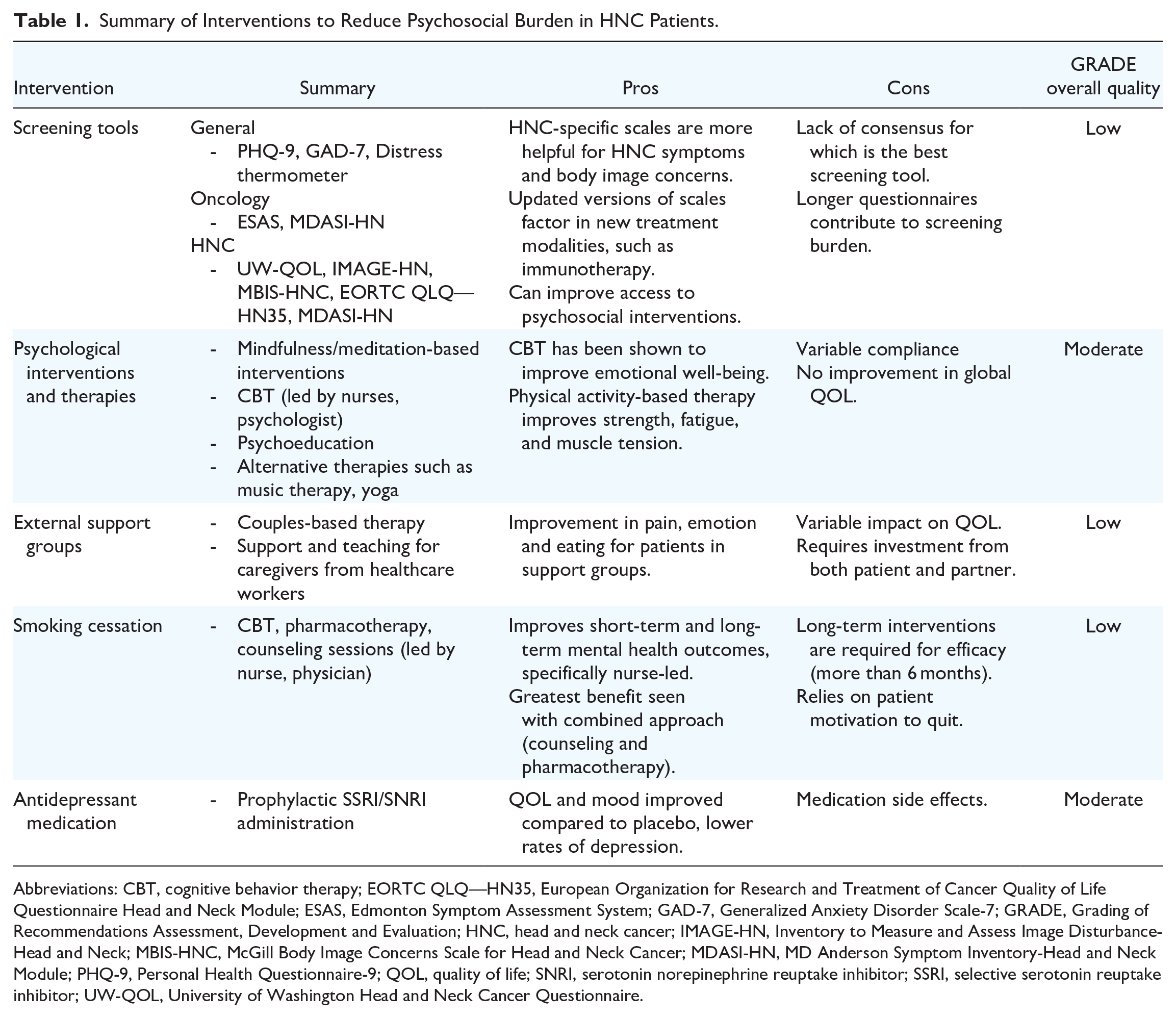
Abbreviations: CBT, cognitive behavior therapy; EORTC QLQ—HN35, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Head and Neck Module; ESAS, Edmonton Symptom Assessment System; GAD-7, Generalized Anxiety Disorder Scale-7; GRADE, Grading of Recommendations Assessment, Development and Evaluation; HNC, head and neck cancer; IMAGE-HN, Inventory to Measure and Assess Image Disturbance-Head and Neck; MBIS-HNC, McGill Body Image Concerns Scale for Head and Neck Cancer; MDASI-HN, MD Anderson Symptom Inventory-Head and Neck Module; PHQ-9, Personal Health Questionnaire-9; QOL, quality of life; SNRI, serotonin norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor; UW-QOL, University of Washington Head and Neck Cancer Questionnaire.
Screening Tools
Early use of validated tools can be implemented by clinicians to identify patients who are socially and psychologically in distress because of their HNC diagnosis. 14 The Personal Health Questionnaire-9 (PHQ-9) 15 and Generalized Anxiety Disorder Scale-7 (GAD-7) 16 are examples of commonly used general depression and anxiety scales based on the DSM-5. When used in the HNC population, studies found that approximately 5% to 21% of HNC patients reported clinically significant psychological distress. 17 When employing more oncology-specific scales that are commonly used in HNC, such as the Distress Thermometer, the Edmonton Symptom Assessment System (ESAS), MD Anderson Symptom Inventory (MDASI), and the University of Washington Head and Neck Cancer Questionnaire (UW-QOL V4), studies revealed even higher distress rates up to 60%.14,17-20
There have been several screening tools focused on symptoms specific to HNC patients including the Inventory to Measure and Assess Image Disturbance—Head and Neck (IMAGE-HN) and McGill Body Image Concerns Scale for Head and Neck Cancer (MBIS-HNC), which can be especially useful as approximately 75% of HNC patients express body image concerns.21-23 The IMAGE-HN has been demonstrated to be reliable and valid with scores correlating directly to clinically significant cancer-related body-image distress. 24 Similarly to the IMAGE-HN, the Shame and Stigma Scale for HNC patients has been validated in Canadian French and English-speaking populations and is based on 4 core domains including: shame with appearance, sense of stigma, regret, and social/speech concerns. 25 The MD Anderson Symptom Inventory-Head and Neck module is another tool which contains 11 HNC-specific items and has been demonstrated to be reliable and valid.26,27 Last, the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Head and Neck Module (EORTC QLQ—HN35) was initially validated in 1999 as a 35-item questionnaire based on 7 scales: pain, swallowing, senses, speech, social eating, social contact, sexuality. 28 It has since been replicated successfully worldwide and is applicable before, during, and after HNC treatment whether that includes radiation, surgery, or chemotherapy.29,30 More recently, modifications to this scale were introduced due to advances in HNC treatment, such as immune checkpoint inhibitors or tailored dose-dependent radiation that did not previously exist when the EORTC QLQ was first created.
Unfortunately, there is no consensus on which of these screening tools is the most appropriate for the HNC population and few studies compare the various tools. 17 In Ontario and many other jurisdictions, the ESAS is widely implemented in cancer centers. 5 It measures 9 cancer-related symptoms, 2 of which are depression and anxiety, and is well studied in the overall cancer and HNC literature.5,31 Gascon et al 17 demonstrated that longer screening tools such as the PHQ-9 and GAD-7 had lower volumes of positive screens but higher sensitivity, whereas shorter tools such as the ESAS or MD Anderson Symptom Inventory-Head and Neck Module (MDASI-HN) captured a range of symptoms that all contributed to distress while decreasing screening burden.
Psychological Interventions and Therapies
Individual psychotherapy comes in many forms, ranging from individual-led mindfulness to psychiatrist-led therapy. 32 A few studies have demonstrated that mindfulness and/or meditation-based interventions can lead to some improvements in emotional well-being in patients with HNC.33,34 These studies, however, were limited by variable rates of compliance which have been similarly echoed in other reviews on adherence to psychological interventions in the general oncology population.35,36 Other individual studies investigating nurse-led counseling programs, 37 home-delivered psychosocial interventions, and psychologist-led therapeutic interventions38-41 have reported improved psychosocial functioning, depression, and anxiety. However, when looking at consensus studies, such as the 2013 Cochrane review on psychological interventions for HNC patients which included 7 studies, it concluded that there was no evidence to suggest that psychosocial intervention promotes global quality of life. 42 Psychoeducation in the context of HNC consists of meetings with nurse specialists or other providers, such as care coordinators, who inform patients and their families about the symptoms and side effects of HNC, as well as the impact those side effects may have on their social life and work.38,43-48 Three randomized control trials (RCTs) have been conducted examining the impact of psychoeducation in HNC and found that patients who received psychoeducation had a better oropharyngeal function, less fear and anxiety related to social interaction, and a better perception of facial disfigurement.43,44,49 In addition, cognitive behavior therapy (CBT) is another form of psychotherapy which focuses on challenging thoughts and beliefs and their associated behaviors to promote emotional regulation and improve coping strategies. 50 CBT has been proven to be one of the most effective treatments for improving cancer-related fatigue, improving quality of life, and reducing fear of cancer recurrence.51-53 A meta-analysis from Calver et al 54 showed an improvement in emotional well-being for patients who underwent CBT, but no change in functional or physical well-being. Overall, the evidence regarding CBT in HNC patients remains inconclusive. This may be due to the unique voicelessness and inability to communicate verbally among HNC patients which is not only a driver for emotional distress, but also as a barrier in engaging in verbal psychotherapy.55,56 One RCT found that 6 nurse-led CBT sessions led to improved emotional functioning, pain, swallowing, and mouth opening at 12 months. 57 However, other RCTs investigated 6 or more sessions of CBT and reported no difference in depressive symptoms and failed to demonstrate sustained improvements in psychological outcomes at timepoints greater than 12 months after therapy.57-60
Alternative types of therapy, such as physical activity, acupuncture, or music, have also been described to improve outcomes in survivors of HNC. In a recent systematic review evaluating the impact of physical activity on HNC survivors, more than half of the studies included demonstrated that physical activity resulted in improvement of at least one patient reported outcome with the most common being fatigue.61,62 Given that muscle wasting and cachexia are prevalent in this patient population, it is important to note that many of these studies have demonstrated improvements in lean body mass, muscular strength, and physical functioning both during and after treatment. These preliminary findings suggest that exercise and physical activity may represent an important component of HNC management; however, further research is needed to determine the best type of exercise and timing of physical activity interventions. 61 Specifically, yoga has been proposed as a therapy to improve muscular tension in head and neck survivors, where neck fibrosis, lymphedema, and trismus is a significant side effect of radiation therapy.63,64 Music therapy has also been discussed as an intervention to decrease anxiety in oncology patients undergoing radiation therapy, which may be particularly applicable in the HNC population as it appeals to an unaltered sense.65,66
External Support Groups and Systems
Spouses and partners often bear the responsibility of being caregivers for their loved ones with HNC providing emotional support, assistance with symptom management, and rehabilitation. The distress rates among spouses and partners with HNC has been found to be comparable to the distress rates among the patients themselves and one study reported 83% of couples reported increased conflict during treatment.67,68 In addition to the stress associated with being a caregiver, human papillomavirus (HPV)-related tumors can have unique impacts on partners due to the sexually transmitted nature of HPV. One study reported partners experience guilt and responsibility associated with HPV-related cancers and significant declines in the frequency of sexual intercourse. 69 There is preliminary evidence suggesting that couples-based therapy may have a positive impact on individual and relationship functioning in HNC patients.1,67,70 Couples-based interventions reported in the literature include combinations of educational material focused on self-care, symptom management, and caregiving skills in addition to group sessions with trained mental health professionals. 67
HNC patients share an understanding of the unique psychosocial impacts of their disease. Thus, group sessions have been proposed for these patients which both encompasses their loved ones and/or other HNC cancer patients. One study by Vakharia et al 71 investigated the impact of participation in a support group on quality of life for HNC survivors and found that they had significantly better scores in the domains of eating, emotion, and pain. Conversely, Mowry and Wang 72 found that patients who participated in support groups did not demonstrate improved quality of life but concluded that this may be due to the fact that more patients who participated in the support group had oropharyngeal cancer and were undergoing chemotherapy at time of participation.
Smoking Cessation
Smoking and alcohol intake are shared risk factors both for developing HNC and poor mental health outcomes.73-75 Continued smoking after diagnosis is common and is associated with concurrent depressive symptomatology, more pain, lower quality of life scores, and worse performance status postoperatively.76-79 In the general population, it has been shown that smoking cessation leads to improved mental health outcomes in short-term and long-term studies.80,81 Within the HNC population, 2 pilot studies compared various smoking cessation interventions and found that nurse delivered CBT and pharmacotherapy resulted in significant increases in smoking cessation rates, up to 16% increase when compared to no intervention at a 6-month follow-up.59,82 Interestingly, in similar studies with a shorter follow-up time such as 1 or 3 months, there were no significant difference in rates of smoking cessation between interventions such as CBT, pharmacotherapy, or individual counseling, suggesting that perhaps longer courses of intervention are needed.83,84 Other studies have looked at physician-delivered advice to stop smoking with a contracted quit date, tailored written materials, and booster advice sessions, which have not shown changes in cessation rates but had patient-reported positive mental health effects. 85
A patient’s motivation to quit is also important in predicting the response to smoking cessation therapies, and HNC patients are oftentimes less likely to enroll in cessation interventions due to low perceived risk of recurrence and low quitting self-efficacy.86,87 In a large (N = 186), randomized controlled trial of a provider-based smoking cessation intervention, Gritz et al 85 concluded that the intervention effect was not significant, but that smokers in the contemplation phase were more likely to maintain abstinence in a 1 year follow-up. These findings emphasize the need to integrate early, targeted cessation interventions into the standard HNC care path. Despite the existence of smoking cessation counseling programs, there is insufficient knowledge of these resources among head and neck surgeons especially as it is not currently considered a priority in the treatment process.88,89 The role of motivational support, relationship with alcohol, and health knowledge and beliefs surrounding smoking and cancer have all been discussed as key elements in the holistic approach to a HNC patient and are an important considerations in smoking cessation. 77
Antidepressant Medication
Major depressive disorder has been reported in up to 52% of patients diagnosed with HNC cancer, which is significantly higher when compared to other forms of cancer.5,90,91 In fact, a recent study showed a 64% prevalence rate of depressive symptoms on ESAS screening in HNC patients in Ontario. 92 Moreover, the HNC population is at higher risk of self-injury and suicide.4,13,93 Higher rates of depression among cancer patients can lead to decreased adherence to treatment and overall lower survival, which makes it even more important to address early on.94,95 Within HNC, studies have shown consistent depression levels as far as 5 years post-surgery, but close to zero use of mental health resources and nonadherence to antidepressant medication. 96 The role of antidepressant therapy as a prophylactic measure has only recently been described among the HNC population. Lydiatt et al conducted a pilot study in 2008 and a larger-scale RCT in 2013 testing whether prophylactic selective serotonin reuptake inhibitors (SSRIs) could reduce the incidence of depression among patients with HNC. The pilot study only included 36 patients but showed that citalopram improved quality of life and improved mood when compared to placebo. 97 Later, this study was expanded in 2013 to include 148 HNC patients and compared escitalopram to placebo. 98 They found a 14% reduction in rates of developing depression when patients were prophylactically treated with a 16 week course of escitalopram and a 7-fold risk reduction [hazard ratio 0.37, 95% confidence interval (0.14-0.96), P = .04]. The number needed to treat was 7 for treatment versus placebo. Despite these favorable outcomes, there have been no other studies looking at the role of pharmacotherapy in the primary prevention of depression in HNC patients. 99 Moreover, antidepressants are associated with side effects including sexual dysfunction, nausea, decreased appetite, and sleep disturbance all of which could be detrimental to HNC patients who are concurrently dealing with treatment side effects.
Conclusions
The diagnosis and management of HNC can potentially lead to a substantial impact on patients’ psychosocial functioning. These patients are at high risk of mental health distress and reducing this burden can improve both morbidity and mortality. Early detection using various screening tools to identify high-risk patients, smoking cessation programs, prophylactic pharmacotherapy, and psychological counseling are different modalities that have demonstrated variable benefit. Formal recommendations should be developed and a greater focus on psychosocial interventions should be emphasized in all HNC treatment pathways.
Footnotes
Acknowledgements
None.
Author Contributions
TC and EG preformed the literature review. AE and TC proposed the idea for this report. All authors wrote, reviewed, and edited the manuscript. All authors read and approved the final manuscript before submission.
Availability of Data and Materials
Not applicable.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Ethics Approval and Consent to Participate
Not applicable.