
Abstract
Objectives
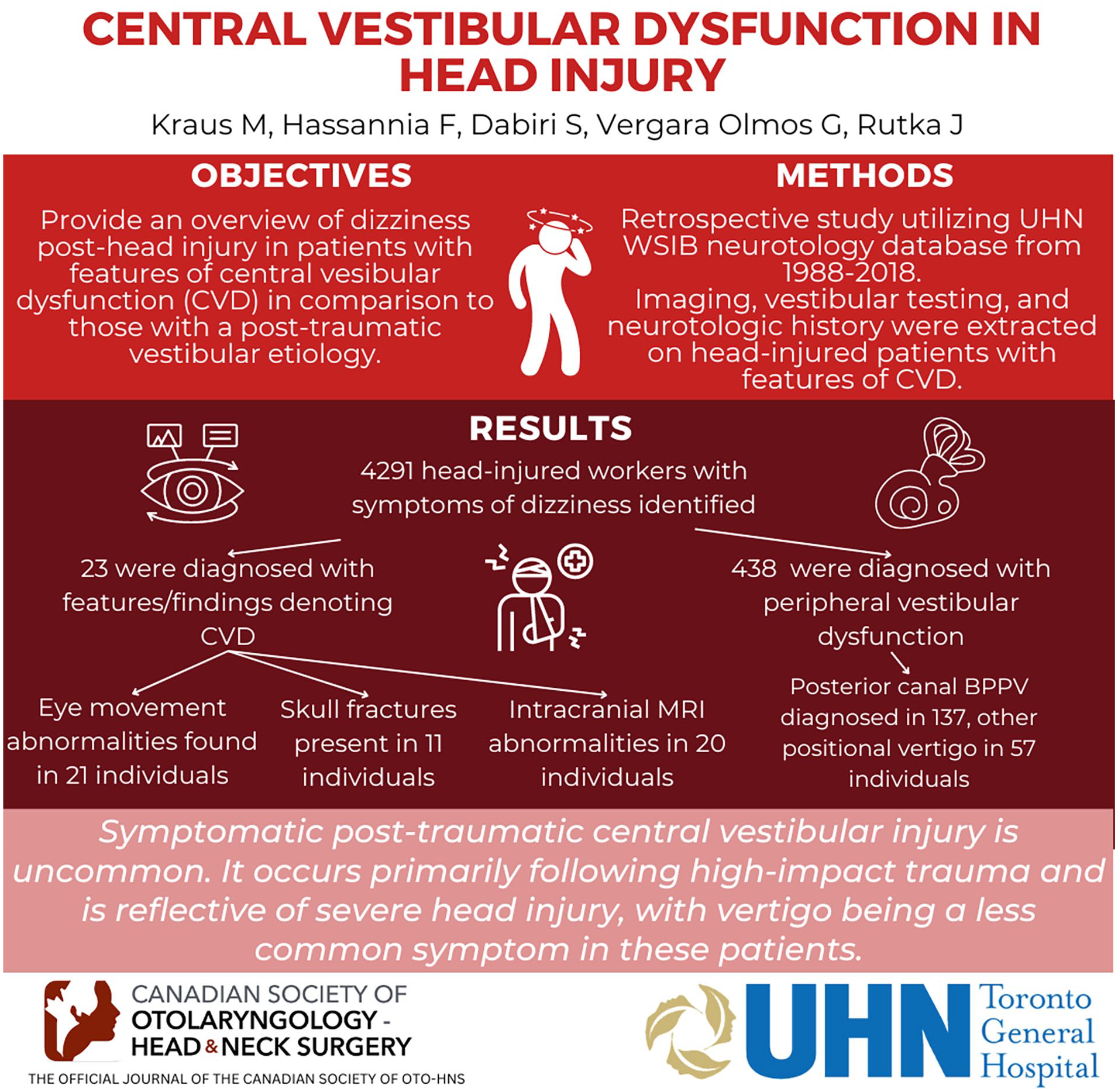
This study aims to provide an overview of dizziness post head injury in those with prominent features for central vestibular dysfunction (CVD) in comparison to those with a post-traumatic peripheral vestibular etiology.
Study design
Retrospective.
Setting
University Health Network (UHN) Workplace Safety and Insurance Board (WSIB) database from 1988 to 2018 were evaluated for post-traumatic dizziness.
Methods
The UHN WSIB neurotology database (n = 4291) between 1998 and 2018 was retrospectively studied for head-injured workers presenting with features for CVD associated with trauma. All patients had a detailed neurotological history and examination, audiovestibular testing that included video nystagmography (VNG) and cervical vestibular-evoked myogenic potentials (cVEMPs). Imaging studies including routine brain and high-resolution temporal bone computed tomography (CT) scans and/or intracranial magnetic resonance imaging (MRI) were available for the majority of injured workers.
Results
Among 4291 head-injured workers with dizziness, 23 were diagnosed with features/findings denoting CVD. Complaints of imbalance were significantly more common in those with CVD compared to vertigo and headache in those with peripheral vestibular dysfunction. Atypical positional nystagmus, oculomotor abnormalities and facial paralysis were more common in those with CVD.
Conclusion
Symptomatic post-traumatic central vestibular injury is uncommon. It occurred primarily following high-impact trauma and was reflective for a more severe head injury where shearing effects on the brain often resulted in diffuse axonal injury. Complaints of persistent imbalance and ataxia were more common than complaints of vertigo. Eye movement abnormalities were highly indicative for central nervous system injury even in those with minimal change on CT/MRI.
Introduction
Vestibular symptoms are common after traumatic brain injury (TBI). 1 Peripheral vestibular structures can be involved at the level of the labyrinth or the vestibular nerve. 2 Trauma can also affect central vestibular structures within the brainstem and their associated pathways in the cerebellum and spinal cord including ascending tracts from the central vestibular nuclei to the supratentorial vestibular cortex. 1 More severe injuries are generally required for physical brain injury to be identified. Nevertheless, white matter abnormalities and diffuse axonal injury have also been reported even in those with mild TBIs.3,4 This article serves to demonstrate that a diagnosis of post-traumatic central vestibular dysfunction (CVD) can be made based on the patient’s presenting history, their physical findings (with specific attention to accompanying oculomotor abnormalities), and/or findings for brain injury on intracranial imaging. Clinicians whose practice involves the care of TBI patients are the target audience. The potential impact of this report is to make clinicians more aware of CVD when encountering a traumatic brain injured patient. Insights from a cohort of head-injured workers with predominant CVD are presented and compared to a cohort with peripheral vestibular dysfunction following head injury.
Methods
The results of 4291 head-injured workers referred to the University Health Network (UHN) tertiary neurotology clinic from the Workplace Safety and Insurance Board, Province of Ontario from 1988 to 2018 for post-traumatic dizziness were evaluated. A waiver of consent was granted by UHN Research Ethics Board (Approval Number: 14-8093).
All head-injured workers underwent a detailed neurotologic history and clinical examination by the senior responsible author (J.A.R.). Audiometry and vestibular function testing with electronystagmography/video nystagmography (ENG/VNG) was performed on nearly all in the study. Vestibular-evoked myogenic potentials (VEMP) studies and video head impulse test were not available for all workers early in the study but were introduced as standard testing when the technology became available.
The normal limit of excitability difference for a canal paresis on VNG (l-Portal VOG, Neuro Kinetics) was set at 15%. VEMPs were recorded using a commercially available evoked potentials system (ICS CHARTR EP 200; GN Otometrics). Cervical and ocular VEMP were elicited via air conduction using a 500 Hz tone. The stimulus was presented at 95 dB nHL (125 dB SPL). The absence of VEMP responses or the presence of an asymmetry ratio >50% in saccular/utricular responses between sides was considered abnormal.
Imaging studies included both brain and/or temporal bone computed tomography (CT) and/or intracranial magnetic resonance imaging (MRI). A diagnosis for post-traumatic CVD was made according to the worker’s injury history, their neurotological findings, the results of vestibular laboratory testing, and imaging abnormalities where predominant neurological dysfunction/anatomic injury was identified. Mechanisms and severity of head injury were based on past iterations from the US VA/DoD Clinical Practice Guidelines updated to 2016 version [Veterans Administration (VA)/Department of Defense (DoD) Clinical practice guideline for the management of concussion/mild traumatic brain injury Version 2.0. (2016)].
Exclusion criteria included workers with a primary diagnosis of headache associated dizziness (including vestibular migraine) and those with preexistent findings for CVD. We purposely did not include those with subjective vestibular perceptual dysfunction more broadly contained under the diagnostic umbrella of a cognitive vestibular disorder in our practice.
Workers with findings for predominant CVD were compared to a cohort with recognized organic peripheral vestibular dysfunction post trauma. 2
Statistical analysis was performed using SPSS 21 for Mac OsX, (SPSS Inc). Chi-square test assessed significance of data difference. The level of significance was P < .05.
Results
CVD Cohort
Twenty-three of 4291 workers were diagnosed with disorders of prominent CVD. All were male; mean age 45.8 years. Mean time between injury and assessment was 16 months (3-64 months). Table 1 shows the mechanism of injury and their occupation.
Mechanism of Injury and Occupation.

Severity of head injury and duration of loss of consciousness (LOC) are presented in Figures 1 and 2. Common reported symptoms included imbalance, “dizziness,” a variety of cognitive complaints, headaches, and tinnitus. “Dizziness” was mostly reported as a constant sense of disequilibrium (7 workers however had a history suggestive for positional vertigo). The most common abnormalities on clinical examination were eye-movement related and problems with gait/balance. In 6 workers (26%), the Dix-Hallpike’s maneuver demonstrated positive findings for posterior canal-based benign paroxysmal positional vertigo (BPPV).

Severity of head injury.

Duration of loss of consciousness.
Eye movement abnormalities were found in 21 (91.3%) workers. The most common eye movement abnormalities identified were saccadic pursuit, an inability to suppress the vestibulo-ocular reflex (VOR) and bidirectional gaze nystagmus. Common presenting symptoms/signs and eye movement abnormalities are listed in Tables 2 and 3.
Presenting Symptoms and Signs.

Eye Movement Abnormalities.

Abbreviation: VOR, vestibulo-ocular reflex.
Eleven workers had skull fractures. Intracranial MRI revealed abnormalities in 20 (87%) workers that included cerebral contusion, intracerebral hemorrhage, subarachnoid hemorrhage, epidural hematoma, and/or diffuse axonal change.
Comparison of Those With CVD (n = 23) Versus Peripheral Vestibular Dysfunction (n = 244)
Disorders of peripheral vestibular dysfunction were identified in 438 of 4291 (10.2%) head-injured workers. Typical posterior canal BPPV was diagnosed in 137 and “other” peripheral type positional vertigo in 57 head-injured workers. Another 244 workers had other disorders of peripheral vestibular dysfunction. Findings from this later group have been published previously. 2 Table 4 provides a comparison between these 2 cohorts exclusive of those with positional vertigo.
Comparison Between Central Vestibular Dysfunction (n = 23) and Peripheral Vestibular Disorders (n = 244) From a Database of 4291 Workers.

Abbreviations: cVEMP, cervical vestibular-evoked myogenic potentials; MRI, magnetic resonance imaging.
Statistically significant.
Mean age was not significantly different in the two cohorts. Those with CVD were all male. They had more severe head injury (P < .0001) and a longer duration of LOC (P = .0004). Complaints of imbalance were significantly more common in those with CVD compared to vertigo and headache in those with peripheral vestibular dysfunction post head injury (P < .0001). Atypical positional nystagmus patterns (not classic for BPPV or “other” peripheral type), oculomotor abnormalities, and facial paralysis were more common in those with CVD (P values .03, <.0001, and .009, respectively). Injury-related hearing loss was not significantly different between groups (P = .1). Skull fracture and intracranial abnormalities were more common in the CVD cohort (P < .0001). There was no significant difference between the 2 cohorts assessing vestibular function with VNG calorics and cVEMP responses (P values .3 and .6, respectively).
Discussion
Head trauma can directly damage the vestibular system from the sensory end organs to central vestibular pathways and their cortical vestibular projections. While diffusion tensor imaging (DTI) studies have demonstrated abnormalities in the brainstem, cerebellar and supratentorial white matter (diffuse axonal injury) in some individuals with mild TBI,5-8 the development of significant CVD usually follows a significant contusion/shearing type injury that involves the vestibular nuclei, cerebellum, and/or central vestibular pathways.
While individuals with acute TBI can demonstrate both central and peripheral vestibular findings, those with purely central findings seem singularly less common.3,4,9 It has been shown that the probability for a common observed peripheral diagnosis such as post-traumatic BPPV increases with severity of head impact. 10
The focus of this study was to investigate head-injured workers who presented with predominant physical findings for CVD. DTI was not available for most of those affected. Twenty-three workers were diagnosed with features of prominent CVD in total. Eighteen had 2 or more vestibular diagnoses including typical positional vertigo from posterior canal BPPV or a peripheral cochleo-vestibular loss in addition. A picture of mixed peripheral and central vestibular involvement was not uncommon.
We acknowledge that the frequency of vestibular diagnoses can be affected by recruitment and assessment method(s) post head trauma. In a prospective study of 150 consecutive patients with severe TBI referred to an in-patient rehabilitation department, the diagnosis of BPPV was confirmed in only 10 (6.6%) patients. The diagnosis was however based on presence of subjective positional vertigo identified in 13.3% and only in this group was a Hallpike’s maneuver performed. 11
By contrast, in a cross-sectional study of TBI subjects admitted to a rehabilitation unit, Harrel et al examined all 73 cases for BPPV without enquiring about the dizziness and found that 60% of the patients tested positive for BPPV despite only 10% of the total cohort having a subjective sensation of dizziness. 12 One explanation for the subjective versus objective discrepancy between studies might relate to the recently characterized TBI phenomenon of “vestibular agnosia” in which brain-injured patients have an obtunded sensation of vertigo. In this regard, Calzolari et al found that acute TBI patients with vestibular agnosia and BPPV were 7 times less likely to be referred for treatment than BPPV patients without vestibular agnosia. 13
The most common presenting symptoms in this central vestibular cohort were imbalance/ataxia (82.6%), followed by dizziness (78.2%) usually reflective for a persistent sense of disequilibrium. There were 7 workers who complained of vertigo in conjunction with historical or physically confirmed BPPV. Episodic attacks of spontaneous vertigo (more typical in peripheral vestibular disorders) were reported in only 1 worker. By contrast, more than 40% of workers diagnosed with a peripheral vestibular disorder excluding BPPV had complaints of spontaneous episodic vertigo. 2 Workers with CVD presented more often with a complaint of persistent imbalance than those with a peripheral vestibular disorder (72% vs 32%, P < .0001).
Gate ataxia/imbalance remains a common feature in acute severe TBI. 14 Imbalance post head injury is considered by some to represent a pattern first reported by Thomas Brandt in acute peripheral vestibulopathy patients 15 , that is, patients were more stable walking than standing still. Calzolari et al demonstrated that the majority of TBI patients had central vestibular ataxia and the degree of imbalance correlated with widespread bilateral and predominantly frontal white matter microstructural parameters on DTI. 13
In our experience, VNG remains a helpful tool as it assesses certain aspects of both central and peripheral vestibular function. Oculomotor abnormalities including findings of atypical post headshake nystagmus (ie, cross coupling), failure of fixation suppression (together with a failure to suppress the VOR clinically), and atypical positional nystagmus seemed helpful in differentiating central from peripheral lesions. More than 91% of our cohort with CVD had a recognized oculomotor abnormality clinically.
Eye movements to a large degree are a mirror reflection of central nervous system (CNS) function.16,17 As such, a careful oculomotor examination can be a used as a proxy or screening measure for CNS function independent of vestibular function testing. Abnormal oculomotor function (eg, saccadic dysmetria, gaze-evoked nystagmus, saccadic pursuit, etc) are nonspecific considerations for injury to CNS pathways that involve the cerebral hemispheres, cerebellum, and brainstem. Pathways for fixation suppression of the VOR additionally require intact connections between the vestibulocerebellum and the vestibular nuclei.
A limitation when relying on oculomotor test abnormalities as a proxy for definite central pathology requires the consideration of related medication effects (especially anticonvulsants) on the CNS.18,19 Only 1 patient in our central vestibular cohort however was taking an anticonvulsant (phenytoin) for seizure control.
Post headshake nystagmus (from testing in the horizontal) was present in 2 of the central cohort. One had down-beating nystagmus (ie, termed “cross coupling”) and the other with a moderate caloric reduction had longer than expected horizontal nystagmus directed away from side of lesion 20 The presence of headshake nystagmus in this worker speaks possibly to an uncompensated peripheral vestibular loss in association with a postulated central injury (a central velocity storage abnormality) or the phenomenon of head jolting nystagmus. 21
Thirty percent of workers with CVD had an abnormality on caloric and cVEMP testing. This was felt more likely to be the direct effect of trauma to the peripheral vestibular system. A paretic response typically indicates injury at some point along peripheral vestibular pathways from the labyrinth to the vestibular nuclei. Vestibular nuclear injuries however can be both central and peripheral in their presentation (ie, Wallenberg’s syndrome). Abnormalities in the caloric test coupled with loss of visual fixation suppression however would be more suggestive for central pathology.14,17,22,23
Vestibular rehabilitation therapy may play a role in increasing an affected individual’s functionality. Nevertheless, our experience is that the benefits seemed limited compared to those with a stable peripheral vestibular loss.23,24 Accordingly any return to workplace activity remains similarly guarded.
We acknowledge the limitations of this study. It is retrospective with all its inherent limitations. The strength of our study however is based on the large number of cases that received extensive investigation and were assessed by the senior responsible author in the same unit and in a consistent fashion.
The main weaknesses beyond the retrospective nature of the gathered data included referral bias possibly engendered by vestibular agnosia (which paradoxically could have reduced referrals for more severe TBI patients not complaining of dizziness/vertigo); the duration between injury and assessment; whether all patients completed a systematic laboratory battery of testing (since subjective symptoms correlate poorly with objective deficit in acute TBI3,13); and paucity of longer term follow-up data to denote improvement either on clinical examination or laboratory testing. Furthermore, there are few laboratory tests for vestibular perceptual function which is part of central vestibular function. The cohort numbers of those with recognized CVD was relatively small compared to those with a primary peripheral vestibular disorder post trauma. The definition of post-traumatic CVD was primarily based on overall clinical findings for which other possible explanations (ie, unrecognized preexistent central pathology) might have been present and positive MRI findings for central pathology that can also found in those without evidence for oculomotor or VOR suppression abnormalities. The absence of agreed on specific ICD-10 codes for reporting purposes 25 and the limited number of publications available for review pose further difficulty knowing whether our findings were primarily institutionally based or whether they can be generally applied. Finally, those with central vestibular syndromes post head injury not infrequently had evidence for peripheral vestibular dysfunction which unfortunately further blurs the lines for a clean demarcation from the effects of trauma on the vestibular system. Comparing our 2 cohort groups would likely need to take into account the aforementioned and the rank difference in magnitude between the 2 cohorts. Nevertheless, despite these concerns, there was a significant statistical difference between central versus peripheral vestibular syndromes in terms of their symptoms (ie, imbalance/ataxia), severity of injury (typically more severe), duration of LOC, their related physical findings (ie, facial nerve paralysis, skull fracture, oculomotor dysfunction, atypical positioning nystagmus), and relative MRI abnormalities.
Conclusion
Symptomatic post-traumatic CVD is uncommon. It occurred primarily following high-impact trauma and was reflective for a more severe head injury where shearing effects on the brain often resulted in diffuse axonal injury. Complaints of persistent imbalance and ataxia were more common than complaints of vertigo. Eye movement abnormalities were highly indicative for CNS injury even in those with minimal change on CT/MRI.
Footnotes
Authors Contributions
John Alexander Rutka: design/conception, final review, and editing of the paper.
Mordechai Kraus: literature review.
Sasan Dabiri: literature review, revised the work, reviewed the paper, and helped with the statistics.
Gabriela Vergara: interpretation of data, reviewed the paper, and helped with the statistics.
Fatemeh Hassannia: literature review, data analysis, and wrote the first draft.
All authors contributed to the manuscript substantially and have agreed to the final submission version.
Availability of Data and Materials
The data that support the findings of this study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
A waiver of consent was granted by the University Health Network Research Ethics Board (Approval Number: 14-8093).