
Abstract
This is the protocol for a Campbell systematic review. The objectives of the present review are to answer the following questions: (1) To what extent to medical students experience racism in educational/clinical settings? (2) What are the impacts of racism for medical students in educational/clinical settings?
Background
The Problem
Prejudice or discrimination against someone on perceived differences based on skin colour and/or ethnic background constitutes racism. Racism as experienced and witnessed by medical students during their education is an important issue worldwide (Morrison et al., 2019). Theories critical on race and racism have denoted that racism can manifest in a number of different ways, from overt acts of racism on an individual level, to less clear forms of prejudice that occur at an institutional and system level; other ways that racism may occur, often in ways that are not as clearly obvious, are racial microaggressions, implicit and explicit bias, and covert forms of racial prejudice and/or discrimination (Ford & Airhihenbuwa, 2010; Needham et al., 2023). While experiences of racism in healthcare settings have been increasingly studied and understood, the experiences of students in a health profession are poorly recognised (Hamed et al., 2022).
The health impacts of racism have been studied extensively and it has been demonstrated that racism can have negative consequences on overall health (Devakumar et al., 2022). Racism has negative impacts on the health and wellbeing of the individual, as well as on society in professional and communal environments. Experiences of racism are correlated with increased mortality and poor mental and physical wellbeing, no matter the stage of life (Devakumar et al., 2022; Selvarajah et al., 2022). Pertinent to the usual age of medical students, adverse health outcomes associated with racism in late adolescence to early adulthood include asthma, hypertension, stroke, diabetes, and increased cancer risk pathologically; anxiety, depression, post-traumatic stress disorder, somatoform disorders, and suicidal ideation psychologically; and maladaptive coping mechanisms such as tobacco, alcohol and substance abuse behaviourally (Selvarajah et al., 2022).
Specific to healthcare education, incidents, behaviours, and training that occur in medical school can significantly impact the trajectory of one’s medical career (Joseph et al., 2021). Sources of racism in healthcare education settings include fellow medical students, teachers, healthcare placement staff and the racial bias inherent in the medical curricula. Experiences of racism and racial bias in medical education have significant health impacts on students’ physical and mental wellbeing. Such experiences may result in poorer academic outcomes, high attrition rates, reduced career satisfaction and ultimately diminish racial diversity in the future healthcare workforce (Joseph et al., 2021). Based on the potential likelihood of racialised incidents occurring during this period, it is vital to understand racism in medical education to highlight appropriate areas for practical intervention.
Medical institutions’ responses to racism in medical education are varied and diverse, including anti-racism policies and statements, diverse recruitment strategies, curriculum reforms and robust reporting mechanisms. For example, the Australian Medical Association has released a statement of anti-racism, stating that no doctor or student should experience any type of harassment or vilification based on ethnicity at work or while learning. (Australian Medical Association, 2018). Similarly, some medical schools have developed anti-racism initiatives spanning across the curriculum, medical recruitment, and student community through creating safe space events and dialogues. (Harvard Medical School, 2024; Icahn School of Medicine at Mount Sinai, 2021).
Guidance regarding the necessary components of an anti-racist approach for educators of health professionals is needed. In their systematic review, Garneau et al. (2023), highlight that an anti-racist education can reduce racialised perspectives in educational settings, but this alone is not adequate – there must also be an understanding of power dynamics, having a critical consciousness towards racism and its impacts, and advocacy for action occurring among both organizations and individuals (Garneau et al., 2023). Additionally, the San’yas Indigenous Cultural Safety Training program provides further insights into how anti-Indigenous racism can be addressed in educational settings through pedagogical change. The program specifies educators need to have core competencies in terms of knowledge, self-awareness, and the need to confront and address micro-aggressions, emotionality, resistance, and personal triggers. Furthermore, Indigenous perspectives need to be emphasised in these educational settings (Ward et al., 2021).
While these guidelines and recommendations exist for health professionals, to date, the extent to which many medical curricula describe the health and social impacts of racism, as well as the way students are educated in how to address racism in clinical settings, has not been well documented. However, some studies have examined the extent of racism and teachings regarding racism in health pedagogy more broadly. For example, Evans et al. (2022) discuss how a culture of white supremacy and whiteness is not acknowledged in health education settings across the United Kingdom, and this results in ineffective approaches to addressing racism in these settings (Evans et al., 2022). As well, a previously published systematic review describes how teaching about structural racism has become a common topic in public health education across the United States since 2006, but the extent of this teaching in medical education was shown to be quite limited (Chandler et al., 2022).
In this systematic review, we will examine the lived experiences of racism in medical education and training, guided by the definition of racism being constituted of prejudice or discrimination against someone based on their race. We will explore the phenomenology of racism among medical students, including experiences witnessing, experiencing, or learning about racism through reviewing both quantitative and qualitative studies. In doing so, we will aim to understand medical students’ experiences with racism in healthcare, and its impacts on future clinicians and their future patients. Overall, this work will help further explore the extent of racism in medical education and identify the impacts of it on students during their education and beyond, helping to identify the areas of need for future work to be directed to minimise racism in educational institutions.
Why it is Important to do This Review
Experiences of racism in medical education are prevalent but underreported due to inadequate and inappropriate reporting mechanisms (Lucey et al., 2017; Mensah, 2017; Okwerekwu, 2016). In Australia, Aboriginal and Torres Strait Islander medical students were reported to be more likely to experience racism compared to other students (Wu et al., 2013). In the United States, experiences of racism have been suggested to increase burnout and stress in medical students (Dyrbye et al., 2007). A scoping review focusing on the UK medical education system found that there is a high prevalence of racial discrimination and harassment, with most medical students feeling unsupported in navigating through this by their medical faculty and educators (Montasem et al., 2023).
The issue of racism and discrimination experienced by medical students around the world may be widespread, with long lasting consequences, yet reviews regarding this topic are limited. To our knowledge, there have been no systematic reviews on this topic with a global focus. Prior reviews have largely focused on discrimination in a broader sense, with inclusions such as gender and sexual discrimination, bullying, and other forms of harassment (Fnais et al., 2014; Ng et al., 2020). For example, a systematic review published in 2014 found that 54% of medical trainees had experienced discrimination and harassment in their education; however, it did not further define the types of harassment experienced (Fnais et al., 2014). This gap in the literature necessitates an investigation of the specific impact that experiences of racial discrimination have on medical students. If racial minority students’ negative experiences of racial harassment in medical school leads to burnout and possible attrition, this has significant effects on the diversity of the future workforce and therefore potentially impacts the healthcare system.
Understanding experiences of racism among medical students through an evidence-based approach is crucial to inform future policy and reforms on diversity, equity and inclusion. Such research helps to identify any pre-existing and newly developing trends within a broader social context and identify any groups that might require more support, as has been pointed out by previous studies (Claridge et al., 2018; Hill et al., 2020). This allows medical schools, academic or teaching hospitals as well as other learning environments (such as General Practitioner clinics) to design new methods or adapt strategies used previously to provide more appropriate and culturally safe teaching and training experiences for their medical students (Lynn et al., 2023).
Strategies that healthcare institutions may employ to provide appropriate training for medical students are varied. For instance, medical schools may be required to include respectful behaviour as part of the professional requirements component of the curriculum. Furthermore, they may also be able to provide accessible and robust reporting pathways within clinical and academic settings, and ensure outcomes for support, remediation and discipline in incidents are appropriate, transparent, and clearly communicated. However, the extent to which medical students receive education on the impacts of racism, and how to address racism in clinical scenarios, also remains poorly understood. This review may also support future developments and reviews of diversity, equity and inclusion policies and interventions for healthcare institutions and specialty medical colleges.
Despite actions and initiatives across universities, minority students globally still face racism in medical education settings from a variety of sources, such as patients, educators, and community members. The need for this review is to further identify experiences of racism in medical schools and clinical learning environments and its impacts. In doing so, we aim to further understand and characterise these experiences. This is paramount in helping institutions develop specific strategies in overcoming barriers to better support their students and prevent experiences of racism. As, to our knowledge, there has been no prior review on this topic, we believe that conducting this systematic review will make important contributions to the overall literature. Though recommendations on deconstructing racism in medical studies are under development, considerably more evidence is required globally to effectively develop such guidelines, and to ensure the well-being of all future medical practitioners (Green et al., 2021).
Objectives
For this review, the goals are in relation to medical students and their experiences of racism and/or racialised encounters for medical students, and the impacts of this in educational settings.
Therefore, our objectives for this systematic review are the following: • To describe the extent of racism witnessed or experienced by medical students in educational/clinical settings. • To explore the impacts of racism for medical students in educational/clinical settings.
Methods
Criteria for Considering Studies for This Review
Types of Studies
For this review, we aim to have a wide array of study methodologies to be eligible for inclusion to ensure that as many relevant studies as possible are included. Therefore, case-control studies, cohort studies, randomized-control trials, cross-sectional studies, quasi-experimental studies, qualitative studies, mixed-methods studies are all eligible for inclusion in this review. While studies with control groups will offer useful insights, it is not required for studies to have controls. Qualitative studies, including interviews and focus groups, will be eligible. Our analysis may separate qualitative and quantitative findings, as required.
Articles with non-original research, such as editorials/commentaries and reviews, will also not be eligible for inclusion.
Types of Participants
Participants in included studies can include medical students, as well as graduates of medical school who describe their experiences of racism in medical school, or who describe the impacts/knowledge that they gained about the detrimental aspects of racism whilst in medical school. Studies that focus on acquiring information from medical school staff regarding teaching of racism in medical school will not be eligible for inclusion. The reason for this is to minimise desirability bias that may come from medical educators and representatives of medical schools.
Types of Interventions
Interventional studies that focus on improving knowledge of racism or improving the well-being for medical students (who may, or may not have experienced racism), as well as those which aim to provide support to medical students who have experienced racism are eligible for inclusion in this review. However, it is important to denote that our review is not explicitly aiming to focus on the impacts of interventions – instead, it is to evaluate the experiences that individuals have had with racism, and the associated impacts.
Types of Outcome Measures
There are numerous important outcome measures to be evaluated in this review. These are as follows: • Number of racist events experienced, stratified by sub-populations (including by geographical location and racial/ethnic background). • Type of racist event(s) experienced, such as (but not limited to) microaggressions, overt racism, implicit bias, and institutional racism. • Psychological impacts (e.g. stress, negative self-perceptions) of racist experiences. • Qualitative experiences after having gone through racism/witnessed racism. • Impacts of racism on student’s progression through educational institutions. • Social impacts (e.g. feeling culturally safe, being able to connect with others).
Search Methods for Identification of Studies
Electronic Searches
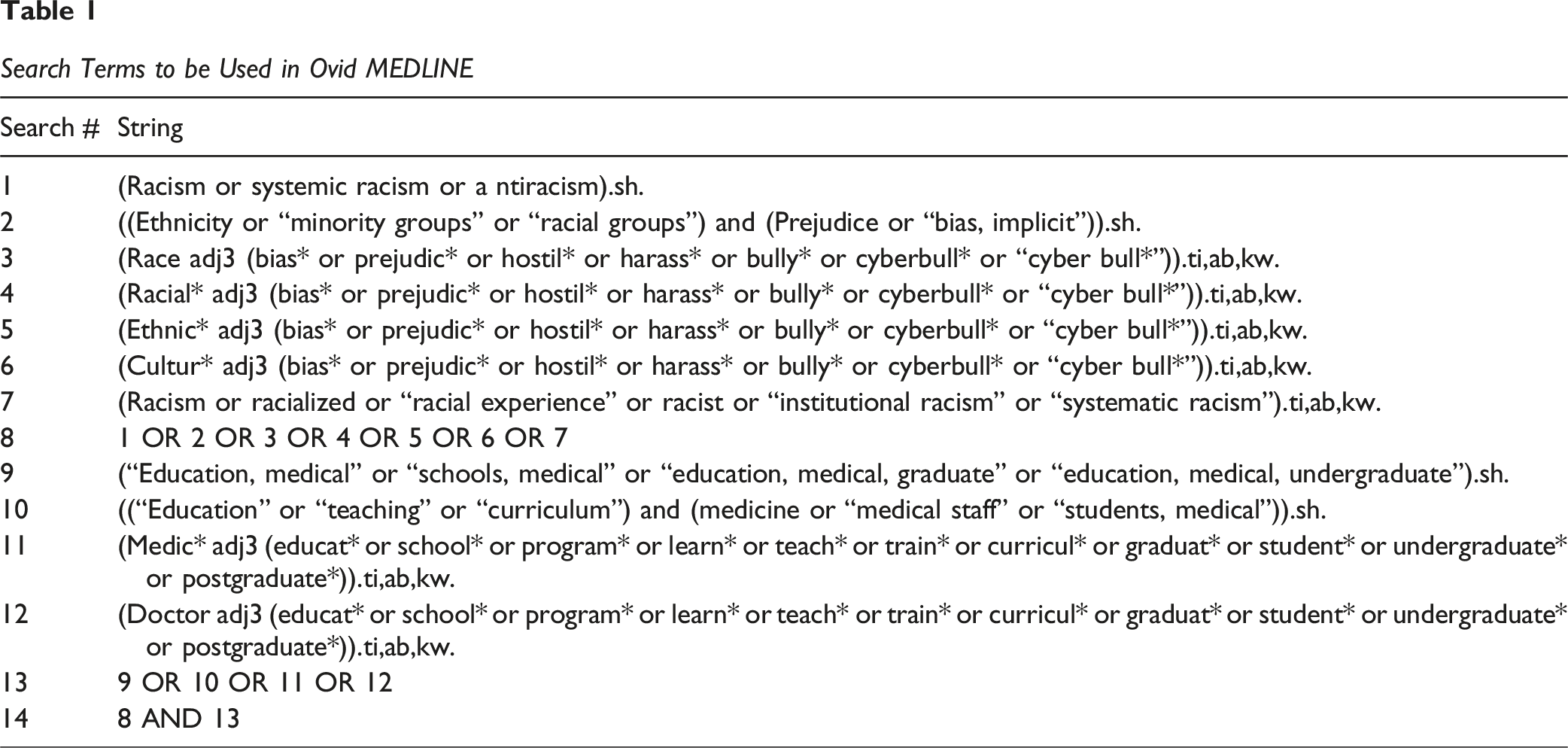
The process for identifying and retrieving articles in this review has followed the new search guidance for Campbell systematic reviews (MacDonald et al., 2024). As suggested in the guidelines, a librarian (author H-L.O.) with numerous aspects of development of this review protocol; these include but are not limited to: selecting databases to search, designing search strategies, running searches, saving in appropriate formats, ensuring reproducibility, drafting the search methods, and obtaining full texts when required.
Search Terms to be Used in Ovid MEDLINE
Searching Other Resources
To maximise the number of potential articles found, reference lists of included studies will be scanned for additional studies to potentially include. Excluded reviews will be marked and have their references scanned to further increase the number of potential articles if not already captured in the search criteria. Reference lists of prior reviews will also be evaluated for additional articles. Existing reviews and meta-analyses, will also be identified via Cochrane Library and Campbell Systematic. Furthermore, we will also use Google Scholar for the purposes of conducting forward citation searching for the included studies. More precisely, to identify any additional relevant articles after completing initial screening, we will enter each article into the Google Scholar database and thereafter assess articles that cited the included studies; these additional studies will also be assessed for eligibility.
Hand searches of relevant journals will also be conducted in this review to capture as many relevant articles as possible that may have been missed during the initial screening process. These journals will be MedEdPortal, Medical Education, Academic Medicine, Medical Teacher, Advances in Health Sciences Education, Teaching and Learning in Medicine, The Clinical Teacher, Journal of Graduate Medical Education, Perspectives on Medical Education, and Advances in Medical Education and Practice. Keyword searches of “racism” (and if applicable “medical education”) will be used for these journals; extensive search terms with Boolean operators will not be possible for these journals with limited searching options. As well, where feasible, experts in the field will be contacted to determine if any additional relevant studies have been missed during the screening process.
Conference proceedings and dissertations are not to be included in this review. This is mainly to ensure the highest possible level of quality of works included that have undergone extensive peer-review, and – considering the complexities of this topic that has many nuances that require extensive explanations – have complete texts with appropriate level of details. For these reasons, we have also excluded government documents from this review as government documents frequently do not undergo the traditional peer-review process of academic literature, and so there will be great difficulty in verifying the rigorousness of the research process – especially when compared with the academic articles to be included in this review.
Data Collection and Analysis
Selection of Studies
Selection of studies for this systematic review will follow the Preferred Items for Systematic Review and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). Once searches have been completed across databases, duplicates will be removed. Next, studies will be screened by title/abstract to determine eligibility. Thereafter, studies will be screened by full text to determine the final eligible articles for inclusion. This process will be completed independently by at least two reviewers; discrepancies for final included articles will be resolved by consensus amongst three authors. The entirety of the screening process will be depicted in a PRISMA flow diagram, and this will show the justifications for exclusion of articles during full-text analysis.
In terms of eligible studies, this review will include studies from as diverse methodologies as possible. There will be no restrictions placed based on date of publication, location of study, or sample size. All included studies must be available in English. The reasoning for only included English-language publications is that the authors’ only competent language for evaluating full-text is English.
Studies must be peer reviewed to ensure included data is of high quality. This promotes reliability of data and minimizes bias; therefore, grey literature will be excluded for reasons already discussed. Additional requirements for studies will be based on whether they address this review’s primary objectives. To be eligible for inclusion, the study must meet at least one of the following: • Includes stratified data for medical students – in any year of training (pre-clinical or clinical) – that describes or quantifies their experiences witnessing, experiencing, or learning about racism. While this is a requirement for included studies, it is not required that studies themselves exclusively focus on racism; for example, if they focus on discrimination, but have stratified data regarding racism experienced by medical students, then the study would be eligible for inclusion. • Includes medical graduates who describe their experiences of racism as a medical student and/or describe the focus of racism in their medical education.
Studies that focus on other health students (e.g. nursing, clinical psychology) will not be eligible for inclusion if they do not provide stratified data for medical students. Furthermore, to minimise bias, studies that focus on obtaining information directly from medical educators about the extent of education regarding racism in medical school will not be eligible for inclusion in this review.
As our review is aiming to specifically focus on racism and its impacts, studies focusing solely on discrimination will not be eligible unless they explicitly make racism/racialised experiences their focus. Furthermore, studies that evaluate a focus on discrimination and/or prejudice in medical education will not be included unless they specifically focus on racism. As well, studies that solely focus on racial disparities, or reducing racial disparities, will not be eligible for inclusion as this is outside the scope of our review.
To better guide the type of data that will be extracted and its interpretation, particularly in regards to what constitutes racism, and other hardships faced by racialized minorities, we will utilise Critical Race Theory (Ford & Airhihenbuwa, 2010), and Needham et al.’s (2023) framework on institutional racism and health; these frameworks have been utilised in the past to allow for more nuances in understanding the types of racialized experiences that minorities face, and the differing impacts of these. These include overt acts of racism, but also include implicit/explicit bias, racial prejudice, institutional racism, systemic racism, and interpersonal racism.
Data Extraction and Management
After articles are selected for inclusion, at least two reviewers will independently extract data from included studies. Discrepancies in data extraction will be resolved by consensus amongst three authors. Data extraction will be broken down into three main categories, and presented in tabular format: study characteristics, study findings. For study characteristics, the following data will be extracted: year of publication, location (city, country), study design, study objectives, sources of data, number of medical students included, and focus of study (either evaluating extent of racism, or knowledge of racism).
In terms of study findings, the following data will be extracted: year of publication and location, number of medical students, student demographic data (such as gender breakdown, age), ethnicities of students, key findings regarding experiences/knowledge, types of racism encountered/experienced (e.g., microaggressions, exclusion), institutional responses., impacts of the racism, additional findings of the study, and study recommendations. To adequately assess, and capture, data across diverse populations, data will be categorised and stratified for subgroups based on geographic location and self-identification of ethnicity or race. We acknowledge that certain groups may remain underrepresented in publications despite this subgroup stratification and recognize this form of publication bias serves as a potential limitation of our review.
Assessment of Quality of Included Studies
To assess overall study quality in this review, the Joanna Briggs Institute (JBI) critical appraisal tools will be utilised. These specific tools will be utilised as they provide multiple critical appraisal checklists for a wide array of study methodologies, which will be particularly relevant for this review. For the purposes of evaluating quality across studies included in this review, we will follow approaches that have been taken in a number of prior studies, (Adalbert et al., 2021; Bowring et al., 2016), and adapt the JBI tools to utilise a numeric score (which will serve as a means of ranking) for studies based on the number of “yes” and “no” responses for the critical appraisal checklist.
Data Synthesis
Trends in qualitative data will be described separately from quantitative data as needed. As per the BMJ Synthesis without meta-analysis (SWiM) in systemic reviews reporting guide (Campbell et al., 2020), studies will be grouped by self-identified ethnicity and geographical location so that experiences can be grouped where possible. Relevant odds ratios/risk ratios will be reported as a meta-analysis will not be possible given studies across numerous methodologies are expected to be included, and based on this, it is also expected that the data from the included studies will be highly heterogeneous. The heterogeneity will be investigated by including tables with characteristics to highlight subpopulations such as age, sex and self-identified ethnicity, and included studies will be referenced.
Summary and Dissemination of Findings
The most pertinent findings, as well as gaps in the literature, regarding medical student experiences with racism, and education of racism in medical school, will be summarised in this review. Based on these findings, implications for future research, medical education, medical school policy, public health, and the medical field more generally, will be described and recommendations will be made based on these. These findings can therefore have important implications in guiding the ongoing improvement of medical pedagogy, as well as for improving the health outcomes and lived experiences for racialised minorities inside, and outside, of medical school.
The findings of this review will be disseminated via presentation in conferences, as well as in workshop and medical education settings. Furthermore, the work will be published in a peer-review journal. The authors will also aim to share the findings with advocacy organizations within medical schools, along with organizations that seek to restore racial justice in broader society, and to help guide interventions and policies that can address racial injustice.
Conclusion
While racism has been recognised as a problem across societies and can be a contributor to both poorer health outcomes and poorer experiences with the healthcare system, there remains a lack of synthesis in literature regarding experiences, and impacts, of racism in medical school. Therefore, this review has an important role in providing an understanding of racism in medical school. This work will offer important insights regarding the development of medical school pedagogy, the impacts of racism, and the need to enact change as a means of addressing the public health issue of racism.
Supplemental Material
Supplemental Material - Experiences & Impacts of Racism During Medical School: A Systematic Review Protocol
Supplemental Material for Experiences & Impacts of Racism During Medical School: A Systematic Review Protocol by Karan Varshney, Mariyah Hoosenally, Jacqueline Rusnak, Charlie Ho, Damian Bradley and Hannah-Lee Obst in Campbell Systematic Reviews.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.