
Abstract
Background
Exercise is beneficial for persons with Huntington's disease (HD). Inpatient rehabilitation settings are well-suited for implementing exercise programs. Exercise parameters, such as duration and intensity, need to be further investigated. The objective of our study was to evaluate the effects of an exercise program at moderate intensity performed five times a week for persons with mid-stage HD during a four-week inpatient rehabilitation program.
Methods
In a single-blind randomized monocentric controlled trial, two groups followed a four-week inpatient rehabilitation program including: occupational therapy, psychomotor therapy, psychosocial workshop, mobility sessions, dietary management, nursing, socio-educational activities, physician consultations and personalized consultations. In addition, the intervention group specifically participated in five one-hour exercise sessions per week at moderate intensity (flat ground walking, sand walking, resistance training, adaptive cycling and water activities), whereas the control group engaged in specific activities without physical activity. The primary outcome was the UHDRS-modified Motor Score (mMS). Functional, cognitive and psychological assessments were also completed.
Results
Thirty-two patients were recruited. The UHDRS-mMS did not significantly differ at post-intervention. In the intervention group (n = 16), within-group improvements were observed for HAD-Anxiety, PBA-apathy, PBA-depression, PBA-psychosis; both within and between-group for 6-min walk test, Stroop Word Reading, and PBA-executive function; and between-group only for Borg. The control group (n = 16) improved within-group on PBA components: depression, apathy and irritability.
Conclusions
Inpatient rehabilitation program had positive effects on psychological symptoms, while exercise produced additional positive effects beyond exercise tolerance, anxiety, STROOP Word Reading and executive function. Inpatient rehabilitation programs may require longer-term post-rehabilitation support.
Trial registration
NCT04917133
Introduction
Huntington's disease (HD) is a rare dominantly inherited monogenic neurodegenerative disorder affecting the brain, ranging from a non-pathological form to severe motor, cognitive and behavioral symptoms.1,2 Disease symptoms typically begin in the third and fourth decades of life. As in other rare diseases, the multidisciplinary approach offered by specialized clinical centers represents a strategy likely to overcome these symptoms and is awaited by HD families. 3 In 2014, in 121 sites taking part in the Enroll-study, 54% of centers used a multidisciplinary approach. 4 Indeed, multidisciplinary care appears to demonstrate benefits when pharmacological treatments, rehabilitative treatments, and appropriate social settings are associated.5,6
As a mainstay of multidisciplinary care, 7 exercise programs are safe and provide significant benefits in persons with HD demonstrated by clinical outcomes6,8–11 and by physiological biomarkers. 12 Reviews of studies have indicated that exercise interventions in HD have consistently been shown to provide benefits in motor outcomes, such as gait speed, balance and cardiovascular fitness.8,11 More specifically, patients who participated in a 12-week multimodal exercise intervention showed a reduction of 2.9 points in the UHDRS modified Motor Score (UHDRS-mMS). 13 A comparable effect was observed, with patients completing an 8-week home-based intervention showing a 2.3-point reduction in the UHDRS-mMS. 14 Evidence for cognitive improvements is less consistent, with some studies suggesting positive effects on learning and memory, while others report no significant changes.9,10 Regarding psychological outcomes, exercise can help maintain or modestly improve quality of life, for instance, qualitative reports highlight enhanced well-being,8,9,15 however effects on depression and anxiety remain uncertain.8,10 Thus, recommendations emerged for persons with HD: aerobic exercise paired with strengthening exercises benefits to improve fitness and motor function, and one-on-one supervised gait training to improve spatiotemporal measures of gait, with Grade A evidence. 16 Despite these recommendations supporting physical exercise, the implementation of structured physical exercise programs requires specific expertise, particularly in persons with HD. In routine clinical settings, this may lead some rehabilitation programs to prioritize activities that are less physically demanding and easier to supervise. A clinical practice survey indicates that clinicians with HD expertise frequently use interventions such as stretching and range of motion exercises, 16 which are generally regarded as easier to implement in routine care.
Inpatient multidisciplinary rehabilitation provides an ideal setting for integrating an exercise program, allowing for daily monitoring within a structured and controlled therapeutic environment. 17 These settings promote high adherence to the intervention offered 18 and ensure safety and adaptability with the supervision of all healthcare professionals. The beneficial effects of exercise have been shown during inpatient rehabilitation programs among persons with HD.18–21 These few studies implemented inpatient rehabilitation programs lasting three weeks and offered daily exercise sessions. More specifically, studies by Piira et al. and Zinzi et al. have repeated these rehabilitation cycles several times throughout the year. Importantly, in the study of Zinzi et al., 19 improvements in motor function, functional abilities, and quality of life were observed at the end of each three-week cycle, demonstrating the benefits of each intervention period. In the study of Piira et al., 20 the benefits of each 3-week rehabilitation cycle can be observed and were associated with improved balance, gait function, physical quality of life and with reduced symptoms of depression and anxiety. Within these inpatient rehabilitation studies, none included a control group and specific details regarding the duration and intensity of the exercise components were not always fully specified. Overall, the results reported to date in physical therapy for persons with HD have emerged from studies using a wide variety of exercise protocols, sometimes without a control group. 9 While interventions predominantly use supervised and self-directed exercises, components such as the time, intensity and frequency of programs are heterogeneous, 10 especially in inpatient settings.
The work undertaken in this study was therefore specifically aimed at generating further evidence to support the justification for integrating exercise into the existing rehabilitation model. By comparing an intensive multidisciplinary program with and without a structured exercise component in an inpatient setting, our objective was to examine whether exercise provides additional benefits beyond those achieved through the rehabilitation approaches currently used in the control group. This approach is based on several key elements: an evidence-based intervention, a high frequency of sessions (five per week), a strong adherence expected from participants given the inpatient setting, and supervision of every session by a qualified professional 22 to ensure safety, optimal engagement, adaptability, and a moderate exercise intensity. To address this aim, we hypothesize that patients with HD receiving a structured exercise program within an inpatient multidisciplinary setting will show greater improvements in UHDRS-mMS, motor, cognitive and psychological outcomes compared to usual care.
Materials and methods
Patient selection
According to the HD-Integrated Staging System (HD-ISS), 23 all subsequent patients at mid-stage of HD (stages 2 and 3) were screened for inclusion at entry in a specialized 11-bed clinical rehabilitation unit hosting exclusively persons with HD in inpatient hospitalization.
According to the National Research Ethics Committee recommendation (N°ID-RCB: 2021-A00423-38), both the participants and their caregiver, when any, signed informed consent upon arrival with the study coordinator. Legal guardians had to sign the consent form if guardianship was involved. Patients had to meet the following inclusion criteria: (1) middle-stage HD with the ability to walk independently for 10 meters, (2) aged at least 18 years, (3) unchanged medication and diet for at least four weeks before enrollment, (4) informed consent and (5) social security affiliation. The exclusion criteria were: (1) a physical or psychiatric condition impairing the completion of the program and assessments, (2) a history of additional major neurological or orthopedic disorders impairing mobility, (3) difficulty understanding or reading French and (4) legal protection for incapable adults. The presence of a caregiver was not mandatory.
The following characteristics were obtained for our study population: sex, age, height, weight, time since diagnosis, time since onset of symptoms, presence of a caregiver and Montreal Cognitive Assessment (MOCA) score. The MOCA score 24 was used, only at baseline because of a learning bias, to describe the population's cognitive function.
Power calculation
A priori power analysis was conducted using G*Power software to determine the required sample size for detecting changes in UHDRS-mMs. Based on an effect size of 1.1 for UHDRS-mMS reported in the study by Khalil et al., 14 which features a total number of structured exercise sessions similar to those in the present study (k = 24), an alpha risk of 0.05 and a statistical power of 0.85 indicated a required sample size of 26 participants (13 per group). With a loss to follow-up rate of 15%, the inclusion of 16 participants per group means that the study can be considered complete.
Randomization process
Computerized randomization was centralized through a secure Internet facility (CleanWEB©, Telemedicine Technologies S.A.). Randomization was performed at the inclusion visit (V0) without stratification on the basis of the Total Motor score of the Unified Huntington's Rating Scale (UHDRS®, HSG 1996). The randomization sequence was generated ensuring that investigators and participants were blinded to group allocation. A random permutation of block sizes of 2 or 4 was used to ensure balanced distribution of the intervention groups. The random permutation of 2 or 4 blocks avoids excessive predictability while maintaining a good balance between groups, with approximately 6 to 8 participants each during rehabilitation. The block size was randomly chosen to prevent allocation guessing. Investigators enrolled participants and accessed group assignments only after inclusion and completion of the UHDRS to preserve allocation concealment.
Intervention
Patients were equally and consecutively randomly allocated to an intervention group or a control group. During 4 weeks in an inpatient rehabilitation program, both groups followed a rehabilitation program with common activities including socio-educational activities, cognitive rehabilitation, mobility sessions, psychosocial workshop, dietary management by a dietician, nursing, psychomotor therapy and occupational therapy, to provide a holistic and recommended rehabilitation. 7 A physician coordinated and facilitated the work of the multidisciplinary team, as recommended. 7 All the professionals worked closely together and interacted within the group. The dietary management, one per week, followed the Nutritional Standards Guidelines of Brotherton and collaborators. 25 If necessary, a consultation with a dentist was carried out.
During this inpatient setting, the intervention group participated specifically in an exercise program of five sessions a week: flat ground walking, sand walking, resistance training and adaptive cycling. The 5th exercise session of the week was a water activity such as surfing, diving or kayaking. Each session lasted one hour with a frequency of one daily session, five days a week, followed by two days of recovery. The number of exercise sessions (k = 20) was similar to that in Khalil et al.'s study (k = 24). 14 The exercise sessions were performed at moderate intensity and were modulated according to the patient's status of fitness, fatigue and perceived exertion. In practice, this meant that the duration of the task could be slightly reduced for an individual participant if needed, for example, by allowing longer rest periods, without changing the overall schedule for the group or skipped sessions. Additionally, it was possible to slightly decrease the intensity of the task for a participant when fatigue or exertion levels required it, while still maintaining the intended structure of the intervention, and ensuring that no session was skipped. This exercise program was based on recent physical activity recommendations for persons with HD. 16 To check whether moderate intensity had been reached, kinesiologists used the Borg Rating of Perceived Exertion (RPE) scale (CR10) several times to assess perceived exertion during the core part of the exercise session, as used in the study of Khalil.14,26 For this study, moderate intensity was defined as a Borg CR10 rating of 4–6, where 1 indicated “no effort perceived” and 10 represents “maximum effort perceived”. Dietary management was carried out to control each participant's diet and prevent weight loss, which could result from the energy expenditure associated with regular physical activity.
During this inpatient setting, participants of the control group engaged in specific activities (without physical activity or high energy expenditure). Hydrotherapy, horse mediation, additional psychomotor therapy (focused primarily on emotional and physical relaxation) and cultural/social activities were performed once a week in the control group during the five exercise sessions of the intervention group to match the time range for social (interpatient) and care interactions. A description of the rehabilitation and exercise interventions (frequency, intensity, duration and type) for both groups is available in supplementary files (N°1) and (N°2).
Assessments
The primary outcome was the modified Motor Score (mMS) of the Unified Huntington's Disease Rating Scale (UHDRS), 27 a composite score that includes only voluntary movements of the UHDRS Total Motor Score (UHDRS-TMS). 28 The patients’ functions were evaluated before and after their rehabilitation by experienced neurologists, who were external to the research project and blinded to whether the patients were in the intervention or control group.
The secondary outcomes included physical, functional, cognitive and psychological measurements. Testing conditions were standardized; only the assessor potentially varied. The outcome measures of physical function were static and dynamic balance (Berg Balance Scale 29 ), effort tolerance (6 min walking test; 6MWT 30 ). The psychometric properties of the 6MWT have been evaluated in HD. It is considered a core assessment for measuring aerobic fitness and endurance, 31 and it can be used to assess effort tolerance. 32 The outcome measures of the functional assessments included UHDRS functional capacity (Total Functional Capacity), functional assessment (FA) scale and dependence (Independence scale). 33 Patients were weighed each week, and energy requirements were assessed by a dietician. The outcome measures of cognitive function were selective attention (STROOP word, color and interference; 34 ), mental flexibility and visual scanning (Trail Making Test 35 ). The psychological outcomes assessed were depression and anxiety (Hospital Anxiety Depression Scale 36 ). The short form of the Problem Behavior Assessment (PBA-s) was designed for the assessment of neuropsychiatric symptoms in HD patients. 37 The Zarit burden scale assesses the psychological burden of the caregiver. 38
To evaluate whether the two groups differed in their physical activity levels during rehabilitation, participants wore a Geonaute pedometer (Decathlon, France) 39 for an entire week of the program. The pedometer was worn on the hip from waking up until evening. Each evening of the week at bedtime, a nurse recorded the number of steps displayed on the pedometer. Depending on their inclusion date, this monitoring week took place either at the beginning or at the end of the rehabilitation period.
Motor and functional outcomes for patients in the control and intervention groups were assessed at baseline and 4 weeks, except for the functional score and Zarit score at 8 weeks (one month after the end of the program). At 8 weeks, a semi-structured interview of caregivers from the intervention group was carried out by phone to explore the maintenance of physical activity after patients returned home, as well as the burden on the caregivers.
Statistical analysis
Before conducting the ANOVA, the assumptions of normality, homogeneity of variances, and sphericity were checked and met. A 2 (Condition: Intervention vs. Control) x 2 (Time: Pre-test, Post-test) mixed-design ANOVA was performed. Post-hoc tests with Bonferroni correction were conducted to follow up on significant interactions. The effect size was measured by calculating η2G for the ANOVA.
40
If the assumptions of normality, homogeneity of variances, and sphericity were not checked and met, non-parametric tests were performed. Non-parametric Mann–Whitney U tests (two-tailed) were performed to assess the difference in medians between intervention and control groups. Non-parametric Wilcoxon signed-rank tests were used to assess the difference in medians between pre and post for the same group. The effect size was measured as follows:
Results
Recruitment and retention
From May 2021 to October 2021, 41 patients were screened. The inclusion criteria were met by 32 patients, all of whom were able to follow up with the complete intervention with all activities and assessments within 4 weeks (Figure 1). The recruited patients lived in 11 different regions of France. For the inclusion of caregivers, not all patients had a caregiver (Table 1). Some assessments could not be completed due to missing reports from healthcare professionals. These omissions may be attributed to clinical constraints (e.g., workload, evaluator availability) or technical difficulties during data collection. Missing data for part B of the Trail Making Test indicated that patients failed to complete the requested task. Three caregivers did not complete the second assessment at week 8 and the post-intervention interview, because they did not consent or respond. The dropout rate of caregivers was one for the intervention group and two for the control group at week 8. Given the proportion and distribution of missing data, we opted for a complete case analysis.
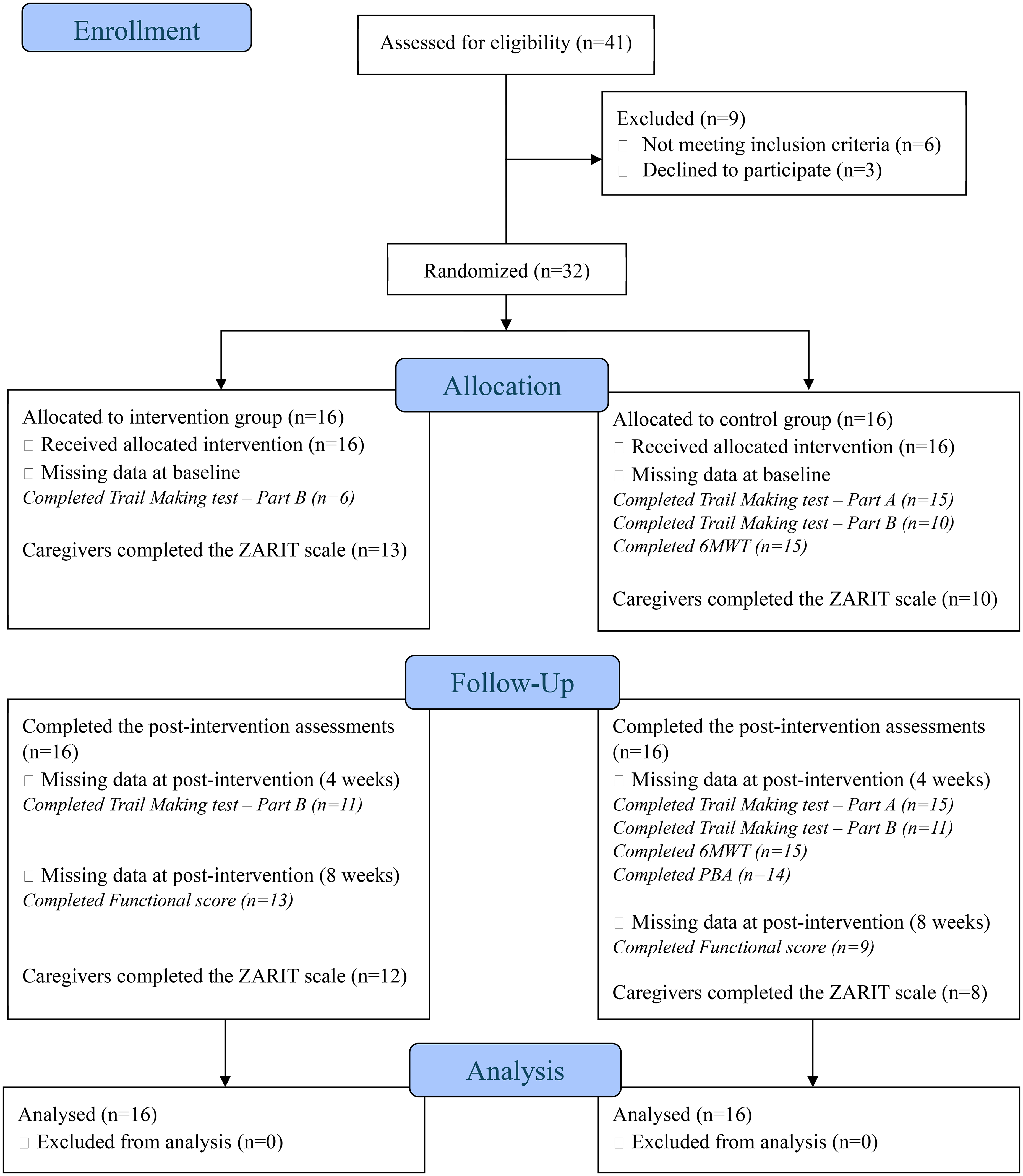
CONSORT flowchart of the study.
Baseline characteristics for all participants.
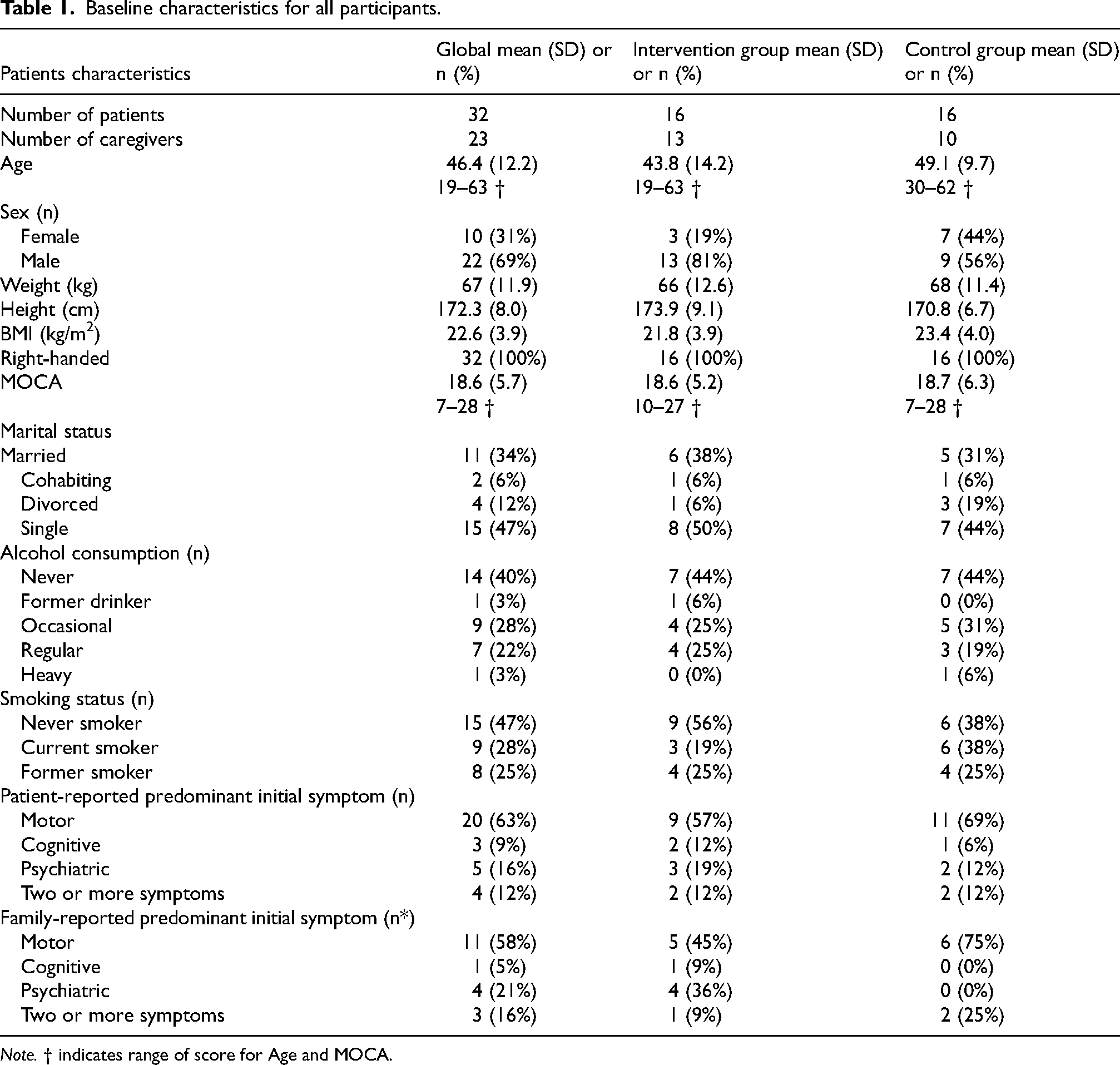
Note. † indicates range of score for Age and MOCA.
Descriptive and demographic data
All participants completed the study. Table 1 presents the characteristics of all the enrolled participants. Patients for the intervention group (M: 18.6; SD = 5.2) and the control group (M: 18.7; SD = 6.3) had mild to moderate neurocognitive impairment, as assessed by MOCA.
Intervention fidelity
A linear regression analysis was conducted to examine the difference in the number of steps between groups while adjusting for the chorea subscale scores. The overall model was significant, F(2, 24) = 14.22, p < .001, and explained 50% of the variance in number of steps (adjusted R2 = .50). Participants in the intervention group walked on average 68 218 (SD: 22 180) steps over a week measured during the stay, significantly more than the 37 861 (SD: 22 228) steps recorded in the control group. This finding indicated that the participants in the intervention group were more active than those in the control group during the implementation of our study, and that patients adhered to the exercise program proposed in the intervention group. In addition, higher chorea subscale scores are associated with more steps identified by the pedometer; each additional point was related to an increase of 1683 steps (β = 1,683, SE = 511, p = .003). Choreiform movements may have affected the step count measure, but UHDRS TMS scores were not significantly different between the groups (p = 0.88).
Every day, a clinical study technician was on site to supervise compliance with the protocol and activities. All participants included in the study completed the four-week inpatient rehabilitation program as outlined in the protocol. Attendance at the scheduled sessions was very high. Specifically, 15 participants attended all 20 exercise sessions, and one participant attended 16 out of 20 sessions, corresponding to an overall mean attendance rate of 98%. The few missed sessions were due to minor and isolated health issues related to stomach pain and did not disrupt the program or the rehabilitation process. Thus, attendance at the exercise intervention and at the other components of the multidisciplinary program was overall excellent.
Safety
There were no patients who dropped out during the intervention, and no serious adverse events were reported. The professionals in charge of the intervention reported to the study coordinator only a few minor adverse events, such as mild muscle soreness or mild fatigue, without moderate or severe adverse events.
Clinical outcomes
There was no significant difference between the groups on the primary outcome UHDRS-mMS at post-intervention (pvalue > 0.10). Figure 2 shows the evolution of the UHDRS-mMS for both groups, with higher scores indicating higher levels of motor impairment. Table 2 provides the means (95% CI) for the UHDRS-mMS, UHDRS-TMS and the 6-min walk test, with ANOVA results. In addition, between-group mean differences with 95% confidence intervals and corresponding effect sizes are presented, providing a clearer view of the magnitude and precision of the observed effects. This approach is consistent with recent recommendations for presenting inferential results and facilitates interpretation of practical significance beyond p-values. 42
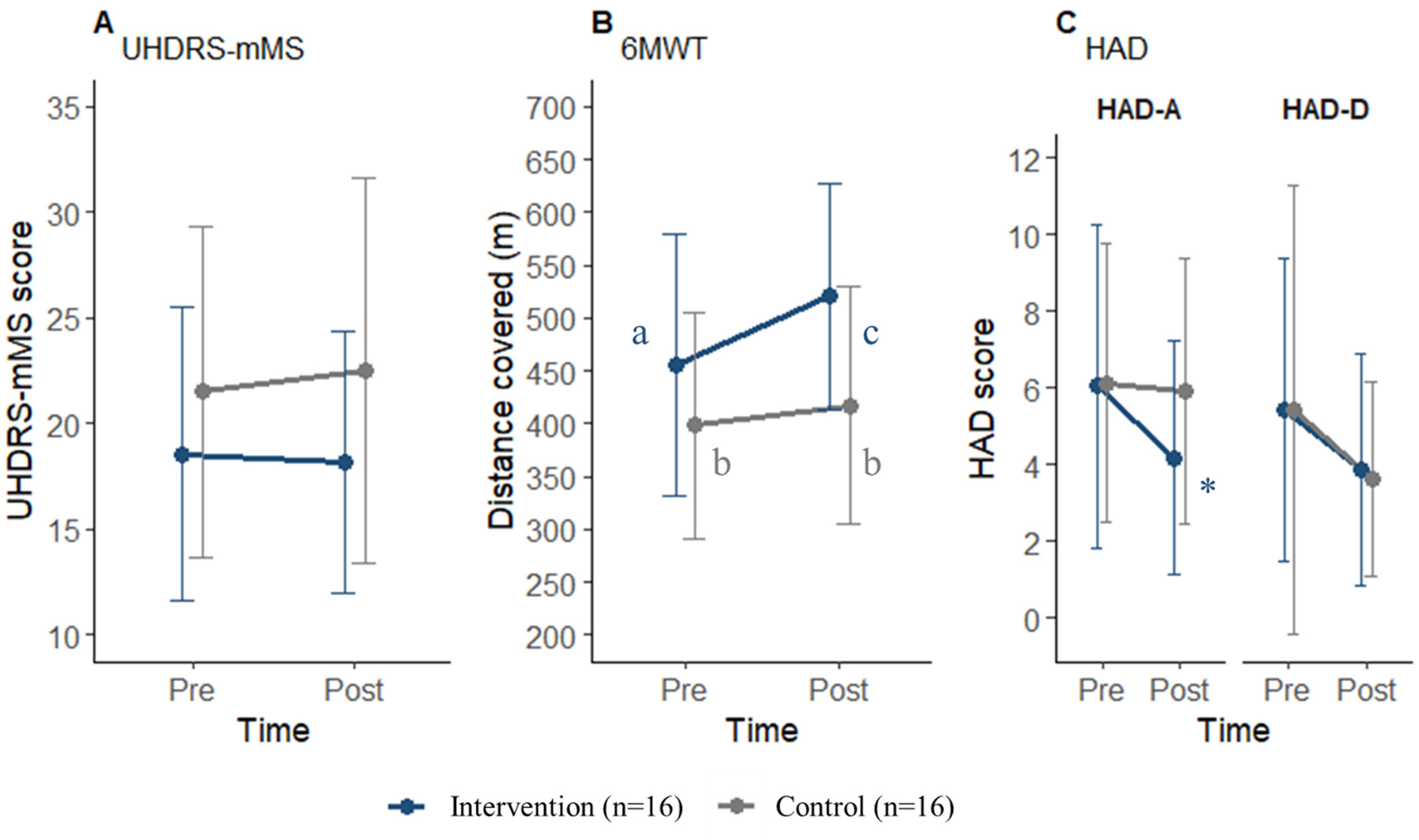
Overview of clinical outcomes. A: UHDRS-mMS score, B: Six-minute walk distance (6MWT), C: Hospital Anxiety and Depression Scale. Dots indicate mean values; error bars represent mean ± SD. To specify the results in Figure B and C, the same superscript letters indicate no differences, while different letters or * indicate significant differences at p = .05. For the 6MWT, the sample size was n = 15 for the control group.
UHDRS-TMS, UHDRS-mMS and 6-min walk test for control and intervention groups at baseline and 4-weeks.
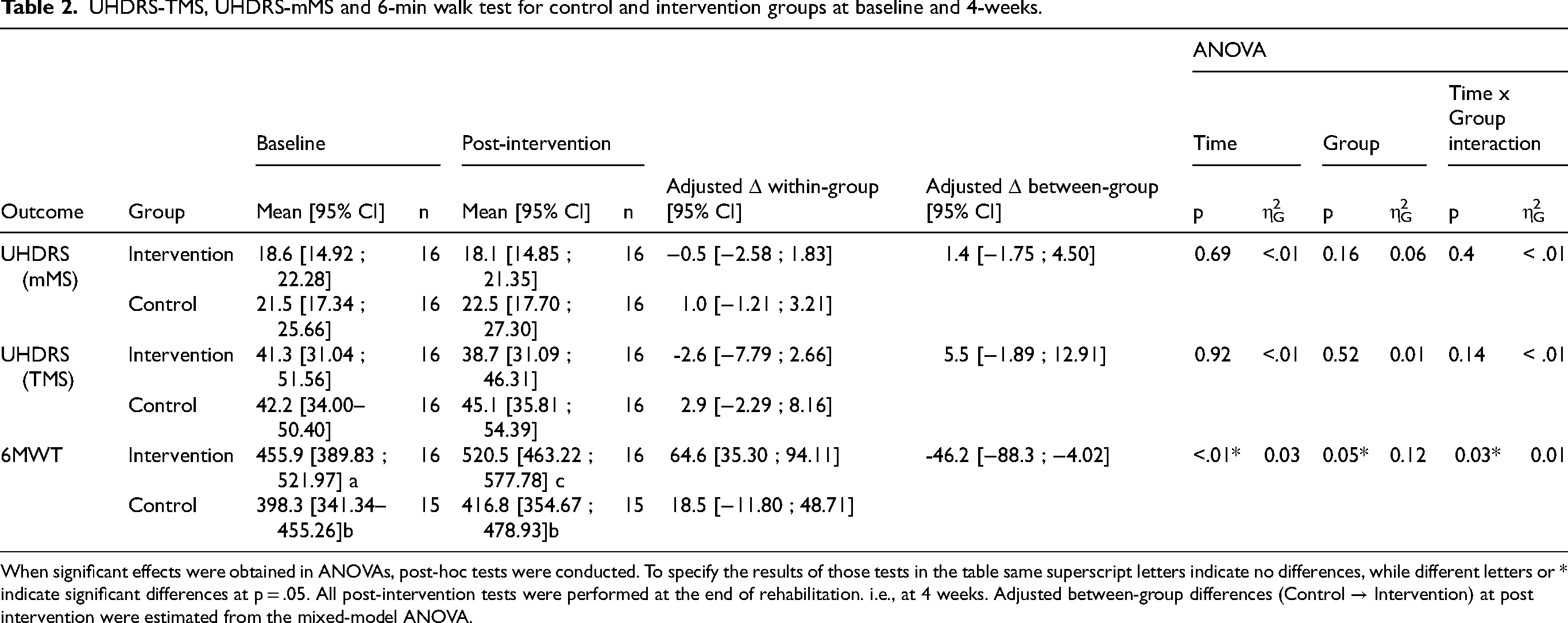
When significant effects were obtained in ANOVAs, post-hoc tests were conducted. To specify the results of those tests in the table same superscript letters indicate no differences, while different letters or * indicate significant differences at p = .05. All post-intervention tests were performed at the end of rehabilitation. i.e., at 4 weeks. Adjusted between-group differences (Control → Intervention) at post intervention were estimated from the mixed-model ANOVA.
For the secondary results, the intervention group covered more distance than the control group during the 6-min walk test at week 4, with a significant interaction Group*Time (F (2,29) = 5.02, p = 0.03). Within-group, the mean distance increased by 64.6 (SD = 57.9) meters in the intervention group, and by 18.5 (SD = 56.7) meters in the control group.
Table 3 provides the means (95% CI) for the motor and functional outcomes at baseline and at week 4, except for the Functional Score at week 8. A significant difference (p = 0.05) in the Berg Balance Scale was detected between the two groups at post-intervention, with a higher score in the intervention group (53.8) than in the control group (46.8).
Motor and functional outcomes for control and intervention groups at baseline and 4-weeks. except Functional score at 8-weeks.
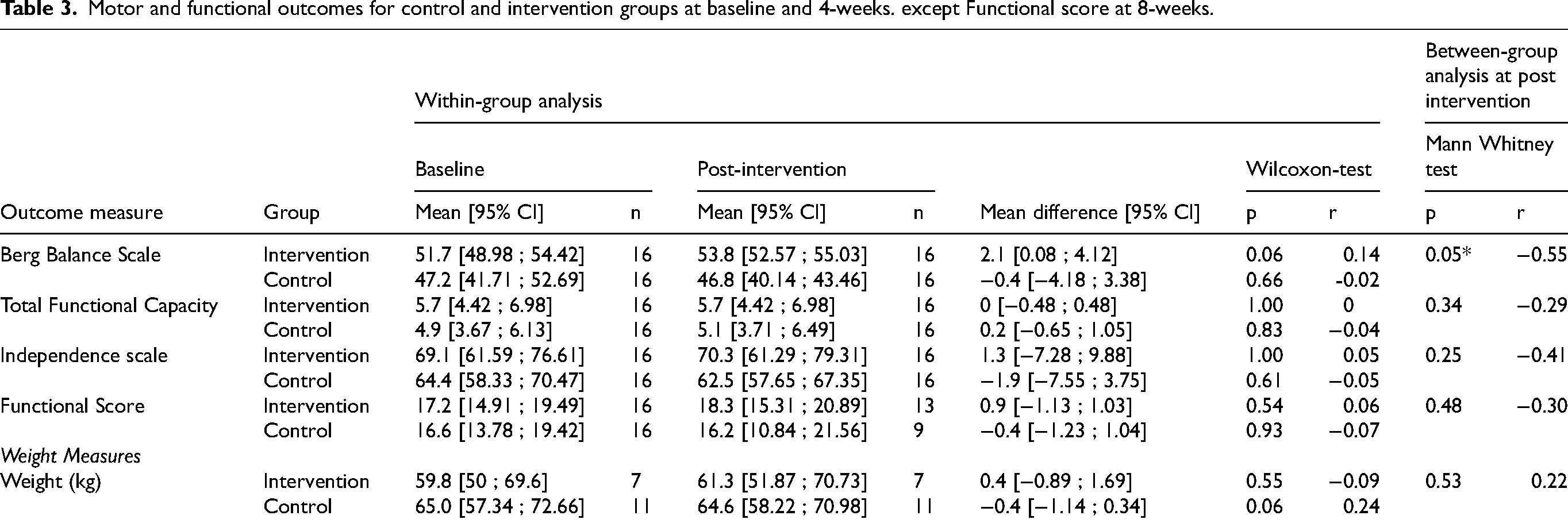
Table 4 provides the means (95% CI) for the cognitive outcomes at baseline and at week 4. Not all patients were able to complete the cognitive assessments, particularly part B of the Trail Making Test at baseline. In addition to those in baseline, 5 more patients were able to complete part B in the intervention group at week 4. In the reading part of the Stroop test, the intervention group read more words than the control group (p = 0.03) at week 4, with a significant increase only in the intervention group (+6.6, p = 0.04), but without a significant change in the interference score.
Cognitive outcomes for control and intervention groups at baseline and 4-weeks.
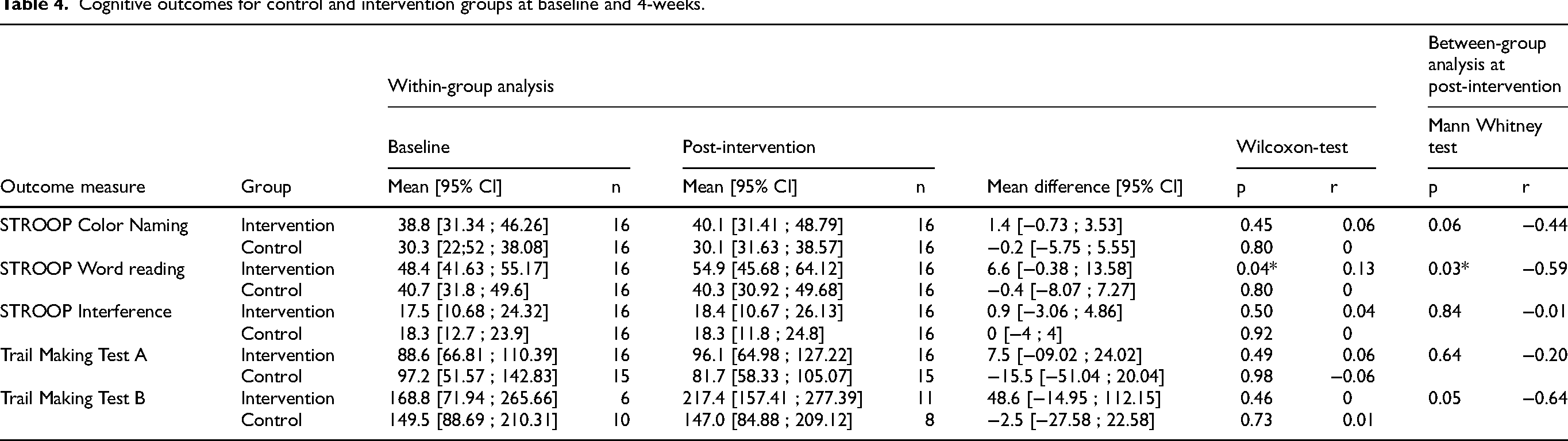
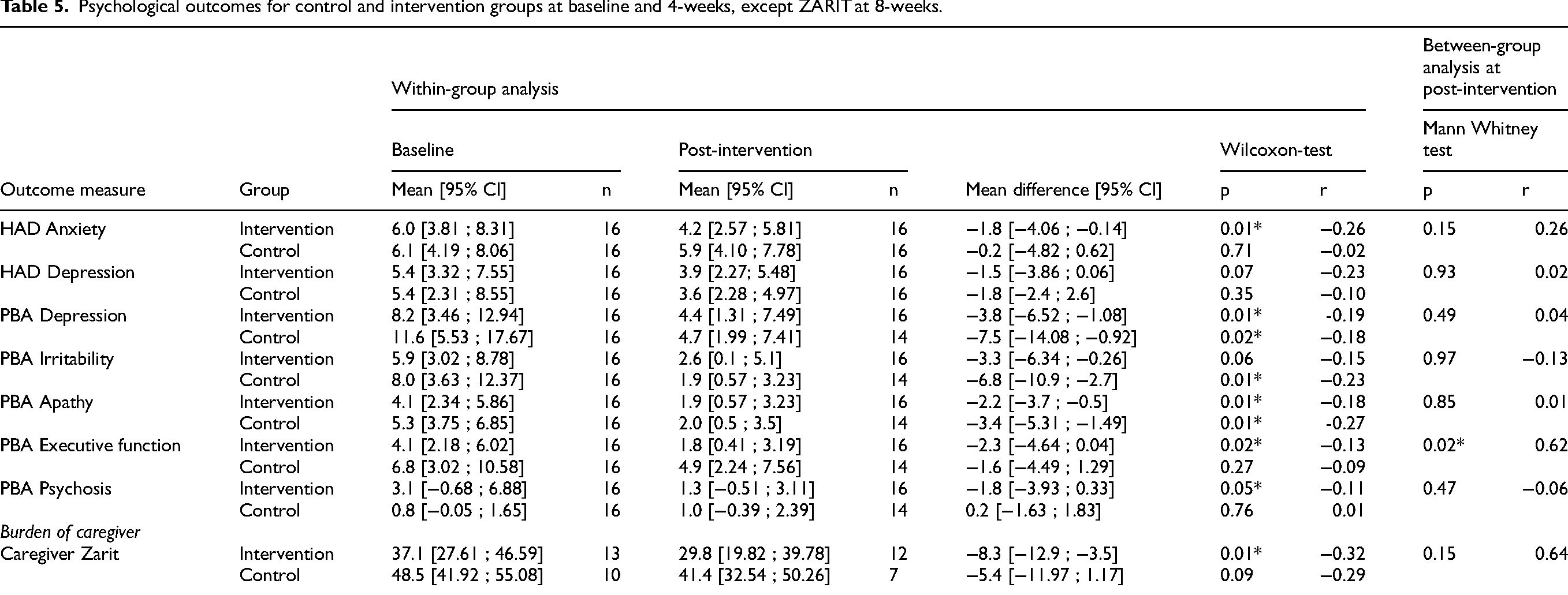
Table 5 provides the means (95% CI) for the psychological outcomes at baseline and at week 4, except for the Zarit score for caregivers measured at week 8. An improvement in the executive function score of PBA was observed at week 4 in the intervention group (p = 0.02), as well as a difference between groups, with the lowest score in the intervention group (p = 0.02). The scores of PBA depression and apathy tended to improve in the intervention group (p = 0.01) and control group (depression, p = 0.02, apathy, p = 0.01), which did not significantly differ between the groups at week 4. The score of PBA psychosis tended to improve for the intervention group only (p = 0.05), but there was no difference between the groups at week 4. The score of PBA irritability tended to improve for the control group only (p = 0.01) but was not different among groups at week 4. The participants in the intervention group had an improvement in anxiety (p = 0.01), as observed by a decreased score in the HAD.
Psychological outcomes for control and intervention groups at baseline and 4-weeks, except ZARIT at 8-weeks.
During the semi-structured interviews with the caregivers at week 8, 9 out of 10 stated that the HD patients continued to be physically more active when returning home than before rehabilitation, mainly by walking, cycling, and fitness exercises.
Discussion
This randomized single-blind controlled trial aimed to examine whether exercise provides additional benefits beyond those achieved through the rehabilitation approaches currently used in the control group by comparing an intensive multidisciplinary program with and without a structured exercise component in an inpatient setting. Both groups followed an inpatient rehabilitation program for four weeks, and only the intervention group participated in an exercise program of five sessions a week.
Intervention fidelity was high, likely due to the excellent attendance of the patients in the intervention, as found in the inpatient settings. 18 The intervention was also conducted in a safe and controlled environment, consistent with what is observed in the inpatient settings, 43 no serious adverse events were reported. The number of steps measured in the intervention group was higher than in the control group. This finding indicated that the participants in the intervention group were more active than those in the control group during the implementation of our study. Nevertheless, higher chorea subscale scores were associated with more steps identified by the pedometer in our analysis. Indeed, some sensors can overestimate steps, which further supports that chorea movements do impact count unless carefully handled. 44 However, wearable devices can provide continuous data reflecting actual performance, which is very useful to inform therapeutic development and behaviors in HD.45,46
The primary outcome did not reach significance, but the evolution of the UHDRS-mMS apparently tended to be opposite in the two groups. In the intervention group, the evolution of the descriptive data tended toward a minor improvement in motor function, as measured by the UHDRS-mMS (mean difference = −0.6 point), in contrast to the control group (mean difference = + 1 point). A longer-term evaluation could be useful to observe the dynamics of the UHDRS score over time. The UHDRS-TMS is sensitive to changes in motor symptom severity and tends to increase over time in persons with mid-stage HD.28,47,48 In the study by Frese and colleagues (2017), an increase of 7 in the motor UHDRS motor section was observed during 6 months of observation. 11 After this period of observation, the UHDRS total motor score stabilized during the 6-month exercise intervention, including 10 weeks of moderate-intensity continuous training at 65% VO2peak, followed by 8 weeks of high-intensity interval training at 90–95% peak heart rate and concluding with 8 weeks of moderate-intensity endurance training. 11
Maintenance of motor function often represents a primary clinical outcome, as motor function is characterized by a marked progressive decline. 23 In the intervention group, the exercise tolerance of the patients improved, as assessed by the 6MWT. However, the mean improvement of 64.6 (SD = 57.9) meters for this group is below the minimal clinically important difference of 126.14 evaluated for persons with mid-stage HD and 70.65 for late-stage HD. 49 This is consistent with the scientific literature, given that the intervention group regularly undertook supervised walking on flat ground and sand. This activity improves exercise tolerance and the spatial-temporal characteristics of walking. 16 In addition, in Fritz et al.'s 2017 meta-analysis, several studies reported benefits of physical activity assessed by the 6MWT. 8 However, the parameters of intervention appear to be important. Cruickshank and colleagues (2018) proposed an outpatient multidisciplinary therapy intervention with less intensive physical activity, and they did not observe significant results on the 6MWT. 50 Concerning static and dynamic balance, the significant improvement in the Berg Balance Scale observed in the intervention group was below the minimal clinically important difference of 5. 49 Although the intervention group scored higher than the control group on Berg Balance Score at post-intervention, a ceiling effect may be present with scores being close to the maximum score of 56.
Concerning functional capacity as assessed by the UHDRS Total Functional Capacity and Independence Scale, no significant results were observed. In line with these results, the study of Frese and collaborators revealed no significant alterations in functional ability. 11 The duration of the rehabilitation stay may be too short to achieve changes in functional capabilities, which neither regressed nor improved. Assessed by the Total Functional Capacity and Independence Scale, functional changes were more common in stage 3,1,25 which corresponds to a more advanced stage than that observed in the patients included in our study. Dietary management was implemented to control the participants’ diet and prevent weight loss resulting from the energy expenditure produced by physical activity. Despite an increase in their level of physical activity, patients in the intervention group maintained a stable weight. It was therefore important to monitor their nutrition, increasing their daily intake as needed. 51
Regarding the cognitive outcomes, the short duration of this study could be an important moderator, especially as some participants did not complete all the cognitive assessments. Nevertheless, the results are rather like those of longer multidisciplinary studies. Indeed, Cruickshank et al. did not observe benefits for these variables (STROOP and TMT) after 9 months of multidisciplinary rehabilitation, but showed a positive evolution of gray matter and cognitive functions related to verbal learning and memory. 52 The observed enhancement in the reading component of the Stroop test for the intervention group may be due to enhanced attention and the stimulating environment provided by the exercise program. While exercise appears to improve cognition in other neurodegenerative diseases, the results are less consistent in persons with HD. 53 Therefore, further investigation is needed into the interactions between cognition and physical activity in persons with HD.
In terms of psychological variables, participants in the intervention group showed significant improvements in anxiety and depression, as indicated by their HAD and PBA scores. These results complement those reported in the literature, although the effects on depression and anxiety remain unclear.8,10,15 Piira et al. demonstrated that a multidisciplinary program including physical activities led to an improvement in HADS scores in persons with HD. 20 The depression scores of PBA also showed signs of improvement in the control group. Indeed, a multidisciplinary intervention of 18 months without physical activity also appears to be effective in reducing anxiety and depression symptoms in persons with HD. 6 The observed enhancement in executive function in PBA for the intervention group aligns with prior research 54 and may result from the stimulating and structured environment provided by the exercise program. In addition, a reduction in psychotic symptoms was also observed in the PBA for the intervention group. Previous studies suggest that exercise, notably in high-intensity, can have beneficial effects on symptoms of psychosis, 55 but the mechanisms underlying these improvements are not yet fully understood. Both groups showed reduced apathy, as indicated by PBA. This is an important finding, given that apathy can affect adherence to and engagement in exercise routines.56,57 Irritability scores improved following the intervention for the control group only. Although research is limited, structured and calming activities have been suggested to help reduce irritability in patients with Huntington's disease. 57 These results are consistent with our intervention, as the control group benefited specifically from horse mediation and extended psychomotor therapy sessions focusing on emotions and relaxation. The Zarit score revealed a reduction in the burden experienced by caregivers in the intervention group. For the control group, the small number of caregivers included represents an important limitation. Caregivers play a major role in patients’ support and carry a heavy burden,58,59 reducing their work time and leisure activities. 60 The time needed to meet their own needs in daily life 61 and the fact that the patient is cared for, 3 may be two main reasons for this reduction in the perceived burden on the caregiver.
Beyond the immediate effects of an exercise program, the sustainability of an observed benefit can legitimately be challenged, 54 especially after an inpatient rehabilitation program. Individuals with neurodegenerative diseases often struggle to maintain adherence to exercise programs, particularly after receiving rehabilitation care. 62 Importantly, short exercise programs should continue to be adapted in the long term with a focus on retention and adherence. According to interviews with caregivers, patients continued to be physically active when returning home, mainly walking, cycling, and exercising. The social and familial context of persons with HD is a key consideration for health care professionals supporting physical activity.31,63 To promote active behaviors in the long term, tools and resources are necessary, such as the co-design of a care partner resource developed in the study by Jones and collaborators. 64 The inpatient rehabilitation program in our study could be a promising starting point for exploring non-supervised or distance-based interventions in post-intervention. These interventions would aim to measure behavioral changes and support long-term adherence to an active lifestyle. In this context, the presence of an HD care coordinator with a focus on person-centered integrated care could be a promising perspective after an inpatient rehabilitation program. 65
Limitations and strengths
One limitation of this study is the small sample size; the results should be interpreted with caution. Although the sample size corresponds to our calculations, the size of the confidence intervals suggests that the sample size is insufficient. The sample size calculation seems to have been ambitious, given the effect size of 1.1 indicated. It would be useful to conduct a study with a larger sample size to obtain more robust results. Some participants did not complete all the assessments, particularly the cognitive assessments. For future studies, we suggest involving all professionals who will participate in the research protocol from the outset to improve engagement and adherence. This should include the use of electronic reminders, periodic monitoring of data entry, and regular feedback to clinical teams on data completeness. A four-week intervention may be too short to measure significant effects for certain variables that are not very sensitive in the short term, particularly the UHDRS score, functional and cognitive assessments. Some results did not reach the required level of significance. This could be due to the intervention having an insufficient effect or the sample size being too small. Only participants with a stable medication regimen and no difficulties that would impair their ability to complete rehabilitation were included. The lack of availability of inpatient rehabilitation stays for persons with HD in countries outside Europe may affect the representativeness and generalizability of the findings for persons with mid-stage HD. The intervention group was compared with the control group, which also benefited, particularly the psychological variables observed in PBA categories. For moderate-intensity exercises, only observation and patient feedback with Borg CR-10 were used to verify intensity. No physiological assessments or metrics (e.g., heart rate during exercise) of intensity were carried out and represent a major limitation. Another limitation of this study is that physical activity was measured using a basic pedometer rather than a more advanced or validated accelerometry device, which may reduce the precision of the activity estimates. Finally, the maintenance of physical activity was measured only one month after the patient returned home during the caregiver's interview. While these data are valuable, it would be interesting to observe the maintenance of physical activity and the long-term benefits obtained through later follow-ups with objective measurements.
The strengths of this study include an inpatient rehabilitation program with a short duration stay (4 weeks), an intensive rehabilitation schedule for the intervention group with five exercise sessions per week, an evidence-based intervention, strong adherence from participants, a controlled environment, and a control group. A description of the rehabilitation and exercise interventions (frequency, intensity, duration, and type) is available in supplementary files with a TIDieR framework. As both groups were hospitalized for the same period, the assessment environment was similar for all participants. Patients took part in all the activities (overall attendance rate of 98%) proposed in their group, which is a strength compared with other studies in which patient adherence fluctuates. However, we did not record compliance with the prescribed sets, repetitions, or exercise intensity, which would have provided additional information on how participants tolerated and engaged with the intervention. The patients’ motor functions were blindly evaluated before and after the intervention by 3 externally experienced HD neurologists.
Conclusion
This study provides evidence supporting adherence to and the positive effects of an exercise program based on aerobic exercise and resistance training at moderate intensity in persons with mid-stage HD during four weeks of inpatient rehabilitation. This inpatient rehabilitation program had positive effects on psychological symptoms in both groups, while the exercise program produced additional positive effects beyond exercise tolerance, anxiety, STROOP Word Reading and executive function. The control group, which received a specific program without physical activity and focused more on relaxation, showed improvements specifically related to irritability. The short duration of this inpatient rehabilitation program may require longer-term post-rehabilitation support to develop and maintain the benefits obtained.
Supplemental Material
sj-docx-1-hun-10.1177_18796397261422975 - Supplemental material for A moderate-intensity exercise program during inpatient rehabilitation for middle stage Huntington's disease: A randomized controlled trial
Supplemental material, sj-docx-1-hun-10.1177_18796397261422975 for A moderate-intensity exercise program during inpatient rehabilitation for middle stage Huntington's disease: A randomized controlled trial by Mathis Brusseau, Brigitte Soudrie, Anne-Catherine Bachoud-Lévi, Stéphanie Bannier, Frédéric Bourdain, Marine Jenkins, Pierre-André Natella, Nolwenn Bombenger and Julie Boiché in Journal of Huntington's Disease
Footnotes
Acknowledgements
The authors thank the participants of this research and their caregivers who generously gave their time. The authors would like to thank all the professional teams for their willingness and enthusiasm to take part in this research project. The authors wish to note that Dr Jenkins has changed affiliation since the completion of this study. We gratefully acknowledge Dr Ben Salah for their insightful assistance during the revision of this manuscript and for their ongoing commitment to the follow-up projects arising from this work.
The committee for the protection of individuals East III approved this study (N°ID-RCB: 2021-A00423-38). Written informed consent was obtained from patients and their caregivers by the study coordinator.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The sponsor was the Assistance Publique – Hôpitaux de Paris (Direction de la Recherche Clinique et de l'Innovation).
Assistance Publique - Hôpitaux de Paris,
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting this study are not publicly available. Further information can be obtained from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.