
Abstract
Acceptance and commitment therapy (ACT) is an experiential, action-oriented talk therapy that emphasizes acceptance of painful inner experience through increased psychological flexibility. In this narrative review and case report, we first review the extant literature on applications of ACT to patients with a variety of mental and physical health challenges, including neurodegenerative disorders, and their caregivers. We then discuss applications of ACT to Huntington's disease (HD). We provide a case report of a 52-year-old man living with HD who, accompanied by his caregiver, received a virtually-delivered 6-session ACT intervention. We measured the patient's self-reported symptoms of depression (PHQ-9) and anxiety (GAD-7) as well as his health-related quality of life (HDQoL) and level of cognitive fusion (i.e., being attached to his thoughts; CFQ-13) at baseline and following the intervention. At follow-up, the patient had a clinically significant reduction in depressive symptoms (from moderate to mild symptomatology) and cognitive fusion. Further, the patient had improvements in quality of life across the domains of physical functioning, mood, and worries. The promising outcomes of this case, as well as extant literature on the effectiveness of ACT in supporting individuals with similar neurodegenerative disorders, suggests that ACT may hold promise as a scalable and impactful intervention for individuals living with HD and their caregivers. We conclude with a call for further study of ACT with this population to build a more robust evidence base that can be used to benefit individuals living with HD and their caregivers.
Keywords
Introduction to acceptance and commitment therapy
Acceptance and commitment therapy (“ACT” pronounced like “active”) is an experiential, action-oriented talk therapy that emphasizes cultivation of psychological flexibility via six interacting processes.1,2 ACT is considered a “third wave” cognitive behavioral intervention; it evolved from cognitive behavioral therapy (CBT), though there are many core differences between the interventions. While CBT is typically focused on “fixing” problems by changing ways of thinking (e.g., evaluating the accuracy of one's thoughts) and behaving (e.g., engaging in an activity even in the face of anxiety), ACT emphasizes changing one's relationship to painful thoughts, feelings, and struggles, in pursuit of a meaningful life even in the face of contextual challenges.
The six central processes of ACT include getting in touch with one's values (i.e., what one stands for in life; how one wants to live), acceptance of painful inner experience (e.g., of uncertainty about the future), and finding motivation to take committed action steps in the service of one's values, rather than engaging in efforts to avoid painful inner experiences. Additionally, there is an emphasis within ACT on developing contact with the present moment (i.e., building mindfulness skills), rather than getting caught in past regrets or future worries. ACT also focuses on methods to help detach or “defuse” from unhelpful thought content (e.g., having the thought, “it's not worth trying to find meaning, I’m only going to get worse.”) Changing one's relationship with painful thoughts can then free them from engaging in avoidance behaviors (e.g., substance use, skipping medical appointments) that served to escape such thoughts. The final component of ACT is accessing an ever-present self that has persisted through all of one's experiences (see Table 1 for further explanation of these six core processes).
Core ACT processes and their applications to Huntington's disease.
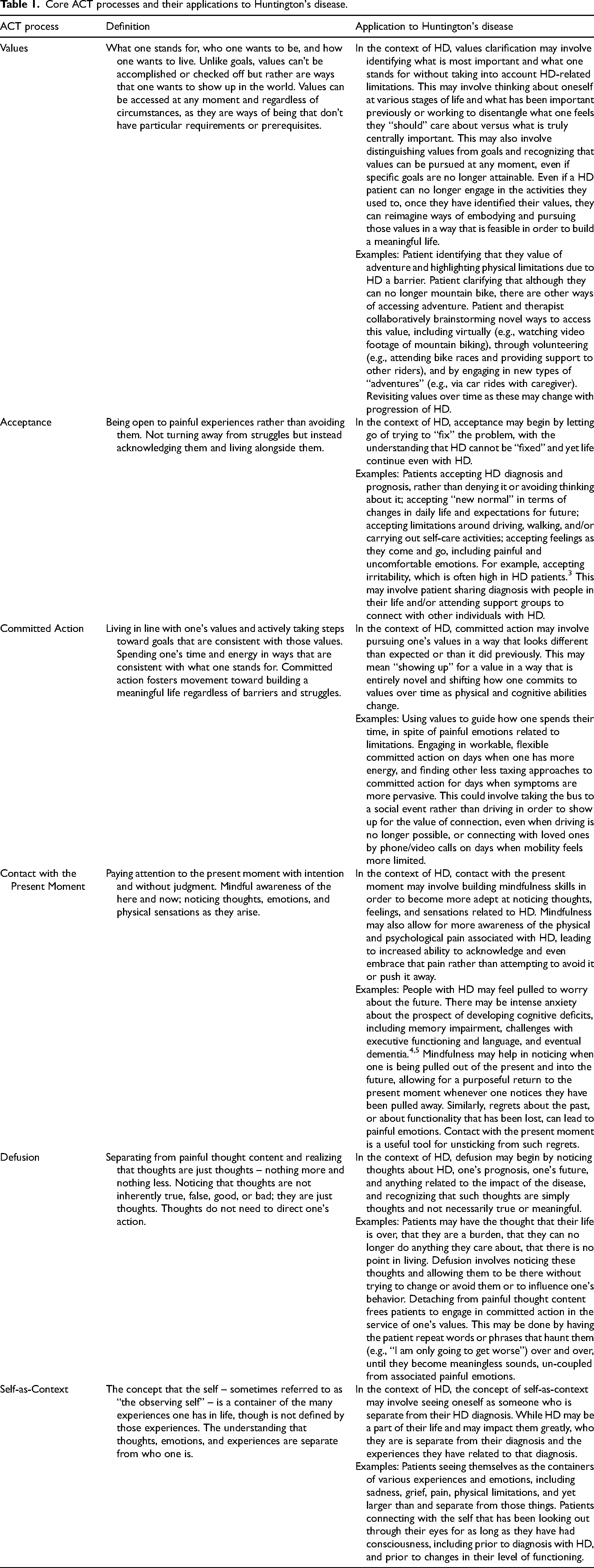
Given these core components, ACT is particularly well suited for helping patients forge their best lives while dealing with challenging experiences that cannot be changed. Further, ACT is a transdiagnostic intervention, meaning that it is not condition-specific and can be used to address a broad range of challenges. ACT is also highly flexible and can be delivered in a variety of modalities (e.g., in person, virtual), durations (e.g., short manualized protocol, longer-term principle-driven talk therapy), formats (e.g., individual vs. group), and settings (e.g., mental health clinic, hospital).6–8 The six core processes – values, acceptance, committed action, contact with the present moment, defusion, and self-as-context are typically flexibly interwoven throughout therapy using exercises and metaphors that can be tailored to the individual patient and their struggles.
ACT has been tested extensively in research trials as an intervention for both mental and physical health challenges.9–11 It is an empirically supported treatment for many mental health conditions including depression and anxiety disorders 8 and substance use disorders 12 and has been used to treat suicidality.13,14 ACT has also been used to treat chronic pain15–17 and a variety of chronic health conditions6,7,11,18,19 and noncommunicable diseases.20–22 Further, ACT has been used to treat psychological distress associated with a broad set of neurological disorders 23 and neurodegenerative disorders, including multiple sclerosis,24,25 Parkinson's disease,26,27 and motor neuron disease.28,29 It has also been used to support caregivers of patients with neurodegenerative disorders and other chronic health conditions.30–32 While the literature supporting the effectiveness of ACT is more robust for certain conditions than others (e.g., depression, anxiety, and chronic pain have been particularly well studied), there is clear evidence that ACT can be effective for an array of physical and mental disorders.8,10,11
Acceptance and commitment therapy and Huntington's disease
Mental health and Huntington's disease
Given its effectiveness with other neurodegenerative disorders, ACT holds promise as an intervention for patients with Huntington's disease (HD) and their caregivers. HD patients suffer from numerous compounding physical and mental symptoms, creating an intense psychological burden that is often overlooked due to the many comorbid medical challenges. This psychological burden can further deplete quality of life.33–35 In addition to the host of physical symptoms, cognitive decline, and behavioral and emotion regulation difficulties, psychological difficulties in HD include depressed mood, anxiety, irritability, and apathy.36–38 Further, patients with HD often develop other comorbid psychological challenges, such as obsessive compulsive disorder (OCD), bipolar I disorder, depression, and anxiety.39–42 Psychological distress is not only common among HD patients, but also often develops prior to a diagnosis of HD.43–46 For many of these comorbid conditions, prevalence among HD patients is higher than the general population.39,46 Further, suicide risk within this population is high; suicide is the third leading cause of death amongst HD patients with estimates of two to seven times risk compared to the general population.47–49 Mental health difficulties significantly impact quality of life for individuals with HD, as well as their caregivers. 50 Caregivers of individuals with HD often experience anxiety, depression, and burnout.51–55
Studies have found that psychological distress is among the most prominent issues faced by HD patients and caregivers. 56 Further, HD patients and caregivers have identified a pressing need for mental health support. For example, in previous studies, HD patients and caregivers expressed interest in receiving psychological support, listing mental health care as a priority need.57,58 Despite this clear need, patients and caregivers have expressed understandable difficulty in knowing what services to seek out or ask for, as accessible and HD-specific mental health services are nearly unheard of, and to date there has not been a gold standard psychological treatment established. 59
Psychotherapeutic interventions for patients with Huntington's disease
There is a paucity of research on psychological interventions for individuals living with HD,60,61 a deficit that has been noted in the literature.61,62 Indeed, psychological support has been highlighted by experts in the field as a necessary aspect of care for HD patients and an area that is urgently needed and vastly underdeveloped.63,64 It has also been recommended that psychotherapy be considered for managing psychological challenges prior to psychopharmacological considerations. 65 Despite the numerous psychological challenges associated with HD, including the need to face inevitable shortened life expectancy as a result of the disease, the field has tended to take a more neuropsychiatric approach to addressing mental health-related symptoms rather than a psychological approach. This has been highlighted as a limitation to supporting patients with HD as it creates a paradigm that underemphasizes psychological components within research and throughout the broader HD community (i.e., including patients, doctors, and caregivers). 63 Given the limitations of a neuropsychiatric paradigm, there has been a call for a shift towards a more psychologically-based framework by researchers in the field and by HD patients, who have noted desire for more psychological support.57,63 Recently, more psychologically-based models have been proposed. 56
Despite the need for psychological support, the research on this topic is sparse. We found a single systematic review from 2020 on psychological interventions for individuals with HD, which identified nine studies. 61 Evidence across these studies was found to be limited and preliminary, with only a single randomized trial and only a small range of psychological outcomes being examined.
Cognitive behavioral therapy and Huntington's disease
Of the extant publications on psychological treatment of HD patients, there have been three studies focused on the use of CBT with HD patients.66–68 Of these, two case studies documented the successful use of CBT in addressing specific mental health difficulties. In one study, CBT was found to reduce depression and anxiety in a patient with presymptomatic HD. 66 In another, CBT was adapted to account for a patient's cognitive limitations and was found to reduce symptoms of OCD and post-traumatic stress disorder. 67 While in both cases, CBT was found to be successful in treating these specific symptoms, the intervention did not address HD-related distress more broadly. A pilot study involving a larger sample of HD patients (both symptomatic and presymptomatic) tested an intervention that incorporated CBT techniques and had mixed results; following the intervention, symptomatic participants had reductions in anxiety, however standardized depression scores did not change, and dropout was high. 68
Although CBT has a robust evidence base for treating a wide array of psychological difficulties that are common in HD (e.g., anxiety and depression) it may fall short in optimally addressing the needs of this population. A recently published review on treatment of depression in HD noted the limitations of CBT, proposing that many CBT interventions focus on assessing cognitions and can thus be cognitively demanding, and not a good fit for individuals experiencing cognitive decline or diminished executive function. 69 Further, CBT involves examining the link between thoughts, emotions, and behaviors, and often includes techniques, such as cognitive restructuring, where thoughts are evaluated for their accuracy. In the context of HD, negative or extreme thoughts about the disease or one's prognosis may in fact be rational and accurate, which may undermine the helpfulness of CBT. 70 For example, given the life-limiting nature of HD, traditional CBT strategies, such as finding evidence for and against distressing thoughts like, “I’m going to die soon,” inevitably fall short. Additionally, there is often an embedded assumption within CBT that the “problem” can be resolved if individuals re-examine their thinking or change their behaviors, which may not be applicable in the case of HD.
Third-wave cognitive behavioral therapies and Huntington's disease
Two studies have examined third-wave CBT interventions that, like ACT, incorporate mindfulness.71,72 In a small pilot feasibility study, presymptomatic HD patients participated in an 8-week mindfulness-based cognitive therapy group. 71 In this group of patients with low baseline levels of anxiety and depression, there were minimal changes in distress.71,73 In another pilot study involving a mindfulness-based stress reduction group intervention for pre-symptomatic HD patients, psychological distress was comparable pre- and post-intervention, though baseline distress was similarly low. 72 In both studies, participants expressed strongly positive experiences with the intervention, and researchers noted a need for larger, controlled studies involving more symptomatic patients.
Given the small number of studies, limited sample sizes, uncontrolled study designs, and low baseline symptomatology, the extant evidence in support of CBT and third wave approaches for HD patients and caregivers is limited. However, when considered together, previous literature suggests that HD patients found mindfulness-based approaches to be highly acceptable. Given that mindfulness-based approaches tend to address challenges holistically (rather than focusing on specific symptoms or diagnoses), such approaches may be better suited than CBT to address the nuanced and wide-ranging concerns within this population.
In addition to mindfulness, previous research points to the importance of acceptance in effectively coping with the challenges associated with HD. 74 Indeed, across the broader literature, acceptance-based therapies have been identified as a beneficial and recommended approach for patients with HD.56,62,70,75 Given that ACT incorporates both mindfulness and acceptance, among other core components, it may be a particularly well-suited intervention for this population.
Why acceptance and commitment therapy?
ACT holds promise as an intervention to support HD patients and their caregivers in reducing symptoms of depression and anxiety and improving psychological flexibility and overall quality of life. ACT is a particularly promising intervention for patients with HD, given both its effectiveness in treating other neurodegenerative disorders and chronic health conditions, and for the alignment of the “spirit” of the intervention with the context of what HD patients experience.56,60,62,63,76
In addition to the ways in which the six core processes may be specifically applied to HD patients (see Table 1) and caregivers (see Supplemental Table 1), there are general characteristics of ACT that align well with the multifaceted psychological and psychosocial needs of HD patients and caregivers. First, ACT is highly contextual, meaning that it takes into account aspects of an individual's circumstances. This may be inherently validating to patients, as it allows for a different way of relating to thoughts and emotions rather than trying to reframe painful thoughts related to one's diagnosis or to find evidence for why caring for a loved one with HD may not be as catastrophic as one's thoughts make it out to be. An ACT approach encourages making space for very appropriate grief and pain, allowing for processing of emotions (rather than trying to push them away) and encouraging one to engage in life even in the face of these difficult emotions. In other words, there is a focus on relating differently to pain rather than trying to feel differently or better about painful circumstances. Second, ACT is highly flexible, which suits the nuanced, compounding, and evolving needs within this population. Because it is a transdiagnostic intervention, there is no need to “pick” a particular symptom or disorder to focus on, which is congruent with the heterogeneity of HD-related challenges and the broad set of associated symptoms and comorbidities. This flexibility and adaptability of ACT is aligned with the needs of HD patients, who have noted the importance of flexibility and individualization within mental health care. 58
Despite manifold examples of why ACT may be a good fit to support HD patients and their caregivers, to our knowledge there have been no published trials or case studies examining applications of ACT to this population. Fortunately, two recently proposed studies will examine use of ACT with this population. A study protocol was recently published that will examine the impact of a self-guided intervention that incorporates ACT principles on HD gene expansion carriers. 77 Additionally, a study was recently registered to examine use of ACT in a group format to support HD caregivers. 78 Though sparse, these recent study proposals are promising as they will add to the limited literature on this topic and may generate additional questions for future research.
Case report
Background
We delivered a 6-session ACT intervention to a patient with HD who had been receiving routine outpatient psychotherapy within our clinic. Given the COVID-19 pandemic, all sessions with the patient (both prior to and including the 6-session ACT intervention) took place via telehealth; ACT sessions occurred from May to June of 2022. In writing up this deidentified case report, we consulted with the Jefferson IRB, who indicated that no formal IRB exemption was needed given that this intervention was delivered as a part of routine care. We also got consent from the patient and his caregiver, who expressed strong support of sharing these findings.
The patient, a 52-year-old White cisgender heterosexual man receiving outpatient care in a northeastern city, had previously been diagnosed with HD as well as comorbid bipolar I and severe OCD, both of which were associated with his HD and had worsened with the progression of the disease. The patient had presented to the clinic approximately nine months prior to the start of the ACT intervention and had been receiving weekly virtual therapy (though sessions were often cancelled due to conflicting medical appointments or other unanticipated conflicts). In the preceding nine months, treatment had been CBT-based and primarily focused on his OCD symptoms; progress had plateaued and thus another approach was warranted. The 6-session ACT intervention was delivered to the patient by the same provider in the context of this ongoing therapeutic relationship.
Given the patient's significant anxiety and OCD symptoms, he attended therapy sessions with his caregiver (his ex-wife, with whom he lived and had a close friendship). His caregiver's presence aided in reducing his anxiety (when the patient first presented to the clinic, he would only engage in therapy if his caregiver was present for the full session) and served to support him in engaging in the therapy (e.g., encouraging him to participate in therapy exercises; offering words of support; taking notes about assigned exercises in order to support him in completing them between sessions, etc.). Unlike in the prior nine months of therapy, wherein the caregiver was present for sessions but did not participate in therapeutic interventions (though was instrumental in facilitating his attendance, sharing her perspective about the patient's progress with the therapist, and serving as a common thread across the patient's multidisciplinary care team), in the 6 ACT sessions, she was invited to participate more actively (see below for greater details of each session).
Method
Following delivery of the intervention and its positive impact on the patient, we felt it would be beneficial to write up this case report, given the limited literature on psychological interventions to support individuals with HD. We sought consent from the patient and his caregiver; both provided consent enthusiastically and expressed full support for their case being written for publication. We also sought approval from the Thomas Jefferson University Institutional Review Board, which determined that this de-identified case report was exempt from the need for review.
Intervention
The brief ACT intervention was an adapted version of prior treatment manuals for specialized ACT interventions developed by our team and tested among patients with different chronic health conditions, including ACT with HIV, 79 ACT with Cystic Fibrosis, 80 and ACT with Pancreatic Cancer. 21 This prior intervention was adapted to address the specific challenges associated with HD (e.g., changing the number from 80 to 60 in an exercise where patients are asked to consider their 80th birthday party) and to engage the support and participation of the caregiver. A general description of the intervention follows, along with some examples of HD-specific modifications and applications. Table 2 provides further information about session content with an emphasis on concepts being introduced in each session. It is important to note that the mechanism of action of ACT is increasing psychological flexibility, which is revisited (along with values, barriers, acceptance, and committed action) in every session, resulting in a flexible and fluid intervention.
6-session ACT intervention components.
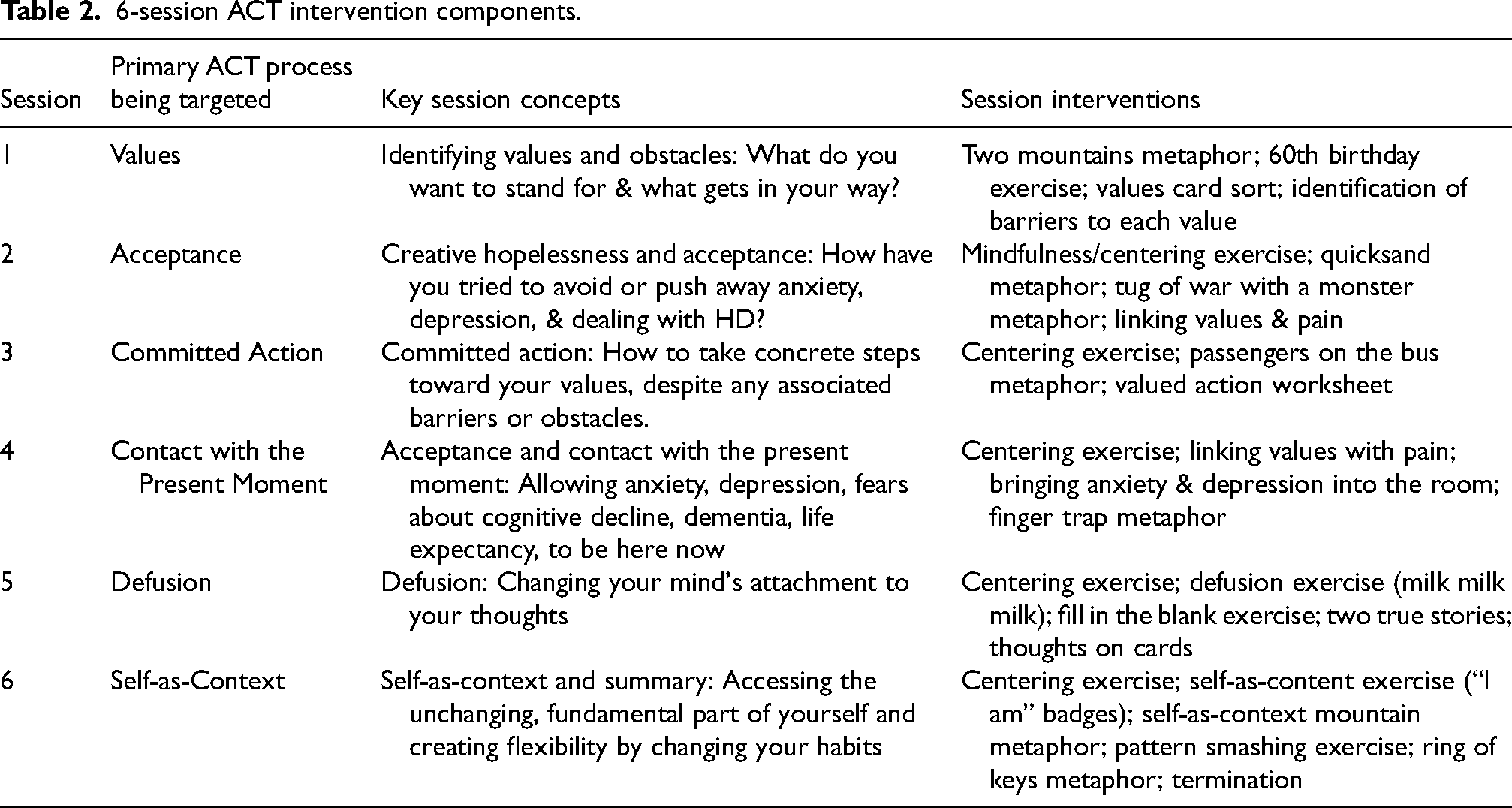
Session 1 starts with values clarification exercises and centers the patient's values (how they want to live, which is distinguished from goals), and informs committed action, which we challenge the patient to take throughout the intervention. In Session 1, the patient and caregiver were each asked to identify their top 5 values. Values are revisited each session, and each session has associated home practice (i.e., homework) regarding connecting with values, identifying barriers to those values, and taking small steps in the service of one's values. In Session 2, values are revisited to ensure that the patient's previously identified values remain relevant (new values are substituted as needed.) The patient is then engaged in a review of prior control strategies that they may have engaged in (including avoidant coping) and how acceptance frees us from the need for avoidant coping or other maladaptive strategies. In this case, introduction of the concept of acceptance included an emphasis on HD and the painful experiences that often come with the diagnosis. The primary target of Session 3 includes committed action (i.e., small steps that the patient and his caregiver could take in the direction of their individual values). When we are freed from the vice-grip of avoidant coping, we then have more bandwidth to engage in actions that align with our values. In this session, we also revisit values and the barriers that come up when we contact our values. We also introduce how increased barriers may even serve as a signal that we are moving toward our values, which hopefully is happening at this mid-point in treatment. This sets the scene for Session 4, which emphasizes the importance of contacting painful emotions that may be present, rather than engaging in avoidance strategies to reduce contact. Here, the link between values and pain is emphasized: as we approach our values, our mind creates barriers in the form of painful emotional and unhelpful thoughts. We introduce mindfulness skills as a tool that can be used to return to the present moment even in the face of those difficult thoughts and emotions. Session 5 provides direct tools for changing our relationship with these unhelpful thoughts and other barriers that our minds generate when we move toward our central values (e.g., “what is the point of investing in relationships if I am going to die soon?” or, “I no longer have time to take care of my own needs, so why bother trying?” Finally, Session 6 serves as a recap and consolidation of previous session concepts, along with introducing the final concept of self-as-context: that there is a consistent self that persists through all emotional and physical discomforts, challenges, and celebrations (e.g., I am not my HD; HD is a part of my experience in life, but I am separate from and bigger than that diagnosis). Similarly, we create psychological flexibility via changing habitual behaviors to create novel experiences.
Measures
To better understand the impact of the intervention on the patient's mental and physical functioning, we administered several validated self-report questionnaires immediately prior to and following intervention (i.e., at Session 1 and Session 6). These measures were delivered as part of the clinic's routine outcome monitoring protocol and selected based on their clinical relevance. Measure selection was guided by the clinic's standard practice of administering no more than 3–4 measures in an attempt to balance collection of important objective data through validated questionnaires with prioritizing patient rapport and minimizing response burden. Though this case report is limited by the measures that were administered, future empirical studies evaluating use of ACT with HD patients and caregivers should include additional questionnaires measuring relevant constructs (e.g., assessing values-based living).
Four self-report measures were chosen by the therapist (author SHS) to capture symptoms of depression and anxiety (PHQ-9 and GAD-7), cognitive fusion (CFQ-13) and health-related quality of life (HDQoL). The PHQ-9 and GAD-7 are standard measures used within the clinic to monitor symptoms of anxiety and depression and have been used regularly with patients with HD.81,82 The CFQ-13 has been used within our clinic in the context of ACT interventions to assess the extent to which cognitive fusion –rigid attachment to unhelpful thought content – had changed. Cognitive fusion, and its opposite, cognitive flexibility, are central components of broader psychological flexibility. The HDQoL – a HD-specific measure capturing health-related quality of life – was selected to assess functional improvement across important domains of the patient's life. The Patient Health Questionnaire (PHQ-9) is a 9-question multipurpose instrument for screening, diagnosing, monitoring, and measuring the severity of depression. 83 Scores range from 0 to 27, with higher scores indicating greater depressive symptoms. Psychometric properties include good reliability (Cronbach's α = 0.86–0.89); excellent test-retest reliability. The General Anxiety Disorder Questionnaire (GAD-7) is a 7-item scale commonly used as a measure of general anxiety symptoms across various settings and populations. 84 Scores range from 0–21, with higher scores indicating greater anxiety. Psychometric properties include excellent reliability (Cronbach's α = 0.92); good test-retest reliability (ICC = 0.83) and procedural validity (ICC = 0.83). The Cognitive Fusion Questionnaire (CFQ-13) is a 13-question measure assessing the degree of rigid attachment to thought content. 85 Scores range from 13–91 with higher scores indicating greater attachment (i.e., poorer ability to separate from thoughts). Psychometric properties include good to excellent reliability (Cronbach's α = 0.88–0.93) and good test-retest reliability. The Huntington's Disease Quality of Life Questionnaire (HDQoL)86,87 captures various facets of health-related quality of life, including physical and cognitive functioning, and worries and mood. A fifth domain pertaining to HD-related services was not evaluated as it was not relevant to the intervention. Scores range from 0–100; higher scores indicate greater health-related quality of life. Psychometric properties include acceptable or better reliability (Cronbach's α = ≥0.7 across scales) and acceptable or better test-retest reliability (ICC ≥ 0.7 across scales).
Results
The patient's scores on symptoms of depression and anxiety were reduced following the intervention, as were his scores associated with cognitive fusion. The patient's quality of life scores increased in the domains of physical functioning, worries, and mood, indicating higher quality of life in those areas, and decreased in the cognitive domain (see Table 3).
Baseline and post-intervention scores.

Depressive symptoms were measured using the PHQ-9 (range 0–27); higher scores indicate more depressive symptoms.
Anxiety was measured using the GAD-7 (range 0–21); higher scores indicate greater anxiety.
Cognitive fusion was measured using the CFQ-13 (range 13–91); higher scores indicate greater levels of cognitive fusion (i.e., poorer ability to separate from thoughts).
Quality of life was measured using four subscales of the HDQoL (range 0–100); higher scores indicate greater health-related quality of life.
With regard to clinical significance of these changes, the minimum clinically important difference (MCID) for the PHQ-9 and GAD-7 are estimated to be 3.7 and 4.0, respectively88,89; there is no established MCID for the HDQoL or CFQ-13, which limit our ability to fully interpret these changes. The patient's reduction in depressive symptoms from 11 to 6 on the PHQ-9 was clinically meaningful, moving from “moderate” to “mild” in severity. Contrastingly, the patient's anxiety symptoms as measured by the GAD-7 decreased by a single point from 11 to 10 (remaining in the moderate range). This reduction is far below the MCID of 3.7 points and thus better interpreted as a non-meaningful change. The patient's quality of life score increased most in the domain of physical functioning, followed by the domain of worries. Without an established MCID, it is difficult to fully interpret these score changes, though in both cases the patient's score increased by ≥15%. The patient's score within the mood domain increased more modestly by 3.3 points (7%). Lastly, the patient's degree of cognitive fusion diminished by 11 points (16%), suggesting that following the intervention, he was less attached to his thoughts and had increased capacity for flexibility in his thinking. While no formal qualitative data was collected regarding the intervention, both the patient and caregiver provided strongly positive feedback following the final session, both stating that they enjoyed the sessions and found the exercises to be meaningful and engaging. Although the intervention was primarily focused on the patient, his caregiver shared that she felt better following the intervention, stating that listening to the session content and thinking through the concepts that were presented had helped her cope with her caregiving role. Further, she was highly engaged in the ACT intervention, choosing to attend all sessions and participating for the duration of each session. Her involvement in the intervention led her to make behavioral changes in her life. For example, she identified “caring” as a core value. After reflecting on this value, she identified that although she seemed to have endless capacity for caring for others, she had largely abandoned care of herself, including making time for healthy eating and exercise, leading to clear targets for committed action. Given that the discrepancy between expectations and reality has been noted in the literature as a large contributor to caregiver burden, 90 finding novel and workable ways to engage in committed action in the face of caregiving responsibilities, while returning to the present moment when faced with worries about the future, are likely to be centrally important when considering applications of ACT to caregivers. In this case, the caregiver's steps toward clarifying her value of caring and attuning to committed action steps, while also maintaining realistic expectations, led to her changing her diet and exercise routine.
With regard to qualitative feedback from the therapist (author SHS, who had prior experience delivering the intervention to individuals with other chronic health conditions), the intervention was highly adaptable and applicable to HD, which facilitated engagement from both the patient and his caregiver and made for a highly positive experience delivering the intervention.
Discussion
There is a need for further investigation of ACT to support individuals with HD and their caregivers. The patient's improvement in depressive symptoms and quality of life suggests that ACT holds promise as an intervention to support this population. In only 6 sessions, the patient not only experienced psychological benefit in that his depressive symptoms were reduced substantially – far exceeding the MCID – but also in the improvement in quality of life across three domains. These improvements suggest that ACT may benefit HD not only psychologically but also in terms of physical health and functioning. This is consistent with previous studies wherein ACT was found to improve physical functioning. 15 While we did not examine the mechanism of change, improvement in physical functioning may have been due to increased engagement in health-promoting behaviors as a result of enhanced psychological flexibility, a mechanism that has been proposed previously. 91 Alternatively, these changes could have resulted from the patient's increased clarity about his values and improved defusion skills, leading to greater motivation to engage in values-aligned activities, and greater ability to defuse from thoughts that were previously obstacles to engagement.
In contrast with these improvements, the patient's anxiety score did not diminish meaningfully. Given the patient's severe OCD symptoms, it unsurprising that anxiety remained in the “moderate” range. During the 6-session intervention, sessions were not focused on his OCD symptoms (which has been the focus of his treatment during the prior nine months) and thus the fact that anxiety did not increase may be viewed as a positive outcome. While ACT may not be able to reduce anxiety in HD patients with severe OCD, it may nonetheless reduce overall distress by changing one's relationship with their thoughts and feelings. Additionally, the patient's quality of life score did not improve within the cognitive domain. We view this small score decrease as a non-meaningful change (the pre-post difference of 1.44 points is the smallest of the four HDQoL measured). This lack of improvement is consistent with the expected degenerative course of HD and the fact the intervention was not intended to target cognition. While it may not be realistic for ACT to halt cognitive decline, these findings suggest that it may nonetheless aid in living a life that has meaning, even in the face of that decline.
Future directions
While a single case of successful treatment is far from the evidence needed to establish effectiveness of ACT with HD patients, the reduction in this patient's symptoms coupled with his and his caregiver's positive appraisal of the intervention is promising and serves as a proof of concept, warranting further research. Given that this intervention was delivered as a part of routine practice (rather than as part of a research study), and thus the patient's caregiver did not complete any measures before or after the intervention, we are not able to speak to the impact of the intervention on her mental health. Future research should formally investigate the impact of ACT on caregivers of individuals with HD. Additionally, the patient had been receiving prior CBT-based treatment in the clinic, which may have impacted (either in amplifying or attenuating) the effect of the ACT intervention. Future empirical research is needed to more rigorously understand the impact of ACT on the mental health of HD patients and their caregivers.
There are many exciting questions at the intersection of ACT and HD that warrant future study. First, there is a need for randomized controlled trials examining the effectiveness of ACT in supporting HD patients and their caregivers. This may be done using a relatively brief intervention, such as the one used with this patient, or with other ACT-based protocols. While no such trials have been published to date, results of ongoing studies will contribute to the limited literature on this topic.77,78 Data from a randomized trial will allow for a stronger empirical evidence base to guide next steps in building networks of psychological support for HD patients and their caregivers. If ACT is found to be effective, this data can be leveraged to implement accessible and scalable psychotherapy interventions.
If empirical support is established, future research will also be needed to understand how best to implement ACT for HD, including research on feasibility and accessibility, delivery format (i.e., in person vs. virtual), and whether to engage patients and caregivers dyadically or individually. Further, questions remain regarding the optimal point at which ACT should be offered. Given that psychological and emotional symptoms in HD may begin years before an official diagnosis, ACT has potential utility even before physical symptoms begin. Further, given the widespread availability of genetic testing for HD, it may be that an ACT intervention adapted for known gene expansion carriers may be useful, given the wide range of psychological reactions that often accompany predictive genetic testing. 63 Given the theoretical evidence presented and the promising outcomes of the case discussed, further assessment of ACT for HD patients and caregivers is warranted as it may support individuals affected by HD in building meaningful lives even in the face of painful experiences.
Conclusion
This narrative review and case study captures the promise of ACT as an intervention to support individuals with HD and their caregivers and highlights the need for further study. Although the empirical literature evaluating ACT with HD patients and caregiver is extremely limited, there is a more robust evidence-base supporting the use of ACT with individuals with other neurodegenerative disorders. To our knowledge, this is the first published case report examining the use of ACT with a HD patient and caregiver. Given the symptom reduction and improved quality of life documented in the case report, as well as the positive qualitative feedback provided by the patient, his caregiver, and the therapist, further empirical study that more rigorously evaluates use of ACT within this population is warranted. Such data will guide the way toward a future where effective interventions for individuals with HD and their caregivers are widely accessible.
Supplemental Material
sj-docx-1-hun-10.1177_18796397251315162 - Supplemental material for Acceptance and commitment therapy with Huntington's disease: A narrative review and case report of a caregiver-assisted intervention
Supplemental material, sj-docx-1-hun-10.1177_18796397251315162 for Acceptance and commitment therapy with Huntington's disease: A narrative review and case report of a caregiver-assisted intervention by Simone H Schriger, Chelsi N Nurse and C Virginia O’Hayer in Journal of Huntington's Disease
Footnotes
Acknowledgments
The authors have no acknowledgments to report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data sharing is not applicable to this article as all data underlying the results shared are available as part of the manuscript, and no datasets were generated or analyzed during this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.