
Abstract
Background
Cognitive impairment in Huntington's disease (HD) is a key driver of disability that can have deleterious impacts on everyday functioning. Currently available patient-reported outcome measures may not adequately capture the impact of HD-related cognitive impairment on daily life, particularly higher-order executive functioning (i.e., processing information, decision making, multi-tasking, planning, etc.).
Objective
To address the unmet need to better quantify the functional sequelae of HD-related cognitive impairment by developing the Huntington's Disease Everyday Functioning (Hi-DEF) scale.
Methods
Qualitative interviews were conducted in two adult cohorts (25–65 years) with early stages of HD (i.e., huntingtin [mHTT] gene carriers with self-reported cognitive complaints but could still function independently). Cohort 1 included 10 dyads of participants with HD and their care partners, who completed concept elicitation interviews to identify cognitive challenges impacting everyday tasks, which was used to design a draft item-set. Cohort 2, which included 15 additional participants with HD, cognitively debriefed this item-set.
Results
In Cohort 1, issues with executive functioning were reported 32 times by participants with HD and 22 times by care partners, and challenges with functioning were reported 46 times by participants with HD and 20 times by care partners. Based on these reports, the Hi-DEF scale was developed and cognitive debriefing interviews evaluated its content validity, relevance, clarity, interpretation, and acceptability. Psychometric validation of the Hi-DEF scale is reported elsewhere.
Conclusions
These interviews revealed the impact of HD-related cognitive impairment on everyday functioning and supported the content validity, relevance, clarity, interpretation, and acceptability of the Hi-DEF scale.
Introduction
Huntington's disease (HD) is a rare, genetic neurodegenerative disease characterized by progressive cognitive, behavioral, and motor decline. 1 The disease is caused by a cytosine-adenine-guanine (CAG) trinucleotide repeat expansion within the huntingtin (HTT) gene that accelerates neuronal degeneration and damage. 2 Approximately 40,000 individuals in the US are diagnosed and currently live with HD, and an additional 200,000 people are HTT gene mutation carriers who are at high risk for developing the disease.3,4 The average age of onset is approximately 40 years.5,6 At this time, there is no therapy to stop or slow the progression of HD, and available approved treatment options are largely focused on alleviating motor symptoms. 7 While symptoms of HD generally include a triad of cognitive, behavioral, and motor impairments, the former two symptoms are especially disruptive and distressing to individuals with HD.
Cognitive and behavioral symptoms can appear 10–15 years before perceptible motor symptoms, often when people are in their prime working years or the height of managing home and work responsibilities.8,9 Therefore, these cognitive symptoms in the early stages of HD may initially pose a bigger burden on individuals than motor symptoms. Clinically, cognitive impairment in HD is multifaceted and may include difficulties in processing of information, memory, attention, communication, decision making, multi-tasking, planning, and organizing.8,10 Although early cognitive decline may not always be detectable by patients with early stages of HD, these changes may be expressed more saliently through their impact on daily activities, such as engaging in work, performing chores, or driving a vehicle.9,11–13 For example, an analysis of data from the Enroll-HD observational study reported that cognitive impairment due to HD is a significant contributor to patients’ inability to maintain employment. 13
Patient-reported outcome (PRO) measures provide valuable insights into changes in a patient's perceptions of well-being, ability to function independently, and overall quality of life. The U.S. Food and Drug Administration (FDA) has noted the importance of incorporating patient perspectives when evaluating treatments, as this information can inform consideration of benefit‒risk tradeoffs. 14 Such measures focus on a patient's responses in order to evaluate how they feel, ability to function, and the effect of therapeutic interventions. 15 This information can help uncover and highlight important patient-relevant endpoints in clinical studies of novel HD interventions.
Despite the burden of cognitive impairment and subsequent functional loss, standardizing assessment and quantifying impact is challenging due to the limited availability of PRO measures with sufficient sensitivity to capture emergent cognitive and behavioral changes, particularly from patients’ perspectives.16,17 Tools such as the HD-PRO-TRIADTM, Huntington Disease Health-Related Quality of Life (HDQLIFETM), and Functional Rating Scale 2.0 (FurST 2.0) offer valid and reliable PRO measures of HD-specific health-related functioning and quality of life items.18–20 Despite the utility of these and other HD-specific PRO measures, subtle cognitive changes in the early stages of HD may not be fully captured by these PRO measures or may even go undetected.19,21 More specifically, while broader aspects of cognition may be recorded in current measures, higher-order executive functions integral in daily life, affecting working, driving, and social functioning, may not be adequately captured.19,21
There is a need for a PRO measure that evaluates HD-related cognitive impairment and its impact on daily functioning, to reflect the first-person perspective in the early stages of HD. It is important to assess impairment in executive functioning and standardize how it is measured and recorded in HD, particularly for new therapeutic interventions and clinical trials. Given the importance and need for this type of measure, the objective of this qualitative study was to develop the Huntington's Disease Everyday Functioning (Hi-DEF) scale, which assesses HD-related cognitive impairment and its impact on everyday functioning. Participants with HD and their care partners were interviewed to better understand their everyday experiences, identify cognitive concepts that impact this population, and guide the development of this novel HD-specific PRO measure.
Materials and methods
Study design and participants
Participants in the study were recruited through two HD patient advocacy organizations: Huntington's Disease Society of America (HDSA) and Huntington's Disease Youth Organization (HDYO), using social media posts and email notices. This study was conducted between December 2019 to August 2020 and comprised a series of qualitative interviews among two cohorts of individuals from the United States with early stages of HD and their care partners. The care partners were included to understand the carer perspective on the impact of cognitive impairment of the participant with HD on their functioning and evaluate differences, if any, between the accounts of the participants with HD versus the care partners. The first cohort (Cohort 1) was comprised of participants with HD and their care partners and was interviewed to identify symptoms and functional abilities impacted by cognitive impairment due to HD, which were used to guide development of a draft item-set for a novel HD-specific PRO measure, the Hi-DEF scale. Cognitive debriefing of the draft item-set of the Hi-DEF scale was conducted with the second cohort (Cohort 2), consisting of participants with HD only, in order to further refine its development. This qualitative research study received central institutional review board approval and was conducted in accordance with ethical principles originating in the Declaration of Helsinki. All participants were compensated after completing the interviews. The sections below describe the interview processes in detail. Interview and cognitive debriefing guides for participants with HD are available in Supplementary Item 1; the interview guide for care partners is included in Supplementary Item 2.
Inclusion/exclusion criteria
Participants with HD between the ages of 25 and 65, and self-reported mutant huntingtin (mHTT) gene positive carriers with cognitive symptom complaints but still functionally independent were included. Additionally, in order to ensure inclusion of individuals in early stages of HD with some cognitive and functional changes while at the same time not being severely motor impaired, the study required a CAG repeat of ≥ 36. Since age of HD onset and HD penetrance can be associated with the number of CAG repeats,22,23 criteria were applied to establish a lower and upper limit of impairment within which all participants would fall. Participants with a CAG repeat between 36 and 40 must have noticed changes in their ability to manage work, manage finances, activities of daily living, or household chores, and those with a CAG repeat greater than 40 must still be able to perform some aspects of their usual work and household chores, manage finances with assistance, and perform activities of daily living with minimal impairment.
Self-reported cognitive symptoms included impairment in memory, decision making, multi-tasking, concentration, and/or following directions. Participants with HD who had been diagnosed with an ongoing neurological condition other than HD, had participated in any investigational drug or clinical drug trial within the last 180 days, or had a history of neurosurgical intervention or significant head injury were excluded from this study. A care partner was defined as someone who had intimate knowledge of the functional capabilities and daily life experiences of the participant with HD. Care partners were required to be adults (≥18 years of age), with no risk for or a carrier of HD, and had spent at least 10 h per week with the participant with HD since diagnosis.
Data collection
Concept elicitation and cognitive debriefing interviews were conducted by three research team members (AL, AR, and TL) by phone and each interview was audio-recorded and transcribed. Interviews lasted 60 min on average. Each participant provided written informed consent prior to enrollment and was compensated for completing their interviews. Before each interview, interviewers introduced themselves, the study objectives and procedures, and allowed the study participants to ask any questions before starting the recording. Semi-structured qualitative interview guides were used by each interviewer.
Concept elicitation interviews
In concept elicitation interviews, Cohort 1 was asked open-ended questions to elicit participants’ experiences in their own words with the aim of understanding how cognitive symptoms or impairment impacted the daily functioning of the participant with HD. Qualitative interviews were conducted by phone with dyads of participants with HD and their respective care partners; participants with HD were interviewed separately from their care partners. In order to understand the concepts important to participants’ functioning at the early stages of disease, interviewers conducted these interviews with each dyad to identify cognitive symptoms and challenges with functioning from both the perspective of the participant with HD and the care partner. Probing follow up questions captured functional impairments experienced while at home or at work if the respondents were still working.
Cognitive debriefing interviews
Following concept elicitation, a draft item-set of the Hi-DEF scale was created to describe the array of functioning difficulties experienced, which were obtained directly from participants. These concepts were grouped by framework domains to ensure independent functioning was captured broadly, including experiences at home, at work, while driving, and while socializing or communicating. The items were reviewed to ensure a wide range of cognitive concepts were covered, including that of executive functioning.
Further refinement of the drafted scale was achieved by reviewing and determining instructions, recall period, response options, and item-set amongst the researchers. These categories were utilized to revise the item-set which then underwent cognitive debriefing with Cohort 2, which was comprised of 15 participants with HD only (no care partners). A think-aloud method was used, which asked the participants to verbalize their thoughts as they completed the questionnaire. Cognitive debriefing interviews were conducted to examine the items to assess content validity, relevance, clarity, interpretation, and acceptability.
Quantitative analyses
Demographic and health information data (i.e., questions related to HD-specific factors and their general health) were collected via electronic forms, and descriptive statistics were generated. To establish a baseline score on a validated instrument, all participants with HD completed the HD-PRO-TRIAD™, a health-related quality of life instrument assessing cognitive, emotional-behavioral, and motor symptoms of HD. 16 Care partners were also asked about their own general health, the nature of their relationship with the participant with HD, such as the type of care provided, and the amount of time spent alongside the participant with HD.
Qualitative analyses
Concept elicitation
The transcripts were analyzed thematically using detailed open line-by-line inductive coding in ATLAS.ti software (ATLAS.ti Scientific Software Development GmbH). 24 Independent parallel coding was utilized to initiate and ensure consistency in coding among the transcripts from the first 5 participants in concept elicitation. From there, a coding guide was developed by the research team to provide guiding principles and a formatting framework; codes were reviewed and agreed upon after each subsequent set of 5 interviews. Researchers met consistently to discuss the results of analysis and adjust codes as necessary.
A conceptual framework was developed using the analyzed interview data to provide a visual representation of the concepts and their interrelationships. Coding of the concepts was done using standard analytical techniques of conceptual model development.25–27 Codes were organized into higher-order categories, which included concepts and domains. Conceptual saturation analysis was performed to ensure that no new themes, concepts, or terms were introduced as additional interviews were conducted; interviews were grouped by 5 chronologically and analyzed. 28 Saturation was said to be achieved if no new concepts were elicited in the final group of interviews.
Cognitive debriefing
Cognitive debriefing interview transcripts were similarly coded with ATLAS.ti using a deductive approach guided by the topics of interest, including validity, relevance, clarity, interpretation, acceptability, and meaningful change thresholds. As per the methods above, researchers met regularly to discuss codes and adjust the format or style of coding if required.
Results
Demographics and baseline characteristics
In total, 10 dyads of participants with HD and care partner interviews were conducted for concept elicitation, followed by interviews with 15 additional participants with HD for cognitive debriefing. During screening for the concept elicitation phase, 4/20 screened patients were excluded due to participation in a drug or clinical trial within the last 180 days, 3 were excluded due to lack of cognitive symptoms reported by the patient, and 1 was excluded due to a lack of genetic testing. 2 dyads did not respond after multiple contact attempts and were not included.
Overall, both cohorts of participants with HD were generally similar in terms of demographics and baseline characteristics (i.e., mean age, sex, race/ethnicity, and CAG repeat), so the demographics of all participants with HD are reported together. Participants with HD were adults (>18 years of age) diagnosed between 1995 and 2019 for an average of approximately 5.5 years since diagnoses (Table 1), with 50% of these diagnoses occurring between 2017 and 2018. Their CAG repeats ranged from 36 to 48, with 88% reported having >40 repeats. Prior to the interviews, each participant completed the HD-PRO-TRIAD™, which showed a mean total score of 8. The mean age of participants with HD and care partners were 40 and 42 years, respectively; approximately 50% of both groups were female. The majority of both participants with HD and care partners self-reported as non-Hispanic/Latino and White, and between one-fifth and one-third of each group had a bachelor's or postgraduate education. More than half of the participants with HD (64%) were working either full- or part-time, and 70% of the care partners were spouses.
Demographics and baseline characteristics.
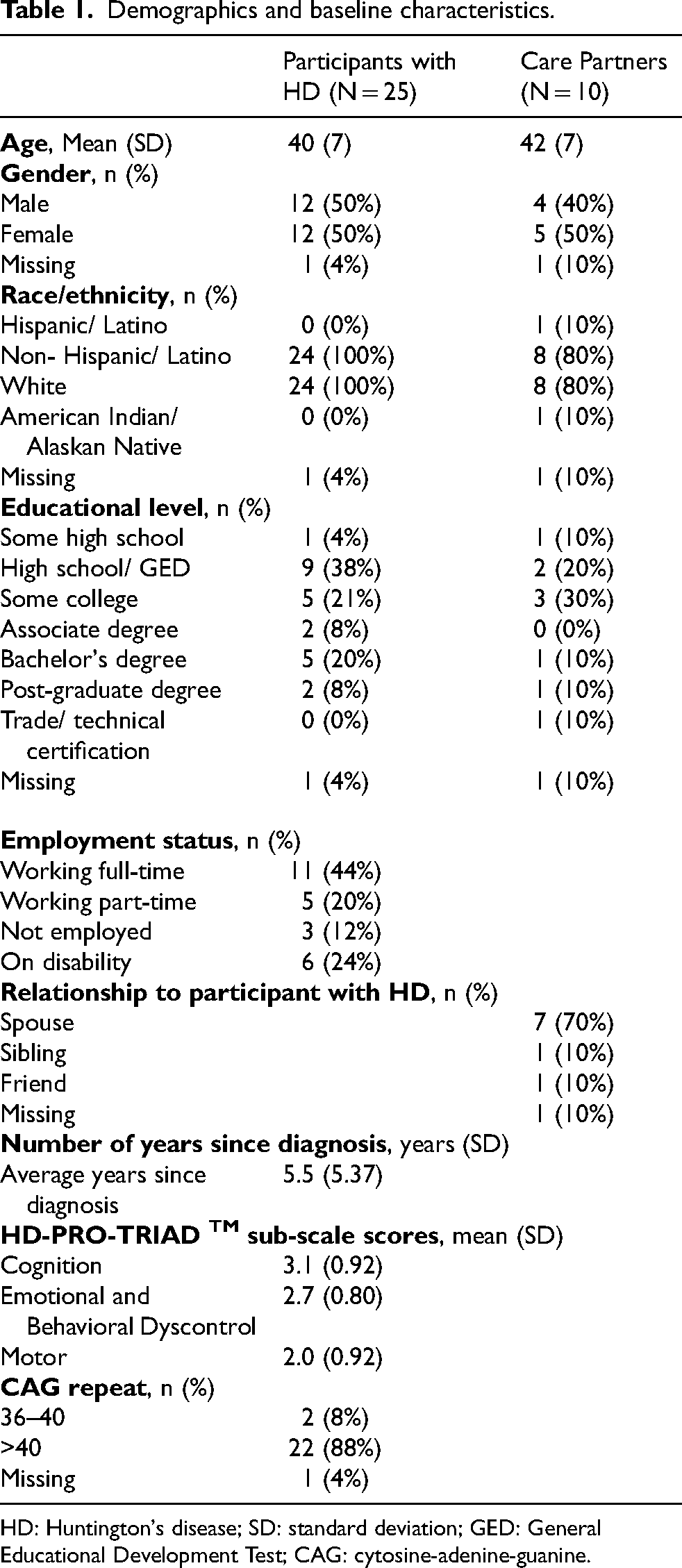
HD: Huntington's disease; SD: standard deviation; GED: General Educational Development Test; CAG: cytosine-adenine-guanine.
Concept elicitation
During concept elicitation, participants in Cohort 1 reported cognitive difficulties, particularly in executive functioning, that impacted the ability of the participant with HD to complete complex tasks in everyday scenarios. The concept elicitation interviews detailed the cognitive symptoms and the challenges with functioning in the early stages of HD in the setting of “At home” (formerly “Daily life”), “At work”, “Driving”, and “Social/Communication” domains. The cognitive constructs and domains are shown in Figure 1.
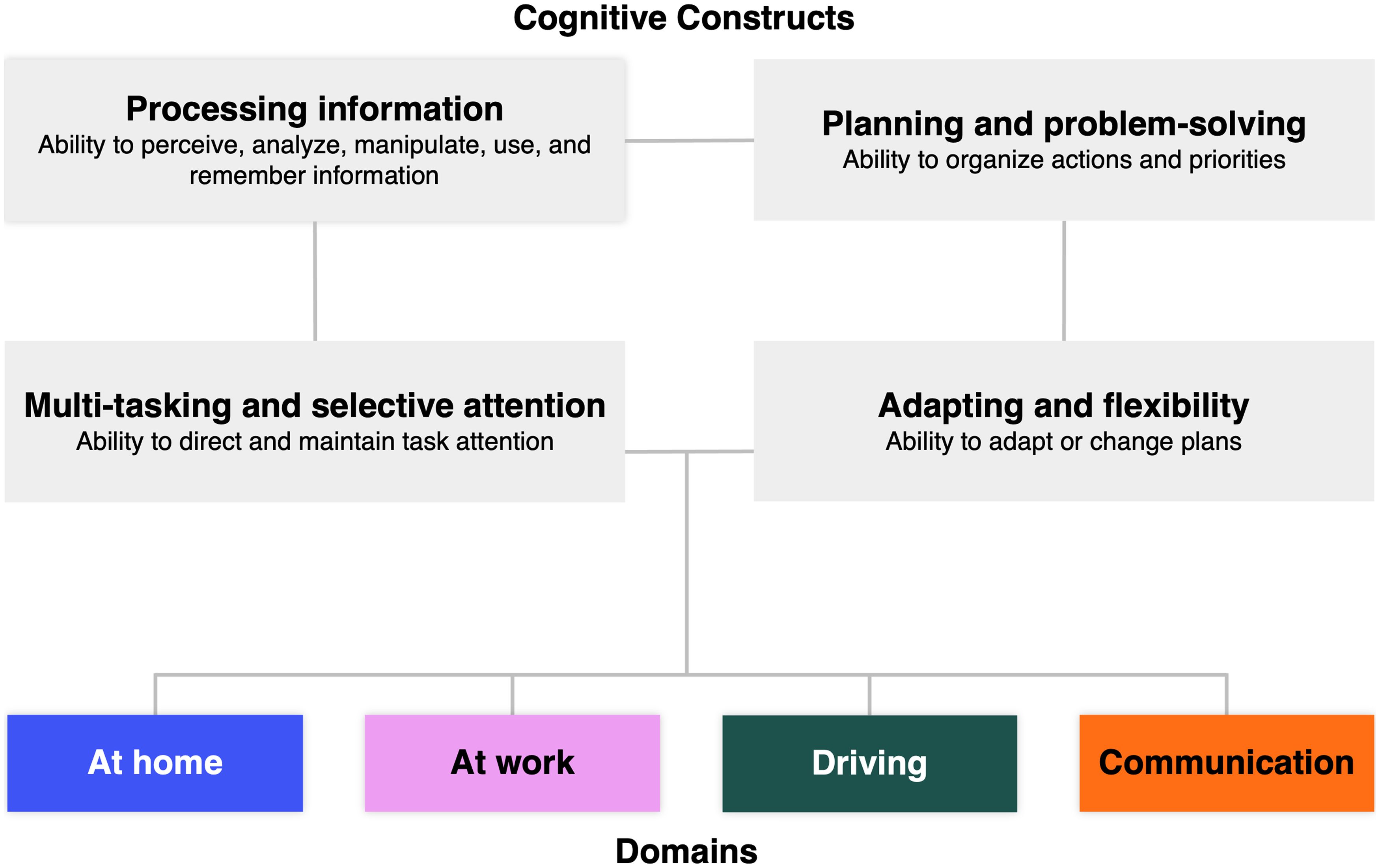
Cognitive constructs and domains from the concept elicitation interviews. Based on participant feedback during the cognitive debriefing interviews, the “Daily life” domain was renamed to “At home”, and the “Social/Communication” domain was renamed to “Communication”.
In the “At home” (formerly “Daily life”) domain, participants with HD reported difficulties with multi-tasking, deviating from planned routines, and processing information (Figure 2). More specifically, participants with HD reported issues with daily activities such as making a meal at home that involved multiple and overlapping steps, learning a new task, or adding to an already established routine. Participants with HD also reported resistance towards deviations from normal routines, while a care partner reported having to take over financial tasks because the participant with HD was not completing them. “There's zero multitasking in my life…if I’m holding ketchup in my hand and I grab mayonnaise in the other, one will drop…And what it causes is like extreme anxiety…” “I haven’t really tried to learn any new tasks. I do the same routine…But for me, I think I’ve already started, not even realizing it, of making a routine for myself and not deviating from it.”
“We do our bill paying on our credit union. And she's not been keeping up with it…So she's kind of leaving things and forgetting things…So I told her that I would like to take it all over…”
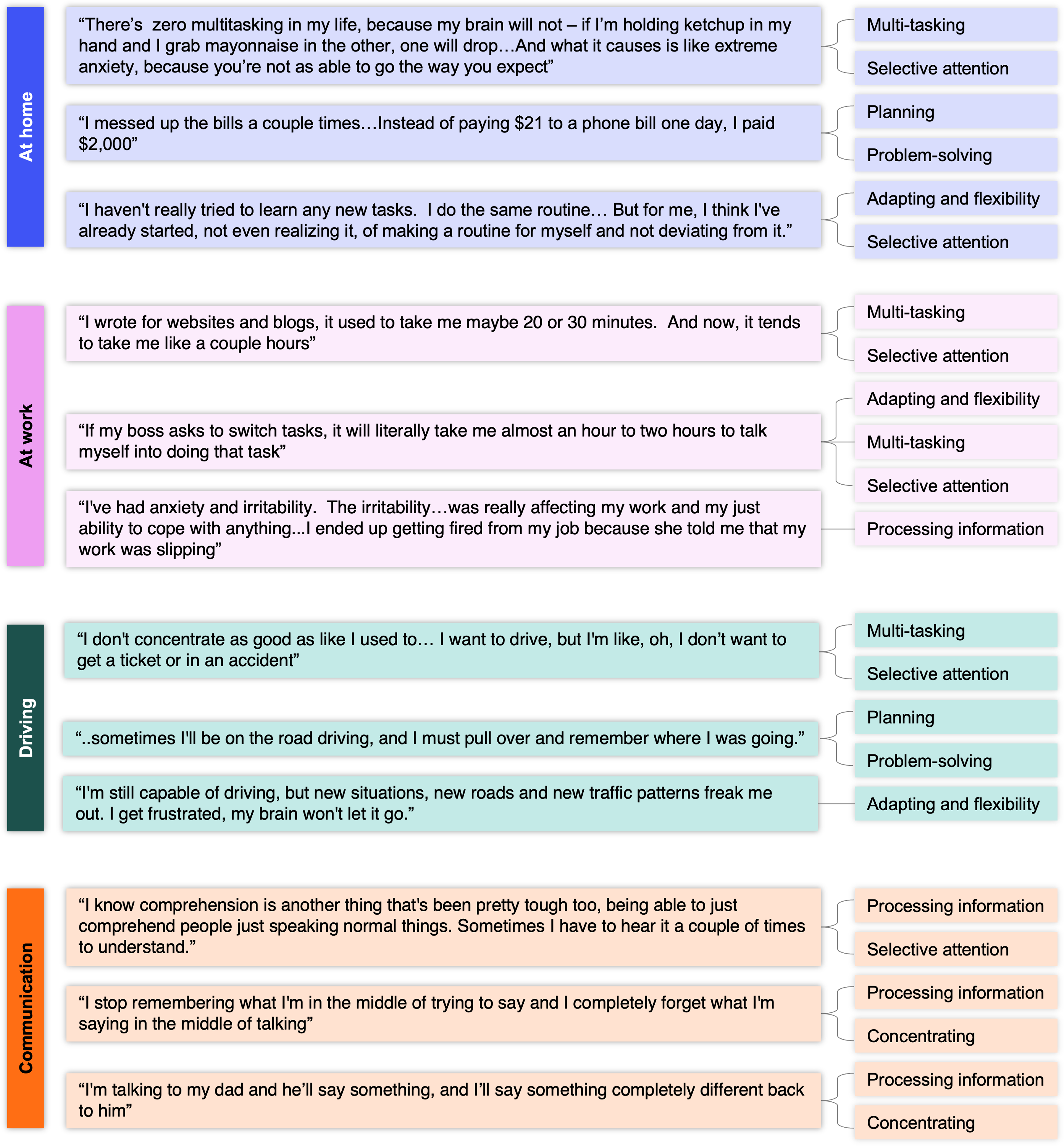
Daily challenges with functioning due to cognitive changes in the early stages of HD. Based on participant feedback during the cognitive debriefing interviews, the “Daily life” domain was renamed to “At home”, and the “Social/Communication” domain was renamed to “Communication”.
Within the “At work” domain, participants with HD reported cognitive difficulties related to multi-tasking and processing information while at work (Figure 2). For instance, participants with HD noticed weakening or loss of the ability to create project schedules, taking acceptable notes, solving mathematical calculations, or interpreting written information. Some participants with HD also revealed how these impairments impacted their ability to work, such as needing additional time to complete the tasks. “The issue is remembering things and being off task, unable to like finish things you start…I noticed that, when I was doing my job at the hospital, I knew something was wrong…charting was supposed to take two hours –I’m taking five.” “I had noticed I’ve been struggling with math in my head a lot…I used to be able to just do this on the fly…” and, “…multitasking was part of my career and scheduling big construction projects from start to finish was my job. I was having a harder time connecting the dots through the construction schedule.”
In the “Driving” domain, participants with HD reported difficulties with deviating from regular routes, selective attention, and multi-tasking (Figure 2). During the interview, these participants expressed how such cognitive impairment impacted them, with one mentioning feelings of frustration and another stating they had to momentarily stop driving their vehicle to remember the destination or route. “I'm still capable of driving, but new situations, new roads and new traffic patterns freak me out. I get frustrated, my brain won't let it go.” “…sometimes I'll be on the road driving, and I must pull over and remember where I was going.”
Within the “Social/Communication” domain, participants with HD reported difficulties with processing information, remembering information, and conveying thoughts (Figure 2). Here, the impact that participants with HD reported included needing other people to repeat words or sentences when verbally communicating and delays in verbal response times while conversing, to the point where it became noticeable to other people. “I know comprehension is another thing that's been pretty tough too, being able to just comprehend people just speaking normal things. Sometimes I have to hear it a couple of times to understand.” “I notice that the amount of time it takes me to sort of think through my response sometimes is longer than I realize or long enough that the other person is annoyed or confused about what I’m doing.”
These responses gathered within the four domains, along with the cognitive constructs, guided the development of the Hi-DEF draft item-set.
Conceptual framework and Hi-DEF draft item-set
The HD-related cognitive difficulties and challenges with functioning revealed by the concept elicitation interviews steered the development of a conceptual framework for the Hi-DEF draft item-set. Most of these concepts were self-reported by participants with HD, while the care partners reported secondhand stories that they heard from or experienced with the participant with HD. Overall, most of the concepts reported by participants with HD and care partners overlapped indicating that individuals in the early stages of HD are able to adequately report on their experiences with cognitive impairment and impact on day-to-day life. The number of concepts reported by participants with HD and care partners are shown in Table 2. The concepts included those related to executive functioning, while challenges with functioning focused mostly on cognitive tasks, instrumental activities of daily living (ADL), and role functioning.
Number of reported cognitive and ADL concepts associated with HD.

ADL: activities of daily life; HD: Huntington's disease.
Executive functioning concepts, including adapting and flexibility, muti-tasking and selective attention, and planning and problem-solving were reported 32 times from the participants with HD in Cohort 1 and 22 times from the care partners. Cognitive tasks (i.e., working, following instructions, multi-tasking, and learning new tasks) and instrumental ADLs (i.e., ability to drive, manage finances, and completing daily household activities) were reported at similar rates by participants with HD, at 19 and 22, respectively. However, care partners overall reported lower rates in both cognitive tasks and instrumental ADLs than participants with HD, and they reported more instrumental ADLs (13) than cognitive tasks (2).
This conceptual framework was utilized in the development of the novel HD-specific PRO measure (Figure 3). The Hi-DEF draft item-set comprised 17 items related to activities in “At home” (formerly “Daily life”), 13 items for “At work”, 9 items for “Driving”, and 8 items for “Social/Communication”, for a total of 47 items. Instructions asked the respondent to consider the past 7 days when reading the items. The rating scale for items related to daily life, work, and driving subsets were based on difficulty from 1 (No difficulty) to 4 (Severe difficulty) and 5 (Cannot do this anymore). Items related to social/communication functioning used a frequency scale of 1 (Never) to 4 (Almost always).
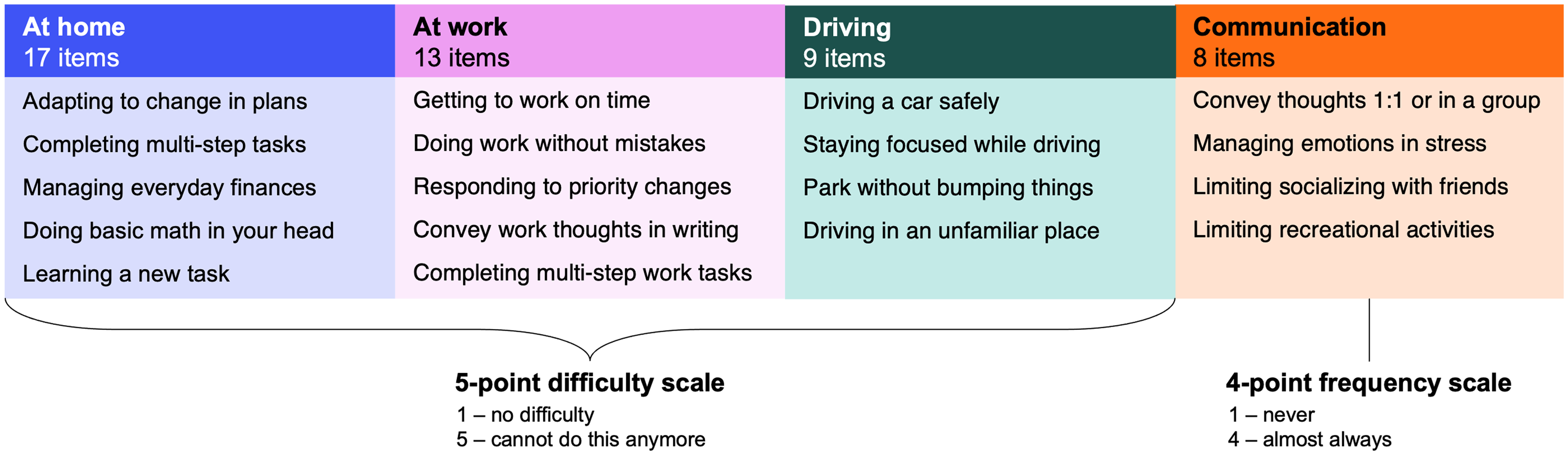
47-item draft item-set with selected activities from the Hi-DEF item list. Domains include 17 items for “At home”, 13 items for “At work”, 9 items for “Driving”, and 8 items for “Social/Communication”, for a total of 47 items. “Daily life” was renamed to “At home”.
Cognitive debriefing
The Hi-DEF draft item-set underwent cognitive debriefing with 15 additional participants with HD for further measure refinement to ensure it covered everyday functioning as it pertained to various daily settings. Based on participant feedback during the cognitive debriefing interviews, the “Daily life” domain was renamed to “At home”, and the “Social/Communication” domain was renamed to “Communication”. Multi-tasking and selective attention “At home” were assessed by inquiring about a participant's experience with completing a multi-step activity or switching back and forth between two different activities, such as cooking a meal and answering the phone. Within Cohort 2, there was mention of changes in multi-tasking and attention when completing household tasks. Planning and problem-solving were assessed in “At work” by asking participants about their ability to complete work tasks on time (Table 3).
Cognitive debriefing: Hi-DEF draft item-set – issues by item.
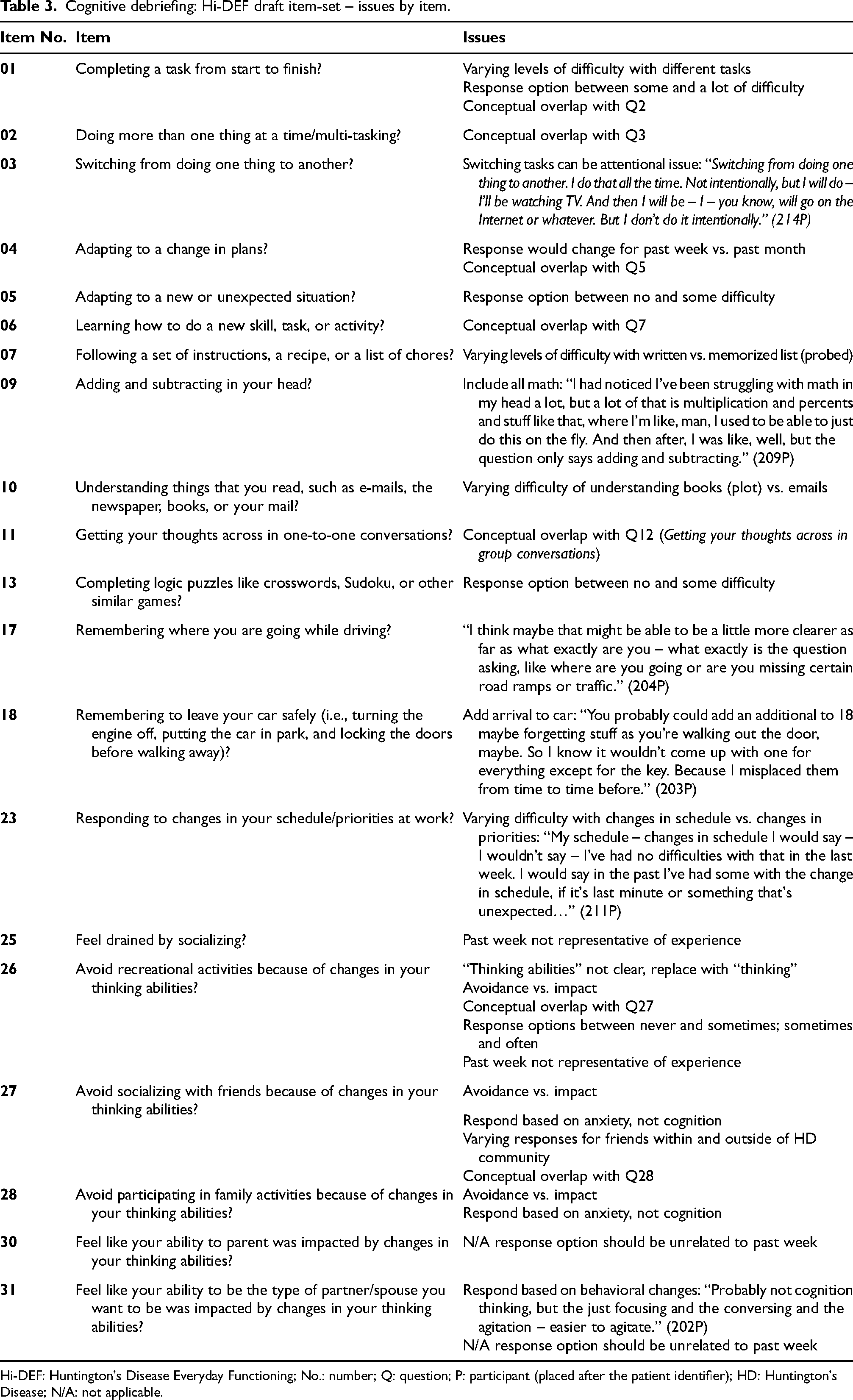
Hi-DEF: Huntington's Disease Everyday Functioning; No.: number; Q: question; P: participant (placed after the patient identifier); HD: Huntington's Disease; N/A: not applicable.
Discussion
This study highlights the negative impact that HD may have on cognitive functioning, particularly executive function, which encompasses adapting and flexibility, multi-tasking and selective attention, planning and problem-solving, and processing information. Quantifying the impact of HD-related cognitive impairment is currently challenging since there are limited HD-specific PRO measures focused on and sensitive to these early and subtle changes. Here, we identified relevant concepts from patient and care partner perspectives, to measure cognitive impairment in the early stages of HD and the associated decline in daily functioning across various settings (i.e., home, work, driving, and communication). Inclusion of care partners and the similarities between reports from both participants with HD and care partners revealed that a PRO which captures self-perspectives can be an effective tool to assess experiences of individuals in the early stages of HD. This led to the construction of the conceptual framework which was utilized to draft the Hi-DEF item-set. The draft item-set then underwent debriefing with additional participants with HD to improve granularity of concepts and relevance.
Our research supports and expands upon previous studies that highlight the impact of cognitive impairment in individuals with HD. In our study, participants with HD reported impairment in multi-tasking and attention when completing household tasks in the “At home” domain, which has been previously observed and supports documented cognitive changes for individuals living with HD.10,29 Impairment in multi-tasking and attention were also reported by care partners in this domain. In one instance this resulted in removing a finance-related task from the participant with HD, which builds upon the executive functioning difficulties reported by caregivers in the literature. 16 Planning and problem-solving were assessed in the “At work” domain by asking participants with HD about their ability to complete work tasks on time, which revealed feelings of frustration when using work-related machinery, even after using the same machines with no issues for multiple years. The inability to work at the same level prior to symptom onset, difficulty planning, and losing the ability to maintain employment in individuals with HD has been similarly reported. 10 Our findings aligned with cognitive impairment previously reported in the literature and further support the need for a cognitive-focused measure for HD.
Some recent progress has been made in generating cognitive-focused measures, particularly through the development of the Huntington's disease cognitive functional rating scale (HD-CFRS). 21 The HD-CFRS could stratify patients by cognitive impairment (cognitively preserved, mild impairment, or dementia) and emphasizes the role of key informants in accurately identifying the extent of cognitive impacts in HD. 21 With Hi-DEF more specifically addressing the impacts to work, finances, driving, communication, and the emotional and behavioral dimensions of socialization, which are not covered by the HD-CFRS, both scales can complement each other and help in better understanding patient experiences with HD. The range of domains measured by Hi-DEF, which were identified by patients and influenced their quality of life and functioning, are often under-represented in existing PRO measures.
One such daily challenge with functioning due to HD that is not fully evaluated by the current HD-specific PRO measures is driving. Loss of driving is a significant milestone in the path to loss of independence, and cognitive symptoms have been linked to driving impairments in individuals with HD. 30 Driving is a cognitively demanding task that cannot be performed well when executive functioning is impaired. This important and widely performed skill warrants capturing in the early stages of HD, beyond the motor-related symptoms. Although the FuRST 2.0, which launched in 2018, is a measure used in the early stages of HD that contains a driving assessment, it includes a mixture of both motor and non-motor domains.20,31 Given that cognitive symptoms tend to arise several years prior to motor symptoms, it would be beneficial to have a measure tailored to cognitive impairment since motor-related impairment may not be immediately relevant for some individuals in the early stages of HD.11,12,32 For this reason, the Hi-DEF scale includes a 9-item “Driving” domain. During the cognitive debriefing interviews with Cohort 2, driving was a relevant concept for all 15 participants with HD.
PRO measures provide key insights into the patient experience and have the potential to impact current and new interventions. 14 The FDA has acknowledged that patients’ perspectives can reveal or highlight the disease burden, outcomes, and risks to consider when evaluating treatments, which makes the development of the Hi-DEF scale relevant for future HD-specific clinical trials. 33 This further highlights a clear need for incorporation of patient-centered information in the clinical setting.15,34 For this reason, we aligned with the FDA recommendations from the Patient-Focused Drug Development (PFDD) guidance document to ensure appropriate collection and reporting of patient experience data. 35 More specifically, the interviewers utilized a script to standardize interview questions during the concept elicitation and used open-ended questions, while a think-aloud method was used with participants with HD during cognitive debriefing. These efforts, among others, aided in ensuring patients’ perspectives were properly captured. Measures such as the HD-PRO-TRIADTM and the HDQLIFETM collect an array of important HD-specific concepts, particularly motor-related items. However, these measures may not thoroughly assess cognitive impairment that can occur in the early stages HD, such as executive functioning, impact on driving, and other complex daily activities.13,16,19 Furthermore, HD-related cognitive impairment has been described as less noticeable than motor and behavioral changes, which may underscore the need for a measure with increased sensitivity. 6 In such instances, a measure like the Hi-DEF scale can appropriately capture the nuances of cognitive impairment that interferes with daily activities and may help in evaluating the full therapeutic potential and impact of interventions in the future. This in turn can help with translating the clinical meaningfulness of cognitive performance measures and aid in evaluating the value of novel HD treatments.
While this study provides an important concept-driven measurement approach for patients in the early stages of HD, there are study-specific limitations. First, the sample of interviewees may not fully represent the population in the early stages of HD at large. The small sample size (n = 25 participants with HD) limits the generalizability of this population, and future studies will continue to validate the Hi-DEF scale and its applications in various populations. Similarly, although previous studies have reported the majority of participants diagnosed with HD identified as White, all participants in this study self-reported as non-Hispanic/Latino and White, which could potentially skew our findings.2,36 This may also be applicable to the participants’ educational levels and their time availability to complete a phone interview. During the recruitment period, individuals may have been aware of this study's focus on cognition; therefore, there is a possibility that the participants were more likely to be experiencing, and to have an awareness of, cognitive symptoms. The study's recruitment based on self-reported cognitive symptoms may have under-sampled individuals with anosognosia, who are unable to identify the cognitive impacts of their HD, as well as those individuals who have fewer cognitive symptoms overall. Incorporation of the Anosognosia Scale 37 or a similar instrument could have further characterized the enrolled population. This characterization could have provided insight into the study population's incidence of anosognosia and its level of alignment with anosognosia prevalence in the general population with HD. The literature lacks consensus on how widespread anosognosia is among individuals with HD, and on whether it is associated with other markers of disease severity; however, a 2022 study suggests that anosognosia may be more common than prior research had indicated. 38 As such, the impact of anosognosia on Hi-DEF ratings and the utility of the Hi-DEF in characterizing the experiences of individuals with anosognosia should be explored in future studies. Such studies could include prospective application of the Hi-DEF scale, irrespective of whether patients self-report cognitive impairment.
The participant's ability to accurately gauge and describe their experiences is an important factor in research related to PROs, despite efforts to make the Hi-DEF scale cognitively accessible. The extent of cognitive impairment that occurs in the early stages of HD may affect the reliability of PROs, including the Hi-DEF scale, 12 however, we found the concepts reported by care partners to align with the experience of participants with HD. Similarly, self-reporting of cognitive symptoms and impacts is limited in its ability to fully distinguish between the effects of HD and comorbid conditions that may affect cognitive function. For example, psychiatric comorbidities and potential psychiatric symptoms of HD 39 may each affect cognitive function and cannot be distinguished independently by this measure. Further psychometric and validation analyses are underway, after which the Hi-DEF scale will likely be finalized. The impact of self-reporting across HD stages should be explored in the psychometric evaluation of the measure. Informant-based and exam-based measures could also be used alongside the Hi-DEF scale in potential clinical trial applications, in order to supplement this PRO metric with additional data.
In summary, we developed the Hi-DEF scale to capture subtle cognitive impairment due to HD that impacts a patient's daily life, based on responses from participants with HD and care partners during the concept elicitation and cognitive debriefing interviews with additional participants with HD. These interviews provided support for the content validity of the Hi-DEF scale and that the instrument and its concepts are clear, relevant, accepted, and interpreted as intended by individuals with HD. Furthermore, they revealed the impact of executive functioning impairment in the early stages of HD and the associated decline in daily functioning. Further investigation of both the cognitive and functional impairments HD has on the quality of life and the Hi-DEF scale is needed to aid in the thorough evaluation of future interventions.
Supplemental Material
sj-docx-1-hun-10.1177_18796397241289044 - Supplemental material for Cognitive impairment in Huntington's disease and its impact on functioning: Concept elicitation and cognitive debriefing for the Huntington's Disease Everyday Functioning (Hi-DEF) scale
Supplemental material, sj-docx-1-hun-10.1177_18796397241289044 for Cognitive impairment in Huntington's disease and its impact on functioning: Concept elicitation and cognitive debriefing for the Huntington's Disease Everyday Functioning (Hi-DEF) scale by Jennifer Petrillo, A Alex Levine, Jason Johannesen, Teya Lovell, Alissa Rams, Stefan Cano, Karen Anderson, Jennifer Klapper and Aaron Koenig in Journal of Huntington's Disease
Footnotes
Acknowledgments
We would like to thank the patients with HD, their families, and the investigators for their support & participation in the study. We would also like to thank Emily Gusse (Sage Therapeutics, Inc.) for help with study preparation and Ruta Sawant (Sage Therapeutics, Inc.) for help with manuscript development. Medical writing and editorial support were provided by Auma Muttu and Francie Moehring-Moskal, PhD of Boston Strategic Partners, Inc., and funded by Sage Therapeutics, Inc.
Funding
The study was funded by Sage Therapeutics, Inc.
Declaration of conflicting interests
Jennifer Petrillo and Jason Johannesen are employees of Sage Therapeutics, Inc. and may hold stock and/or stock options. Aaron Koenig was an employee of Sage Therapeutics, Inc. at the time of this study and may hold stock or stock options. A Alex Levine, Teya Lovell, Alissa Rams, and Stefan Cano are employees of Modus Outcomes, a division of THREAD, which received payment from Sage Therapeutics, Inc. to conduct this research. Karen Anderson is an Editorial Board member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer review. Jennifer Klapper reports no relevant conflicts of interest.
Data availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.