
Abstract
Introduction
Huntington's disease (HD) is one of the most complex and debilitating long-term neurological conditions 1 due to the variety, severity, and progression of symptoms associated with functional disability. People with symptomatic HD experience motor (e.g., uncontrollable movements), cognitive (e.g., impaired thinking and decision making), and psychiatric problems (e.g., depression and suicidality). 2 In addition, HD is hereditary, with each offspring at 50% risk of inheriting the gene mutation,3,4 meaning HD affects families across generations.
Evidence shows a high psychiatric burden in individuals diagnosed with HD, compared to the general population, including a higher incidence rate of psychotic disorders, depression, insomnia, dementia, weight loss, pneumonia, and falls. 5 Due to its complexity, both individuals with HD and HD carers, experience substantial burden, with worse mood, quality of life, and social isolation when compared to people living with other long-term neurological conditions.6–9 Although incidence and prevalence of the disease are unknown in England, using United Kingdom (UK) based estimates, we calculate that yearly approximately 410 people are newly diagnosed with HD, 10 with a minimum prevalence of 6 000, 11 and increasing over time. 5 A UK cohort study identified that people's risk of death is four times higher in HD, with a median survival of approximately 12 years from diagnosis. 5
Research has highlighted that the multidimensional features of HD require input from multiple health and social care professionals to support people's needs, as well as a personalized care plan across the lifespan for people living with HD and their family.12–16 Evidence also identifies shortcomings in the health and care system's response to meeting the complex needs of people living with HD,17–19 alongside unequal access to care and support.1,12,20 In light of this, health and social care policy has underlined the importance of integrated care to improve the outcomes for public health and care users.21,22
However, to date little is known about whether, or to what extent, the complex needs of people living with HD are currently being met through multi-sectoral action. 23 Furthermore, evidence is lacking on how to develop, implement and improve programs seeking to integrate care and support for people living with HD.23,24 This is particularly important when trying to solve care fragmentation 25 experienced by people with such chronic conditions, as this is a major contributor to low-quality care, negative health outcomes and unnecessary admissions/re-admissions - with associated costs.26,27 As such, there is a need to compare current health and care provision with service users’ perspectives of what good care looks like, and to establish a national baseline to facilitate assessment of future system developments, ensuring people are kept at the heart of change.
To accomplish this, we sought to identify the current standard of care received by service users living with HD in England, and to explore the extent to which people experience an integrated response to their care needs. Consequently, this user-driven research will advance our understanding of what good care means from the perspective of those affected, providing a foundation for tailoring care services to meet their needs.
Materials and methods
Project design
This study is part of a mixed-methods sequential explanatory research project, aiming to develop a model of integrated care that addresses the needs of people living with HD in England. The project consists of three phases, which foundation was set by a systematic literature review: 23 Phase 1 – Exploratory, Survey (Integrate-HD, currently described); Phase 2 – Design, Case studies, in-depth semi-structured interviews and stakeholders consensus workshops; Phase 3 – Integration, data integration phase following Cresswell and Clark. 28
Survey design
The Integrate-HD survey is a quantitative cross-sectional survey, designed to benchmark current HD care provision in England, from the perspective of service users. To maintain rigor, the Integrate-HD survey was developed based on the Equator Network Checklist for Reporting of Survey Studies (CROSS) guidelines. 29
The survey design was based on the findings from a systematic literature review of the international evidence of integrated care in three long-term neurological conditions: Parkinson's disease, multiple sclerosis, and HD. 23 This review identified four key categories for successful integrated care interventions: expert knowledge; multisectoral care coordination; care continuity; and a person-centered approach. Survey questions were informed by these categories and adapted for different sub-groups. Additionally, the key concept of “person-centered coordinated care”, developed by The National Voices, 30 was used to evaluate people's experiences of care.
The survey (template available as Supplementary Material) had five sections: (1) Experience with professionals and services; (2) Experience with coordinating care; (3) Support available to manage the condition; (4). Improvements needed; and (5) Personal characteristics. The number of questions varied depending on the respondent's path, with a person living with HD answering up to 60 questions. The survey could be paused and re-started from the stopping point at people's convenience. The survey path was tailored to the type of participant, in relation to the language and content. For example, carers survey asked questions either in relation to the person with HD or in relation to the carer; while the at risk/diagnosed survey focused on questions about the individual; former carers survey asked specific questions about support accessed after the person with HD passed away.
The survey was co-designed with patient and public involvement (PPI), which means people with lived experienced worked in partnership with the research team, carrying out the study “with” members of the public rather than “to/for/about” them. 31 Here we present some data regarding the co-design process, that will be further detailed in a separate manuscript. Firstly, two PPI representatives, from the Integrate-HD PPI group, gathered on an online workshop with the researcher (SBP) to discuss and draft the survey. The survey was then piloted with four individuals with different lived experience of HD, all members of HD voice (PPI group embedded in the Huntington's Disease Association England & Wales), through electronic correspondence. Changes were done in relation to: content (e.g., the individual that was at risk suggested to add options/questions around whether the individual wanted to engage with services, and whether any services had reached out to them proactively); language (e.g., changed participant categories from “diagnosed with HD” to “gene positive or with a clinical HD diagnosis” to confirm pre-symptomatic participants were welcomed to participate); and usability of the survey (e.g., usability and progress of the survey on electronic devices, that prompted changes in the setup, such as pause and re-start allowed, and instructions, such as to turn the screen horizontal in some questions). The final version of the Integrate-HD survey incorporated feedback from PPI, pilot participants, HD advocacy organizations (Huntington's Disease Association England & Wales and Genetic Alliance UK) and integrated care experts.
The anonymous survey required online consent before data collection. It included a mixture of closed and open questions across different domains, Likert-type scales, and free-text areas. This design ensured the instrument could distinguish differences over a sufficient range of response outcomes. Service users were asked to identify systems or organizations involved in their care, the main care provider and the county of residence and/or care received. Apart from consent and participant category, there were no mandatory questions, allowing respondents to skip irrelevant questions. At completion, participants were asked for their consent to be contacted in the future about other research opportunities and whether they wished to receive the results of the study in a lay report. Ethical approval was received by the University of Southampton (UK), number 77725.
Study population
The survey was open for completion from 28 February until 2 October 2023, inviting adults living in England who were:
at risk of HD, where at least one parent is diagnosed with HD, therefore their offspring has 50% chance of developing the disease; gene positive, where the person undergone genetic testing and has a CAG expansion mutation due to carrying the mutated gene (HTT); clinically diagnosed with HD, where motor symptom onset is clinically diagnosed by a specialist; informal caregivers and former informal caregivers that had taken care of someone living with HD in the past three years.
Exclusion criteria was set as people below 18 years old, not fluent in English, and/or people without capacity.
A non-probability “river” sampling method was used to recruit respondents online. River sampling involves inviting respondents to follow a link to a survey placed on a web page, email, or other location likely to be noticed by members of the target population. 32 This approach was chosen to advertise the study via community and public channels (as opposed to recruitment from specialist clinics), to also reach individuals not regularly engaged with health care services. This promoted the inclusion of people at different stages of HD (such as people at risk) and with different caring experiences (including for example, former informal caregivers).
Recruitment plan
The survey was advertised through social media using a study Instagram account (@integrate_hd), Facebook, X (previously Twitter), and Linked In. In addition, Huntington's Disease Association England & Wales and Genetic Alliance UK promoted the survey through their different online and electronic channels, via emails, newsletters, word-of-mouth (mainly through charity local advisors and PPI contributors), social media posts and research webinars. The survey was available online, using Qualtrics, and paper surveys were offered, but no copies were requested. The study was registered (ID NCT05828992) and publicly accessible via the platform ClinicalTrials.gov. 33
Data analysis
Surveys where 70% or more of the data was missing and had not been submitted, were deleted and not used in analysis. In accordance with our objective of documenting HD care in England, respondents who lived outside England were excluded from the analysis.
Descriptive statistics were used to explore and describe the outcomes using SPSS (version 29). Results from the quantitative analysis are presented via tabulation. Samples per analysis will vary because individuals only answered the questions they deemed relevant. Free-text responses were subjected to content analysis using NVivo (version 14, through cloud and tree maps). Results from the qualitative analysis are illustrated using quotations.
Results
Sample demographics
The Integrate-HD survey was available online for seven months, in an attempt to map all English counties. Surveys were considered valid and included for analysis where at least 30% was completed, otherwise it was considered a withdrawal and the data deleted. 153 surveys were included in the data analysis, 34 indicating a 40% withdrawal rate (Figure 1). Most of the surveys that were deleted were initiated by people who were gene positive or at risk of developing HD (73%), while the remaining left the category unanswered. Non-response/missing data is reported where applicable. Key respondent characteristics are summarized in Table 1.
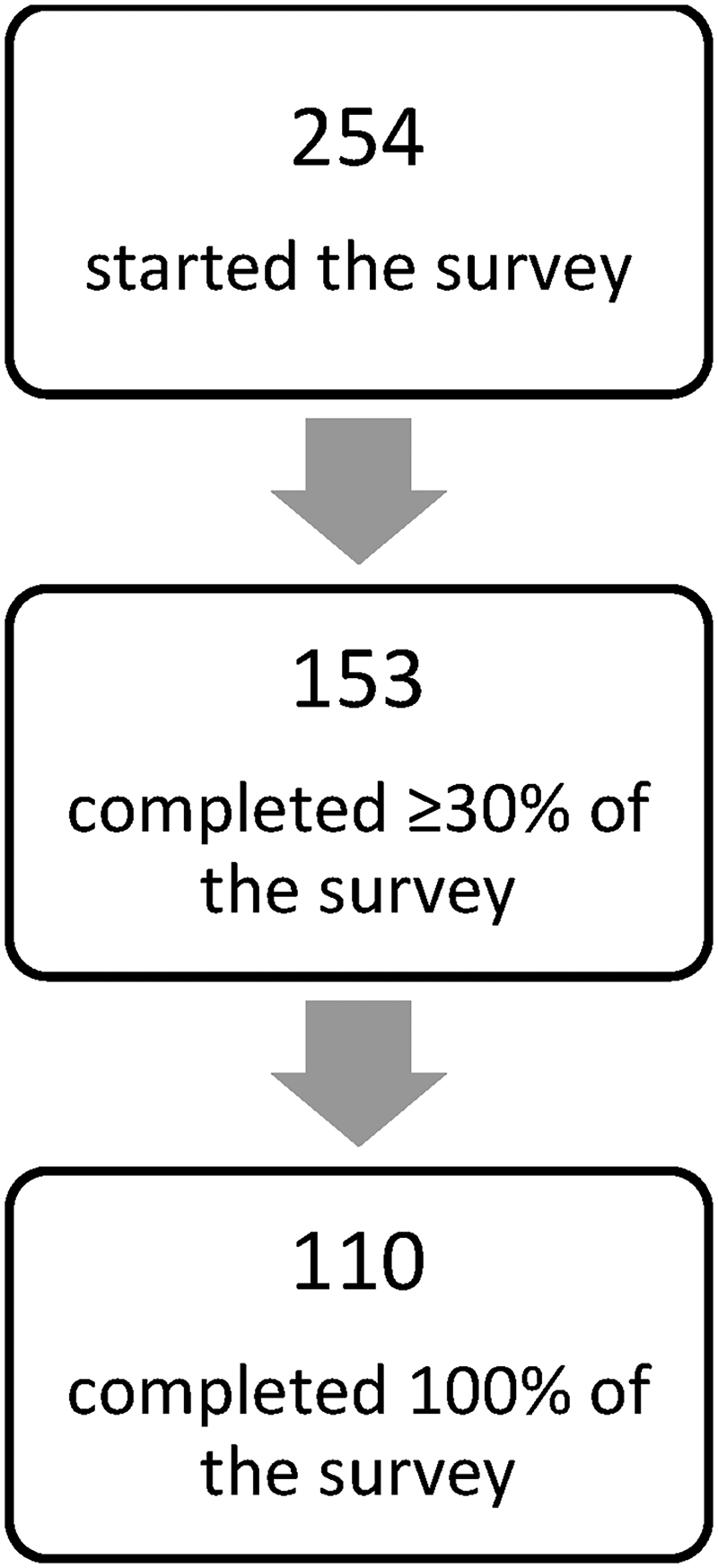
Integrate-HD flow diagram of participants.
Respondent characteristics.
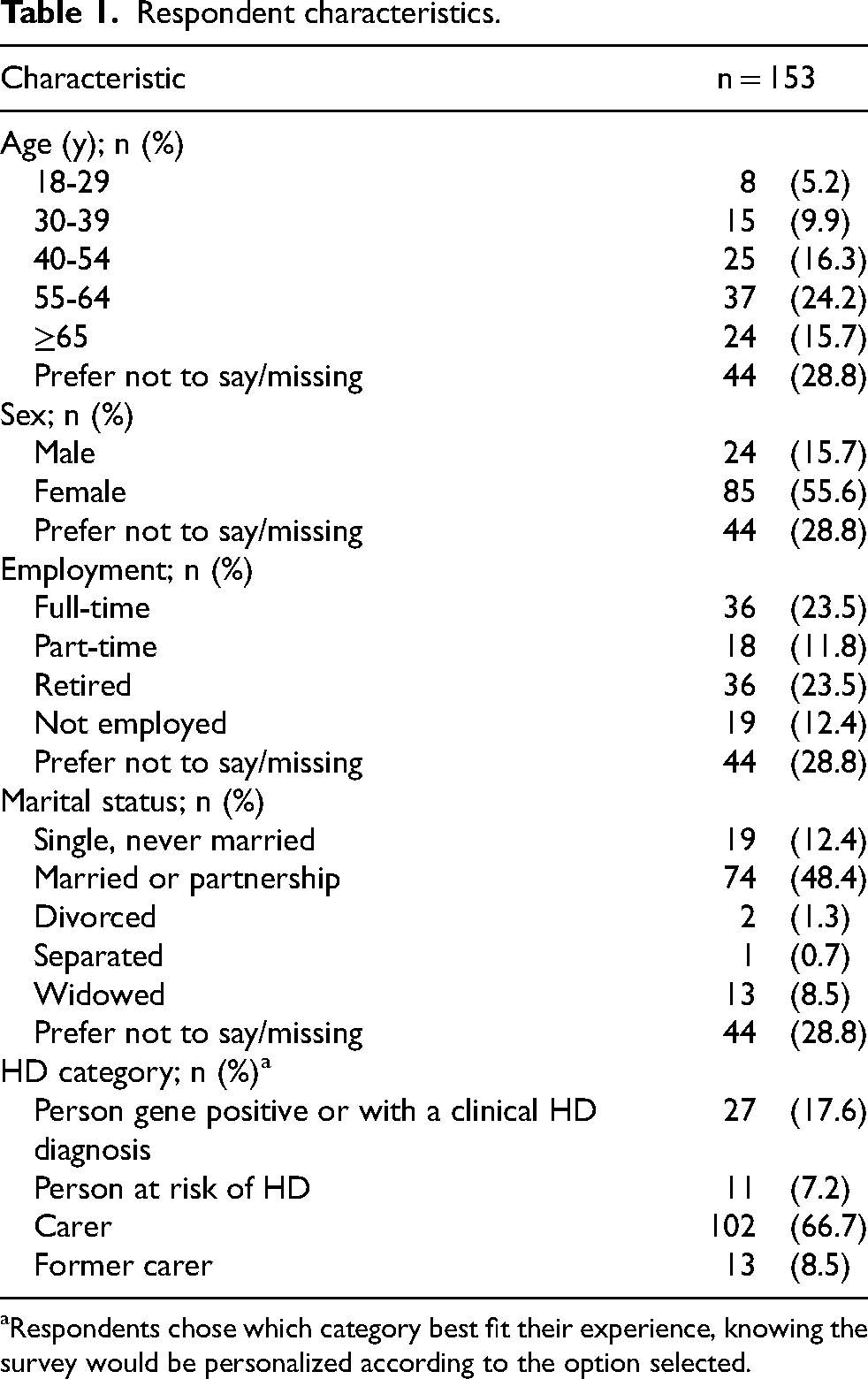
Respondents chose which category best fit their experience, knowing the survey would be personalized according to the option selected.
Our sample (n = 153) was constituted by nearly 67% carers from people with HD, 75% if we add former carers. This is similar to other surveys, namely in the United States of America (USA),35,36 where 64% to 79% of the sample were carers. The survey captured care experiences from 45 out of 48 counties in England, with responses per county ranging from one to 10.
Integrated care domains
Results in this section follow the four key domains from our previously completed systematic review 23 describing successful integrated care: Person-centered care, Expert knowledge, Coordination, and Continuity of care.
Person-centered care
Participants were asked to evaluate their experience of person-centered coordinated care using the National Voices definition: “I can plan my care with people who work together to understand me and my carer(s), allow me control, and bring together services to achieve the outcomes important to me”. 30 , p.3 Of the total sample, 74% (n = 113) provided rankings, while 26% did not evaluate their care. The results of this assessment are presented in Table 2. The findings reveal: 44% of respondents ranked their care equal or below 4, 20% ranked their care neutral, and 35% of respondents ranked their care equal or above 6.
Person-centered integrated care ranking. a
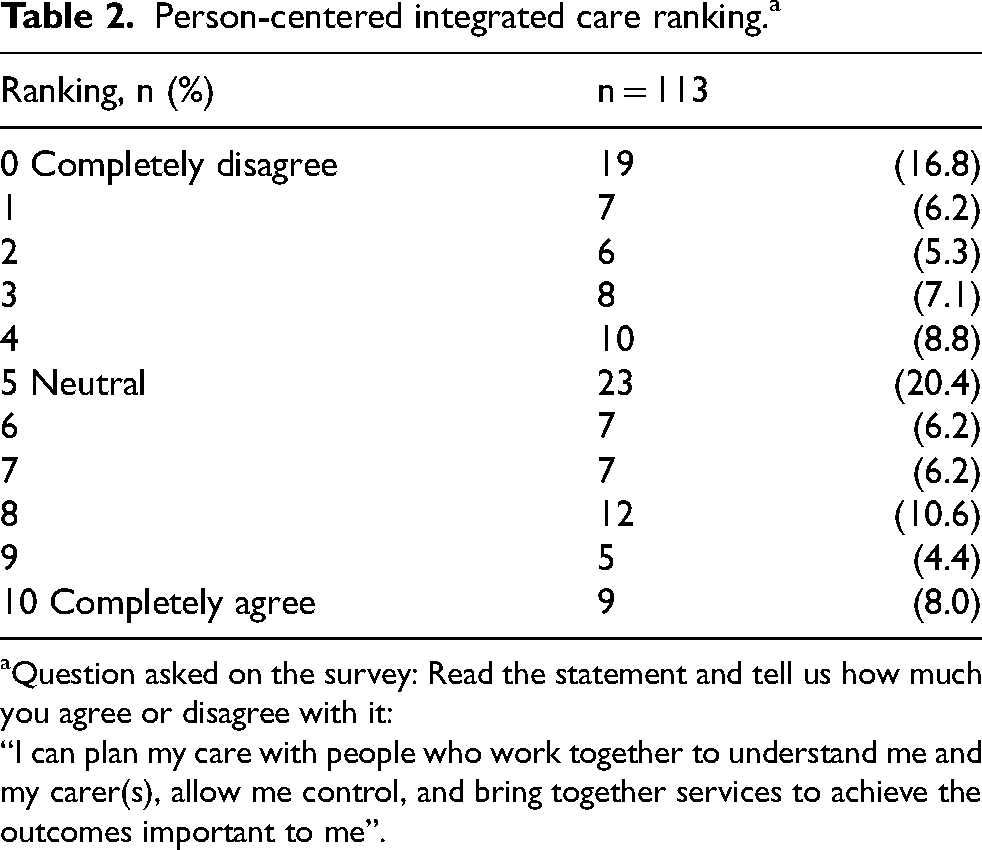
Question asked on the survey: Read the statement and tell us how much you agree or disagree with it:
“I can plan my care with people who work together to understand me and my carer(s), allow me control, and bring together services to achieve the outcomes important to me”.
Sub-group analysis of care experience ratings revealed notable variation among different cohorts (see Supplementary Figure 1). Carers reported the lowest satisfaction with their care experience yielding a mean rating of 4.0. Individuals at risk, gene positive and those clinically diagnosed with HD had a more heterogeneous experience resulting in a neutral mean rating of 5.2. In contrast, former carers expressed the highest satisfaction, with a mean rating of 6.4, surpassing all other subgroups.
Per county, sub-group analysis suggested regional variation when assessing person-centered coordinated care and satisfaction with care needs (Supplementary Table 1), indicating access to resources and quality of care may differ depending on geographical location within the country. Participant's quotes are provided to illustrate regional variation. These findings will be further explored in the next stages of the research project. “I am fortunate enough to be able to have a really excellent care plan by the team in [County A] and feel really positive to live within a region with such excellent healthcare almost on my doorstep”. Person gene positive/HD diagnosis “I am more physically affected by HD than cognitively. I live in a very rural area [County B] and it is difficult to access care not coming to my home”. Person gene positive/HD diagnosis “I have found it very difficult to access coordinated care for my mother, we had a good team in (…) but when she moved to (…) it was very difficult”. Person at risk of HD
Participants evaluated their satisfaction with how health and social care services met the needs of people living with HD. Nearly half the sample (48% n = 63) were somewhat or extremely dissatisfied; 28% of the sample were somewhat or extremely satisfied; and 24% were neutral. Carers and former carers were specifically asked how their own care needs were met by health and social care services: 57% (n = 41) were somewhat or extremely dissatisfied; 14% were somewhat or extremely satisfied; and 29% neither satisfied nor dissatisfied. More than half the study sample (65%, n = 70) reported being involved in HD care decision-making as much as they desired, while 17% reported not being involved to the extent they wished. The remaining 18% were involved to some degree, albeit not to their preferred level.
Concerning accessing care supporting people living with HD, 65% (n = 80) of respondents considered access somewhat (25%) or extremely difficult (40%). Carers reported particular challenges in accessing care that supports them, with 46% saying it is extremely difficult to access care and 21% finding it somewhat difficult. About 2% of the sample considered access to care extremely easy.
Expert knowledge
Respondents were presented with a list of 25 multi-sectoral professionals and resources (including council services, voluntary sector organizations, community groups, and police) and asked to identify up to three primary sources involved in supporting HD management. The most frequently selected resources were: neurologists (n = 41), primary care practitioners (GPs n = 40), social workers (n = 37) and HD charities (n = 35).
For each professional identified, respondents were asked to evaluate their perceived knowledge of HD. Figure 2 illustrates the comparison between the main professionals/resources identified as being involved in HD care and how knowledgeable respondents perceived them to be in HD-specific matters.
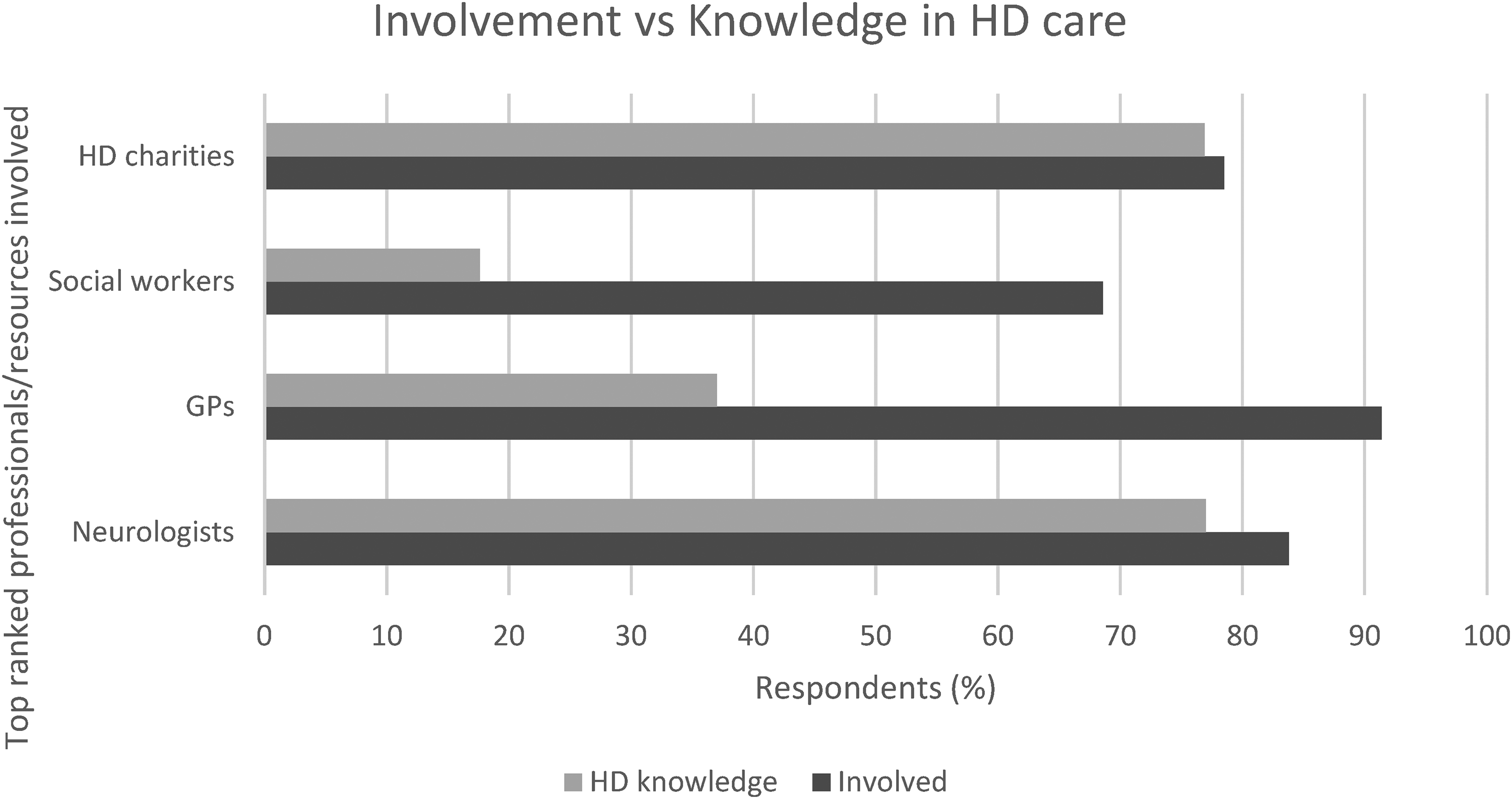
Top ranked professionals/resources involvement vs HD knowledge, as perceived by the Integrate-HD survey participants.
The data revealed significant discrepancies between involvement and perceived knowledge for certain professionals, particularly GPs and social workers: 69% (n = 35) of the respondents confirmed that social workers were involved in HD management, but only 18% considered them knowledgeable. 91% (n = 74) of the respondents confirmed that GPs were involved, but only 37% considered them knowledgeable. In contrast, neurologists and HD charities demonstrated a closer alignment between their involvement and perceived HD knowledge.
Coordination
We asked how important it was to have a care coordinator (understood in the survey as a professional who links different services and professionals to meet their HD care needs). Although 90% of respondents (n = 112) stated it was very important or extremely important to have a care coordinator, only 19% of people indicated that they had a care coordinator in HD; the presence of a care coordinator was identified in only 19 English counties. The role of care coordinator was mainly taken by nurse specialists (48%), consultants (19%, e.g., neurologists and neuropsychiatrists) and social care workers (14%).
Among those with a care coordinator, 81% reported being somewhat or extremely satisfied with their services. The presence of a care coordinator correlated with better person-centered care rankings (Supplementary Figure 2). In fact, 21% of people without a care coordinator ranked a score of 0, while no participants with a care coordinator reported this low score. Conversely, 38% of people with a care coordinator available gave high scores of 8 and above.
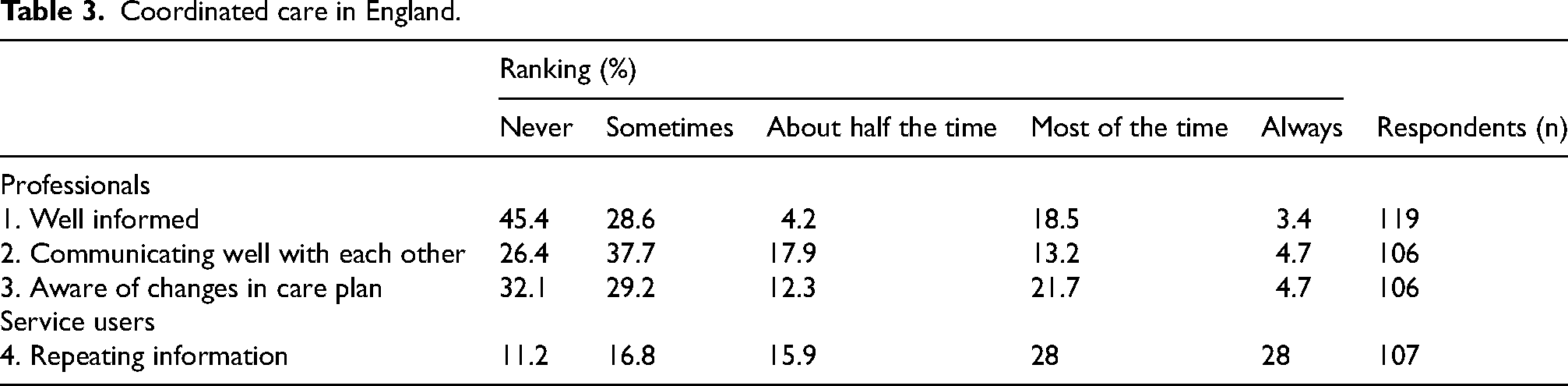
To evaluate the quality of care coordination in England from the perspective of service users, respondents were asked about their experiences with various aspects of professional care (Table 3). Specifically, they were queried on how often they perceived that different care professionals were: well informed about what happened in other consultations, aware of changes in their care plan, communicated well between themselves about care needs; and, how often respondents needed to repeat information to different professionals involved in their care. Care coordination aspects (points 1–3) consistently received low ratings, with most respondents selecting “never” or “sometimes”. Conversely, the need to repeat information to different professionals (point 4) was reported as more frequent, with 56% of respondents indicating this occurred “most of the time” or “always”.
Coordinated care in England.
Continuity
To assess continuity of care, we focused the survey on relationship continuity,37,38 examining participant's views on the importance of discussing their HD care with the same professional at every appointment, and, in the previous 2 years, how often they saw that same professional at every appointment.
Regarding GPs, 54% (n = 120) said it was extremely important to see the same GP at every appointment, yet only 10% consistently did so; 32% of the sample stated never seeing the same GP.
Concerning neurologists, it is important to note access figures; 74% of the sample (n = 126) stated having access to a neurologist through the National Health Service (NHS). Of these, 60% said it was extremely important to have access to the same neurologist at every appointment to discuss HD care, and 50% reported seeing the same consultant at every appointment.
Only 34% of the sample (n = 127) stated having access to a specialist nurse. Of these, 42% said it was extremely important to have access to the same specialist nurse at every appointment, but only 21% did so.
We asked participants how important it was to them to see a professional regularly about HD. Overall, 78% of the sample (n = 125) said it was extremely or very important, but 31% did not regularly see a professional. Approximately a quarter (24%) stated seeing a professional every year about HD. When we asked the sub-group of people diagnosed with HD (n = 36) about their preferred consultation frequency, 39% of people indicated a preference to see a professional every 1–3 months or 4–6 months, while 33% preferred an annual review.
Although more than half the people (56%, n = 62) indicated they probably or definitely knew who to contact for HD care questions, only 27% were satisfied with the response time.
Unmet care needs: Setting priorities
Respondents provided free-text answers on their most important perceived care needs and were asked to identify their top three care needs. Data was imported to NVivo version 14 and a word cloud data query was generated (Supplementary Figure 3).
Mental health needs were mentioned most frequently, typically as “mental/psychiatric” needs, in relation to the person diagnosed with HD (presenting behavioral symptoms), and to caregiver's own unmet mental health needs, including caregiving burden and emotional distress. Family needs were mentioned in relation to HD being a hereditary condition, emphasizing it as a family disease rather than an individual condition. Participants requested counselling for their children and more easily accessible respite or caring “offload”, that would give caregivers a bit of time to manage many other family responsibilities. Financial support was often mentioned, with bureaucracy cited as an obstacle to much needed support and forms ill-suited for completion by people who are cognitively impaired and/or mentally and physically exhausted. Social support needs varied including home support with trained paid carers, house-hold chores assistance, access to equipment aids for home management, and appropriate long-term care settings for younger people with complex needs.
In response to the question “In your own words, please list the top three things you think need to improve so that patients’ and caregivers’ needs are better taken care of”, participants provided several areas for improvement; these were themed using a tree map in NVivo. Replies centered around the need to improve support, care and access. Areas for improvement are listed below (in no specific order of importance) and illustrated with participant's quotes:
1. “Very difficult to organise an appointment with services, when they eventually do come out its all talk but not very much actually gets done help like equipment and aids to support and make things easier to support caring for someone are near to none. No social workers to advise and get financial support and advice”. Carer “I think because HD is unique in its genetic risk, counselling needs to be specific to HD. I felt grief for my husband, but also grief for the life HD affected, even before he was diagnosed, the effect on the family of mood swings & anger outbursts, for example’. Former carer
In addition, many former carers referred to the need for support to continue after the death of the person with HD. They mentioned the need for counselling, a friendly ear, with a need to do so with a person that understands HD. They also needed support to navigate the transition from full-time carer with no time to “all the time in the world”.
2. “One person with HD has passed away, but there are other family members who will soon start to require support. HD is a constant in our lives rather than something that comes to an end. We are currently in a small period of respite until it all starts again. So at this point we just want to stop and try to live some life for a while until we have to start up with hospital appointments and medications and doctors’ conflicting advice and social workers…”. Former carer
“My needs will definitely change as I get older. I also will have needs related to being a carer as my sister also has HD and if she gets sick before me, I may have to help with caring”. Person gene positive/HD diagnosis
3. “All care has been difficult to access, mostly medical and social care. Social workers have 2 appointments here, then close the case if you're not in immediate danger, disregarding the progression of HD or working proactively to help mitigate future problems. The long wait times trying to call the GP, hospital, pharmacy and district nurse is a big barrier for accessing information/appointments. I've been left on hold for 30 + minutes with NHS calls and in most cases don't get through to anyone the first time calling. This is very frustrating when trying to find out information on medicine or scheduling urgent appointments”. Person at risk of HD
4.
“Care plan was written with mental health services and adult social care who had no understanding of HD. Therefore it was always flawed anyway”. Former partner
5. “Until the introduction of our HD Neuro Nurse, who visits us bi-annually and is available to answer questions by email in the interim, we struggled. We were only given this contact when I, as the carer, had a total meltdown and couldn't cope. She has referred us to other agencies as required and visits us whether there is an emergency or not. It was the HDA who got us in contact with her, not the NHS, although she works in conjunction with the neurologist. We believe this position is quite rare in the NHS but is invaluable.” Carer
“There doesn't seem to be any joined up thinking or best practice stating what care we can expect. If there is, we haven't heard of it. It is up to me to initiate anything we need. Waiting lists are an issue here of course; it may be that things are happening behind the scenes (e.g., referrals) but just very slowly. I just don't feel there is a team we can reach out to for support”. Carer
6. “I guess the gaps lies between where health and social care join. This is where the lack of collaborative working is, especially when I think about assessments surrounding care and individual needs being met. Recently we failed to receive CHC [continuing health care] funding and I had to coordinate a lot of the assessment with specific health and social care practitioners”. Carer
“I had a lot of trouble convincing social care that my father was a danger to himself and others. People fall through the cracks all the time. My mind wanders to the recent case of the man living with HD who went missing early in 2023 and his body was recently found in (…) river. This could have easily been my father when he went for his wanders whilst confused. This happened because someone wasn't looking out for a vulnerable adult. There are huge holes in the care of people with HD and everyone who has the disease knows they will be completely reliant on others to keep them safe in the future”. Person gene positive/HD diagnosis
7. “When a care home placement was needed then things became difficult because the HD patient was only 39 years old and most care homes that take HD patients, only take people over the age of 55 or 60”. Former partner
8.
“Many people living with HD also take part in follow-ups for research purposes. These can (not always) reveal incidental findings or flag issues which then get related back to clinical care team. So although I only see my specialist once a year; I interact with the clinic 2 or 3 times a year due to research. I think this is important for my well-being and I feel less alone and disconnected because of it.” Person gene positive/HD diagnosis
Discussion
To our knowledge, this study is the largest survey undertaken in HD in England. Comparison with previous HD surveys in England was not undertaken as the only published UK datasets for HD were from 2006/2007, and only recruited carers.17,18 Therefore, Integrate-HD fills an important gap in the literature, with a user-driven approach that explored health and care experiences by service users living with HD in England. Primarily, our findings show that people and families living with HD in England experience fragmented care, regional variation (postcode lottery) and have numerous complex unmet needs. Improvements are particularly urgent around social and mental health support. Our participants reported high difficulty in accessing care, but those cared by an expert team with a knowledgeable care coordinator reported markedly improved care experience. Our findings have substantial implications for practice, policy and research in HD.
Practice implications
Integrate-HD identifies serious problems with the current standard of care, calling for improved multi-sectoral integration. The top professionals/resources involved, identified by participants (GPs, neurologists, social workers and HD charities), represent the multi-sectoral nature of HD care. Nevertheless, the imbalance between professionals’ involvement and perceived HD knowledge highlights obstacles in receiving person-centered care. In other hand, Anderson's study 35 in the USA, found that professionals were rated as providing a good care experience, particularly HD specialists, adding to the evidence that access to specialist care improves people's experiences with care. Our survey participants also emphasized the importance of accessing knowledgeable staff, but not without difficulties. Our participants’ experiences match the reported by professionals in the UK HD specialist services overview, 39 highlighting limited access to mental health support and HD specialist nurses. In addition, researchers found lack of willingness from professionals to manage patients and make referrals. This underscores the importance placed on a care coordinator.
Although only 19% of our respondents identified access to a care coordinator, those that did, reported higher rankings of person-centered care, revealing a much better experience with living with HD. Care coordinators, in our study, were mainly recognized in the role of HD nurse specialists. Although HD is a condition that requires expertise to be well-treated, it lags when compared to other neurodegenerative diseases - while in Integrate-HD only 34% of people had access to a specialist nurse, in multiple sclerosis and Parkinson's disease, figures rise to 78/79%. 40 However, there are common obstacles among neurodegenerative diseases, such as difficulties in the access of community services and referrals, especially when care relies on a professional without a cross-sectoral boundaries role, such as a neurologist or a GP.40,41 This suggests that a better solution may be a care coordinator with a cross-boundaries role, someone to navigate the multi-sectoral “HD care web”.
Policy implications
HD remains an incurable disease with symptomatic and holistic disease management; 42 this makes it more relevant that professionals involved are knowledgeable about the condition. Rare diseases policies21,43 recognize the need to improve access to specialist care, treatments and drugs. However, there is currently a lack of pragmatic treatment guidelines, such as NICE guidelines, accessible to varied professionals involved in HD care. Our results highlight the detrimental consequences of action plans taken by staff with knowledge gaps. Namely, carers reported inadequate assessments of people's mental capacity by social care professionals, resulting in undue cessation of support. The development and implementation of HD guidelines has the potential to improve care for individuals and families with HD, mirroring the positive impact seen in other conditions.44,45
Despite the 24-year gap, similar to Bernard 40 and colleagues’ survey of primary care trusts in England to explore services for people with long-term neurological conditions, our data suggests regional variations in care, akin to a postcode lottery. Based on the recent Marmot review, 46 we believe that care inequalities have worsened, particularly for the most vulnerable, and people will only feel a wider access gap post-pandemic. Particularly as, contrary to the advice on Marmot's review to better fund and action the social determinants of health, England's seen their total public expenditure per capita on adult social care considerably lower than in other UK countries. In Integrate-HD the underserved social needs are particularly striking at carer level, with high dissatisfaction, coupled with financial struggle. Informal carers are the main workforce supporting people with high levels of dependence. However, the King's Fund 47 reports that fewer carers now receive direct support compared to a decade ago. Sustaining carers becomes crucial considering the lack of suitable care settings for people living with HD as the disease progresses. Carers require formal recognition as part of the workforce, including financial remuneration. 48 In Sweden for example carers have a contractual employment between the carer and the municipality to provide assistance. 49 We propose implementing similar policies in England to identify, assess and financially reward carers, thereby alleviating financial strain.
Research implications
Our data indicates people have a better care experience when a knowledgeable care coordinator is involved, therefore further research should test the cost-effectiveness of an HD care coordinator. While a “one-size-fits-all approach” is unfeasible, there are numerous common approaches which, if adopted, would significantly enhance quality of care. 50 Future research should focus on developing complex interventions to address common needs across similar conditions, and evaluate not only cost-effectiveness, but efficacy at user-level. Subsequent phases of the Integrate-HD project aim to do this, identifying core person-centered outcomes for people living with HD and characterizing an integrated care model that meets their complex needs. This will form the basis of future pilots across similar conditions.
Limitations
Despite maintaining rigor, our study has several limitations. The survey was advertised mainly via charitable resources and social media platforms, potentially resulting in selection bias, with higher participation from people accessing charity and social media resources and those reporting poor experiences, rather than those with positive experiences. Furthermore, there was a high non completion rate among people at risk of HD and gene positive (40%), which may indicate the survey was insufficiently fine-tunned to capture these groups’ needs and experiences. The possibility of nonresponse bias may have affected the results. At county level the sample was too small to be representative, but important inferences could still be drawn nationally.
Conclusions
Findings from this study are important and novel highlighting the national standard of current HD care, allowing us to track progress and set the direction for future intervention development. In the face of the current health and care reforms, the Integrate-HD survey provides a baseline in the first year of Integrated Care Systems becoming mandatory in England. This is important for monitoring future progress towards integration in neurological conditions such as HD.
Service provision for people living with long-term neurological conditions remains an under-researched area, despite its significant impact on health and care. This paper offers a valuable and necessary contribution for policymakers, commissioners and service leads in benchmarking integrated person-care from the perspective of service users. Based on this report, we propose some interventions that may improve care experiences: provision of support from a knowledgeable and cross-boundaries care coordinator; identifying, training and compensating family carers; improving access to specialist care; and developing and implementing HD care guidelines. Furthermore, this study underscores a crucial point: given the identified areas for improvement and unmet needs of people living with HD, future studies must develop a complex integrated care program addressed and assessed from a person-centered perspective. Without knowing the difference our integrated care interventions have at the individual level, we cannot deem a reform successful.
Supplemental Material
sj-docx-1-hun-10.1177_18796397241288449 - Supplemental material for Are people living with Huntington's disease experiencing person-centered integrated care?
Supplemental material, sj-docx-1-hun-10.1177_18796397241288449 for Are people living with Huntington's disease experiencing person-centered integrated care? by Sandra Bartolomeu Pires, Dorit Kunkel, Nicholas Goodwin, Sally Dace, David Culliford, Christopher Kipps and Mari Carmen Portillo in Journal of Huntington's Disease
Supplemental Material
sj-docx-2-hun-10.1177_18796397241288449 - Supplemental material for Are people living with Huntington's disease experiencing person-centered integrated care?
Supplemental material, sj-docx-2-hun-10.1177_18796397241288449 for Are people living with Huntington's disease experiencing person-centered integrated care? by Sandra Bartolomeu Pires, Dorit Kunkel, Nicholas Goodwin, Sally Dace, David Culliford, Christopher Kipps and Mari Carmen Portillo in Journal of Huntington's Disease
Footnotes
Acknowledgments
The authors express their gratefulness to the patient and public representatives living with long-term neurological conditions who contributed to this work. The authors thank the National Institute for Health and Care Research Applied Research Collaborations Wessex (NIHR ARC Wessex) for providing funding. The authors also convey their sincere appreciation to all the third sector entities that supported recruitment for Integrate-HD, specifically the Huntington's Disease Association England & Wales, Genetics Alliance UK and The Neurological Alliance.
Funding
This research was conducted as part of the Integrate-HD research project, a mixed-methods study aiming to develop an integrated care model that meets the needs of people living with Huntington's Disease, funded by the National Institute for Health and Care Research Applied Research Collaborations Wessex (Award: NIHR-INF-1701). The views expressed in this publication are those of the authors and not necessarily those of the National Institute for Health and Care Research or the Department of Health and Social Care. The funder had no role in the design of the study, data collection, analysis, or writing of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.