
Abstract
Background
In most Huntington's disease expanded gene carriers (HDEGC), losing work capacity is the first sign of functional decline. Cognitive deterioration, motor dysfunction, and psychiatric disturbances are associated with or predict work outcomes in HD. The role of profession-specific requirements, however, has not been investigated.
Objective
This study examines the relationship between work outcomes, clinical characteristics, burnout, and profession-specific requirements in HDEGC. We hypothesize that burnout-like symptoms are associated with mild apathy and that profession-specific requirements influence clinical characteristics affecting work capacity in HD.
Methods
A cohort of 117 HDEGC (CAG repeat ≥36) participated in the “HD-work” study at Leiden University Medical Center. Participants were 18–67 years old, either, worked at baseline, or had lost their job within two years. The Unified Huntington's Disease Rating Scale assessed motor abilities, global functioning, and cognition. The HD-work questionnaire and the ‘Utrecht Burn Out Scale’ assessed work problems and burnout. Statistical methods included descriptive statistics, Pearson correlations, Cronbachs alpha, t-tests, and logistic regressions.
Results
Burnout-like symptoms did not differ between those with full and reduced working capacity and were not more prevalent in HD than in the general Dutch population. No significant effect was found between work outcomes and profession-specific requirements, even when adjusted for clinical characteristics.
Conclusions
Our study suggests that profession-specific requirements do not significantly impact work ability among individuals with HD in early phases of HD. Workplace adjustments should be tailored to individual preferences rather than profession-specific demands. Burnout-like symptoms did not affect work capacity or relate to apathy.
Introduction
An essential early sign of functional decline in Huntington's disease (HD) is losing the ability to work. In the majority of cases (61% to 65%), it is even the first sign of functional decline in carriers of HD-expanded gene mutation. 1 Loss of work causes financial and emotional distress, consequently decreasing quality of life.2,3 Moreover, maintaining one's occupation affects psychological well-being positively. 4 Over the years, several studies reported determinants of the loss of work capacity, resulting in a somewhat heterogeneous list of clinical characteristics. 5 The loss of work capacity has been associated with or predicted by motor dysfunction, psychiatric behavior such as apathy, and cognitive deficits in attention and executive control. 5 Where mild apathy seems to play a more prominent role in the early stages of the disease, motor dysfunction and cognitive deterioration seem to have an increasing effect in later disease stages.5,6
Apathy is characterized by a lack of motivation, initiative, and interest in activities that were previously found engaging or important. 7 However, mild apathy is a somewhat vague and elusive construct especially, in working and premanifest individuals. Clinically it might be more akin to a construct like exhaustion we see in burn out, where it manifests as a feeling of being drained and unable to cope with the demands of work or daily life. 8 Burnout and apathy both involve emotional exhaustion and reduced motivation, but burnout specifically includes depersonalization and a sense of reduced personal accomplishment. This makes studying burnout symptoms in HD relevant, as both conditions may similarly impact one's work capacity. Additionally, chronic diseases are often associated with higher prevalence of burnout and burnout-like symptoms, making it a relevant variable in this study. 9 Therefore we aim to study the potential role of burnout symptoms in HD.
Another work-related variable that might influence work-outcome in HD is impact of profession-specific requirements in combination with clinical characteristics of the disease on the capability to work. Several researchers have suggested an added influence of these requirements on work outcomes in HD.6,10,11 Profession-specific requirements refer to the demands an individual needs to meet to perform their professional duties and responsibilities. For example, while motor symptoms may significantly impact individuals with professions requiring physical activity, cognitive symptoms may be more detrimental for those who need to multitask in more administrative functions.
Therefore, we hypothesize that there is an early influence of burnout-like symptoms in HD that are associated with mild apathy complaints. Additionally, we anticipate an added value of profession-specific requirements as a confounding variable that will partially influence the aforementioned heterogeneity of clinical characteristics influencing work in HD. This study aims to identify and further disentangle the factors influencing work in HD, providing valuable insights for patients, caregivers, employers and healthcare professionals to support work participation in HD.
Methods
Participants
One hundred-and-seventeen HD expanded gene carriers participated in HD-work, a longitudinal observational study conducted at the Leiden University Medical Center in the Netherlands. Participants were all aged between 18 and 67 years, had a confirmed CAG repeat length ≥36 in the HTT gene, and were either currently employed in any capacity or had experienced job loss within the previous two years. The two years are based on the WIA (Work and Income according to Labour Capacity Act) which is a Dutch law that governs how individuals with work incapacity are supported in their income and rehabilitation back into the workforce. The HD-Work study was approved on 14 March 2019 by the Medische Ethiek Toetsing Commissie – Leiden, Den Haag, Delft (METC-LDD) (reference: NL67070.058.18). This study is cross-sectional, using the baseline data only and involves multiple exploratory analyses.
Demographics and clinical characteristics
Information on the participant's age and sex was obtained. Next, we used the Unified Huntington's Disease Ratings Scale–Total Motor Score (UHDRS-TMS), a physician-administered semi-quantitative neurological exam, to evaluate motor impairments in HD. In this scale, higher scores indicate more motor impairments, and scores range from 0 to 124. We also used part of the Total Functioning Capacity scale (TFC) of the UHDRS to determine the overall functional abilities of participants: lower scores indicate less functional capacity, and scores range from 0 to 13. This scale consists of five questions, focusing on occupation, finances, household chores, activities of daily living, and care level. We used the occupation item to determine whether someone has a normal or reduced working capacity. We used the Diagnostic Confidence Level (DCL) of the UHDRS to determine whether a participant has unequivocal HD signs (DCL = 4; manifest) or does not have signs that are unmistakably due to HD (DCL < 4; premanifest). Apathy was measured with the Psychiatric Behavioral Assessment -short version, a semi-structured interview conducted by trained healthcare professionals that focuses on psychiatric problems and behavioral symptoms caused by HD. 12 We have not included other psychiatric variables as previous research shows little to no influence on work related outcomes in a relatively early phase of HD.5,6 Finally, we use the CAG – age product score (CAP-score) as a measure of disease progression. 13
Cognitive assessments
Cognitive ability was measured with the symbol digits modalities test (SDMT), 14 the Stroop word reading test (SWRT), the Stroop color naming test (SCNT), the Stroop interference test (SIT), 15 the verbal letter fluency test (VLFT), 16 the verbal category fluency test (VCFT), 16 and the trail making test part A and B (TMT-A & B). 17 These tests were used as measures of attention and processing speed, psychomotor speed, mental flexibility, inhibition control, and the ability to shift attention, respectively. All cognitive tests were administered by trained neuropsychologists.
HD-work and burnout questionnaires
The HD-work questionnaire combined questions derived from the Nederlandse Arbeids Enquete (NAE; Dutch national work questionnaire) 18 and the Huntington's Disease Workforce scale (HDWF). 19 The NAE items focus on variables surrounding work circumstances, for instance, the number of working hours, the type of employment, or whether any changes as a result of external factors have occurred. In this study, we used it primarily in combination with the TFC to determine whether someone was working at normal capacity. The HDWF is a scale specifically constructed to determine work problems in HD and was found to show differences between manifest and premanifest participants. 19 Participants are asked to rate statements on a 7-point Likert scale from “not at all like me” to “very much like me”. Statements are, for example, “My handwriting is as good now as it ever was” and “I make decisions quickly”. In this study, we have translated the original 20 items from the HDWF into Dutch and added 5 items for additional insights into participants’ work capacity.
Profession-specific requirements were classified based on the tasks and responsibilities of each participant's occupation. Researchers KZ and MF reviewed job descriptions, the added HDWF questionnaire statements on necessary abilities, and questions from the NAE section of the HD-work questionnaire (e.g., “Do you work behind a desk?”) in order to fully determine the profession-specific requirements of each individual participant. Both researchers had to reach an agreement on the classification. They then classified each subject accordingly. An overview of the reported professions and their distribution by mental or physical profession type is given in the Appendix. Burnout levels were determined using the ‘Utrechtse Burnout Scale (UBOS)’, 20 a self-reporting assessment with 22 questions assessing emotional exhaustion, depersonalization, and personal accomplishment on a 7-point Likert scale. To compare the prevalence of burnout-like symptoms between our cohort and the Dutch population in general, we used that part of the UBOS, which is also incorporated in the NAE. The NAE uses five items of the UBOS items to measure burnout symptoms in the Dutch population. However, these separate items are not very specific and represent burnout-like symptoms rather than burnout.
Statistical analysis
We used R version 4.2.2 for statistical analyses. The sample size of 117 participants was determined based on feasibility within our clinical setting and the aim to ensure a diverse representation of individuals with HD across various stages and occupational backgrounds. Specific sample size calculations or effect size estimations were not performed. Descriptive statistics were used to summarize the overall characteristics of the sample. Pearson correlations were performed to determine associations between work outcomes. Two-tailed t-tests were used to determine the differences in demographic information, clinical characteristics, burnout/burnout-like symptoms, and work outcomes between people with full and limited working capacity. To address the reliability as a measure, the internal consistency of the HD-work questionnaire and all derived scales was evaluated using Cronbach's alpha, calculated with the psych package in R. An alpha value of 0.7 or higher is considered acceptable for psychometric scales. 21 Binary logistic regressions were used to study the effect of profession-specific requirements, clinical characteristics of HD, and their influence on work outcomes. For a visualization of the investigated associations, see Figure 1. The statistical significance level for all analyses was set at p < 0.05. The variance inflation factor (VIF) was used to assess multicollinearity, and models with VIF > 10 were excluded.
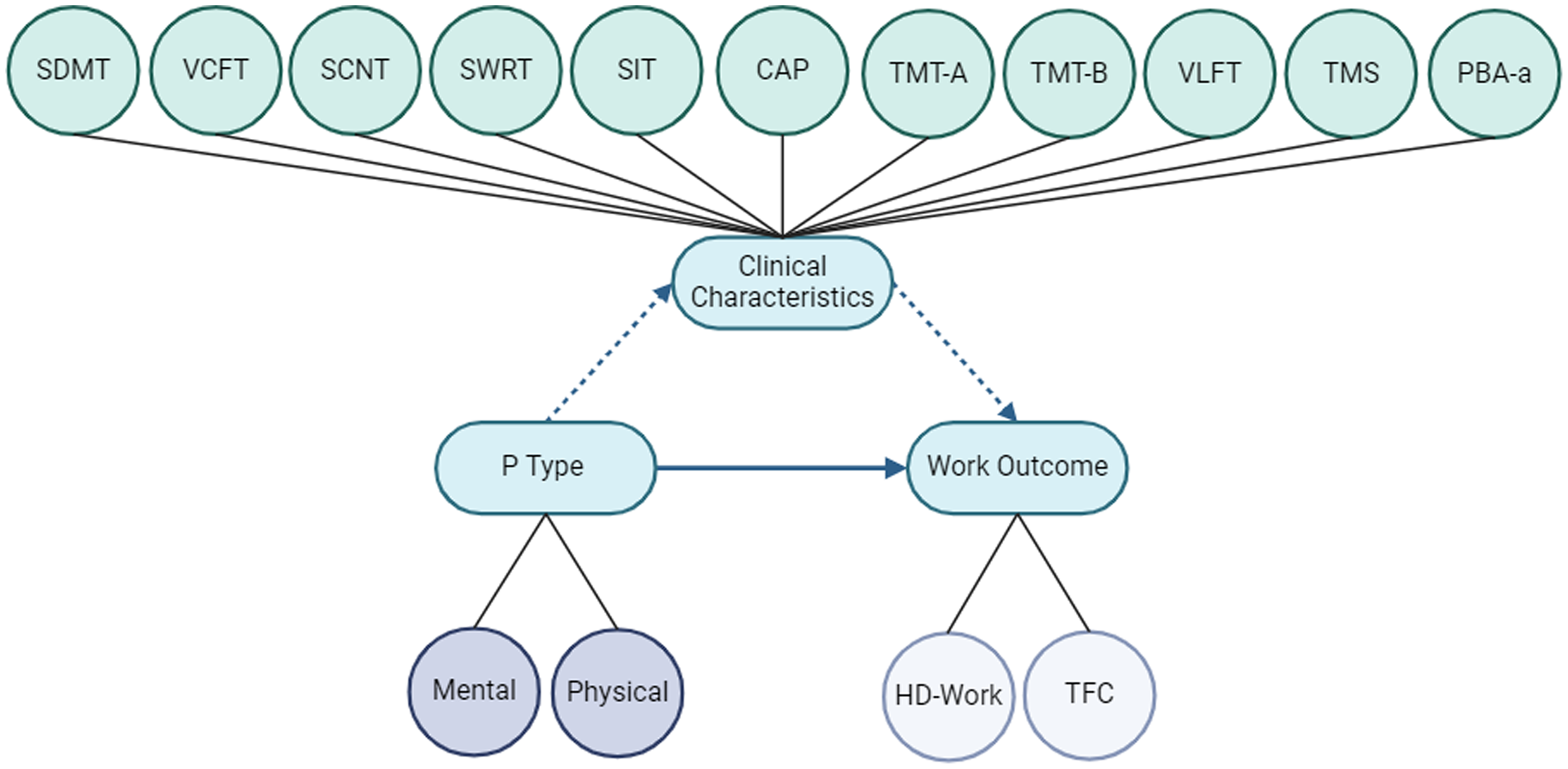
The investigated associations between profession type, work outcomes, and the influence of clinical characteristics. In blue are the main investigated topics. The first association (undashed arrow) that is studied is the influence of profession type (mental or physical) on work outcomes. Secondly, the added effect of clinical predictors (above) is evaluated (dashed arrows). PBA-a: Psychiatric Behaviors Assessment – Apathy; P Type: Profession Type; SCNT: Stroop Color Naming Test; SDMT: Symbol Digits Modalities Test; SIT: Stroop Interference Test; SWRT: Stroop Word Reading Test; TFC: Total Functioning Capacity; TMS: Total Motor Score; TMT A & B: Trail Making Test A & B; VCFT: Verbal Category Fluency Test; VLFT: Verbal Letter Fluency Test.
Results
In our sample, most participants were premanifest (n = 79), had a permanent contract (n = 66), and were part-time employed, i.e., worked less than 36 h a week (n = 55). This, however, does not reflect their working capacity (Table 1).
Demographics and employment characteristics of HD-work.
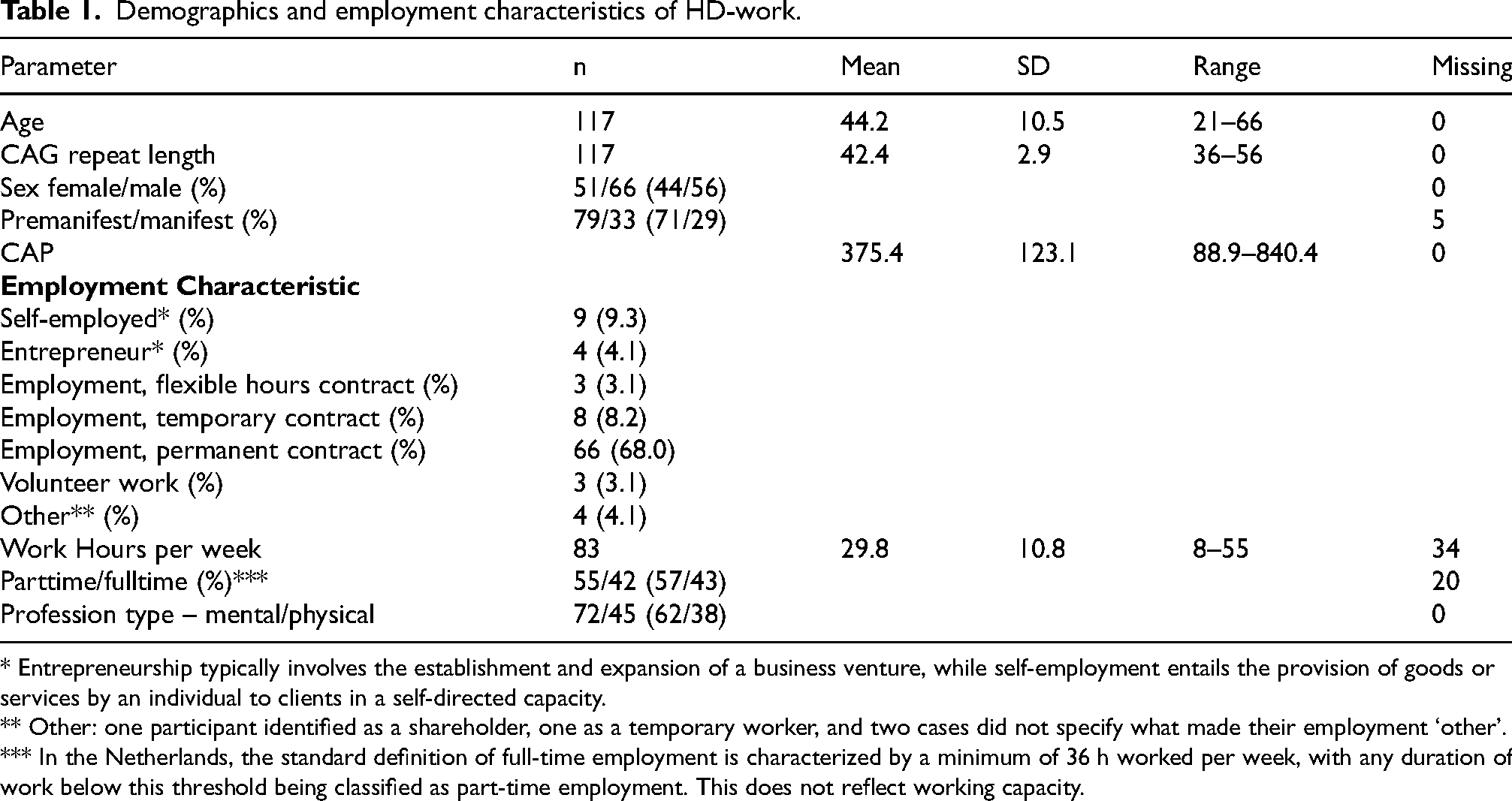
* Entrepreneurship typically involves the establishment and expansion of a business venture, while self-employment entails the provision of goods or services by an individual to clients in a self-directed capacity.
** Other: one participant identified as a shareholder, one as a temporary worker, and two cases did not specify what made their employment ‘other’.
*** In the Netherlands, the standard definition of full-time employment is characterized by a minimum of 36 h worked per week, with any duration of work below this threshold being classified as part-time employment. This does not reflect working capacity.
Reliability of the HD-work questionnaire (Dutch version of the HDWF)
Cronbach's alpha for the Dutch translation of the first 20 items (the original HDWF) was 0.80 (95% CI 0.74 to 0.85), indicating good internal consistency. Moreover, G6(smc) = 0.87, average inter-item correlation = 0.17, and Signal-to-Noise Ratio (S/N) = 4.1. The standard error of measurement (ASE) was 0.027. The 5 items for additional insights into participants’ work capacity resulted in a Cronbach's alpha of 0.82 (95% CI 0.77 to 0.86). The G6(smc) = 0.89, average inter-item correlation = 0.16, and Signal-to-Noise Ratio (S/N) = 4.7. The standard error of measurement (ASE) was 0.024
We categorized groups based on the TFC occupation domain and participants’ responses to work status questions in the HD-work questionnaire, as some participants reported no work-related problems on the TFC but did mention reduced working hours or adjusted work responsibilities. We defined the outcome as binary: ‘full working capacity’ if participants reported no work-related problems and ‘limited working capacity’ if they reported any work-related problems. Comparing these groups, we see the following differences (Table 2). Firstly, the full working capacity group is younger, has a lower CAP score and performs better on cognitive and motor tasks than the limited working capacity group. Also, the limited working capacity group's cognitive scores indicate lower cognitive function on all tests but two, where they score comparable to the full working capacity group (i.e., the SIT and the VLFT). Work-related characteristics show that the group that does not have full working capacity works fewer hours and experiences more exhaustion and depersonalization. Notably, no significant differences in apathy levels were discerned between the two groups.
Comparison of participants with full and limited working capacity on demographical information, motor, cognitive, and work characteristics.
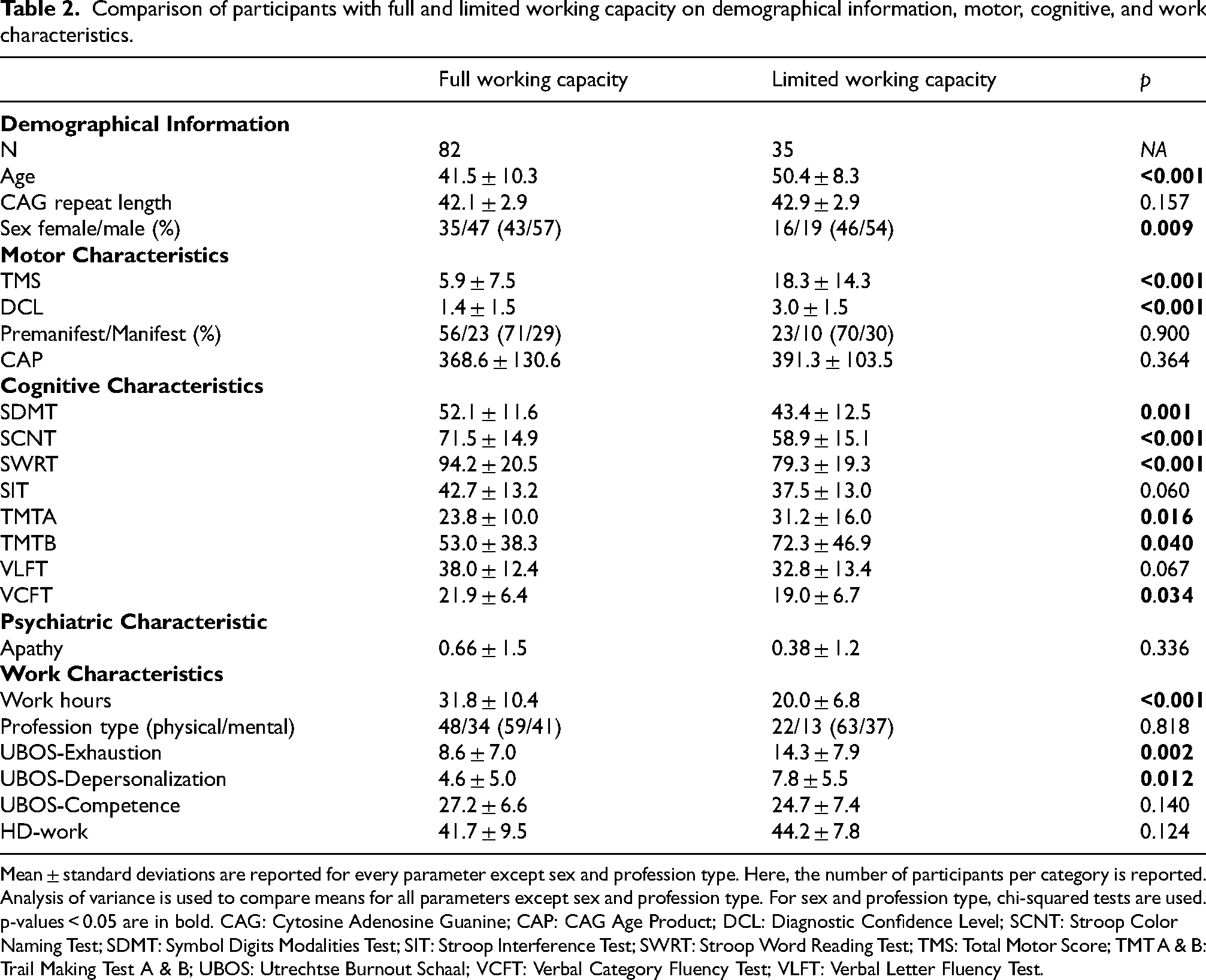
Mean ± standard deviations are reported for every parameter except sex and profession type. Here, the number of participants per category is reported. Analysis of variance is used to compare means for all parameters except sex and profession type. For sex and profession type, chi-squared tests are used. p-values < 0.05 are in bold. CAG: Cytosine Adenosine Guanine; CAP: CAG Age Product; DCL: Diagnostic Confidence Level; SCNT: Stroop Color Naming Test; SDMT: Symbol Digits Modalities Test; SIT: Stroop Interference Test; SWRT: Stroop Word Reading Test; TMS: Total Motor Score; TMT A & B: Trail Making Test A & B; UBOS: Utrechtse Burnout Schaal; VCFT: Verbal Category Fluency Test; VLFT: Verbal Letter Fluency Test.
We have also categorized participants on manifestation of the disease as defined by the UHDRS-DCL (Table 3). The premanifest group is younger, has a lower CAPscore and performs better on all cognitive and motor tasks than the manifest group. They do not differ on apathy, or any of the work- and burnout outcomes.
Comparison of premanifest and manifest participants on demographical information, motor, cognitive, and work characteristics.
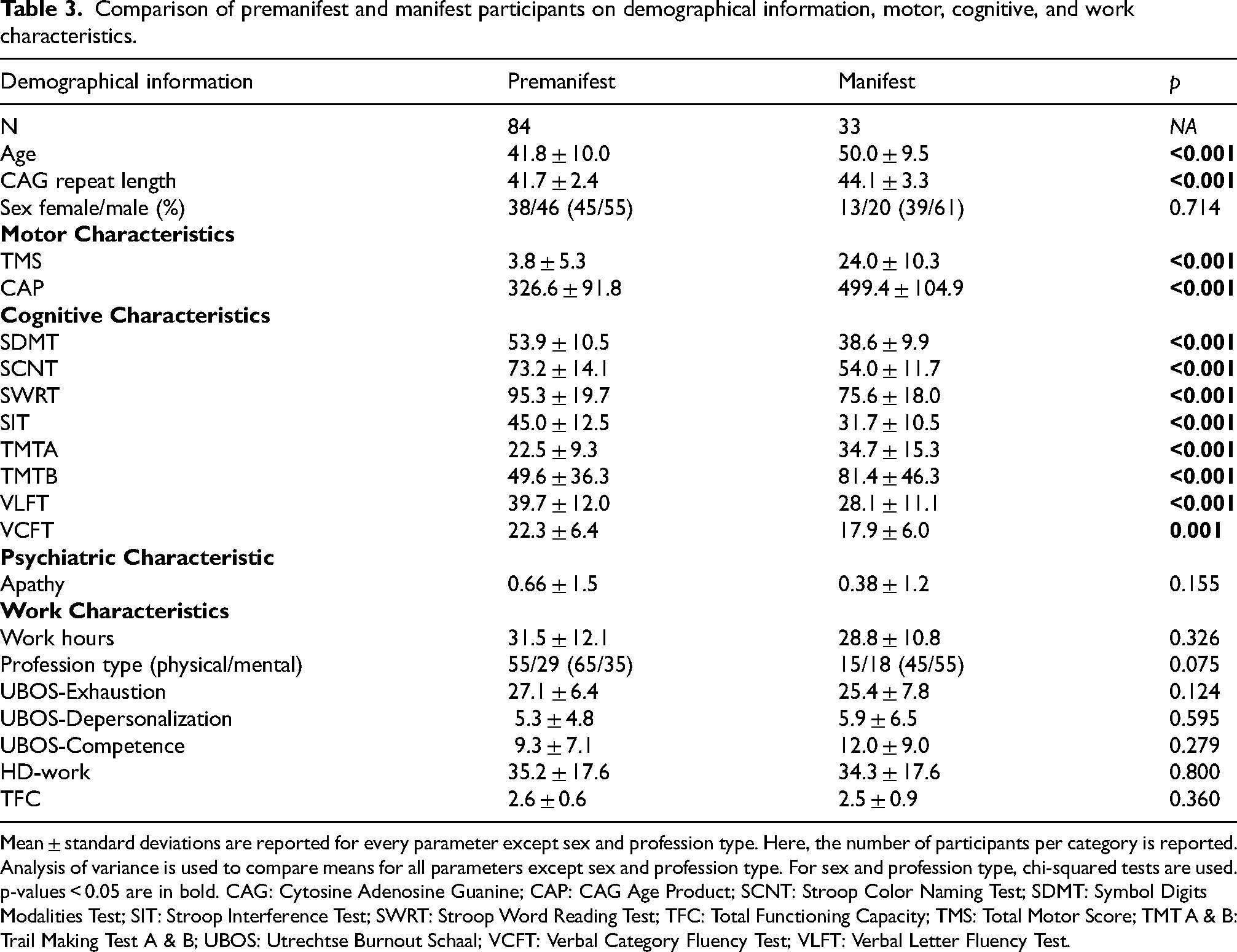
Mean ± standard deviations are reported for every parameter except sex and profession type. Here, the number of participants per category is reported. Analysis of variance is used to compare means for all parameters except sex and profession type. For sex and profession type, chi-squared tests are used. p-values < 0.05 are in bold. CAG: Cytosine Adenosine Guanine; CAP: CAG Age Product; SCNT: Stroop Color Naming Test; SDMT: Symbol Digits Modalities Test; SIT: Stroop Interference Test; SWRT: Stroop Word Reading Test; TFC: Total Functioning Capacity; TMS: Total Motor Score; TMT A & B: Trail Making Test A & B; UBOS: Utrechtse Burnout Schaal; VCFT: Verbal Category Fluency Test; VLFT: Verbal Letter Fluency Test.
Summary of binary logistic regression results.
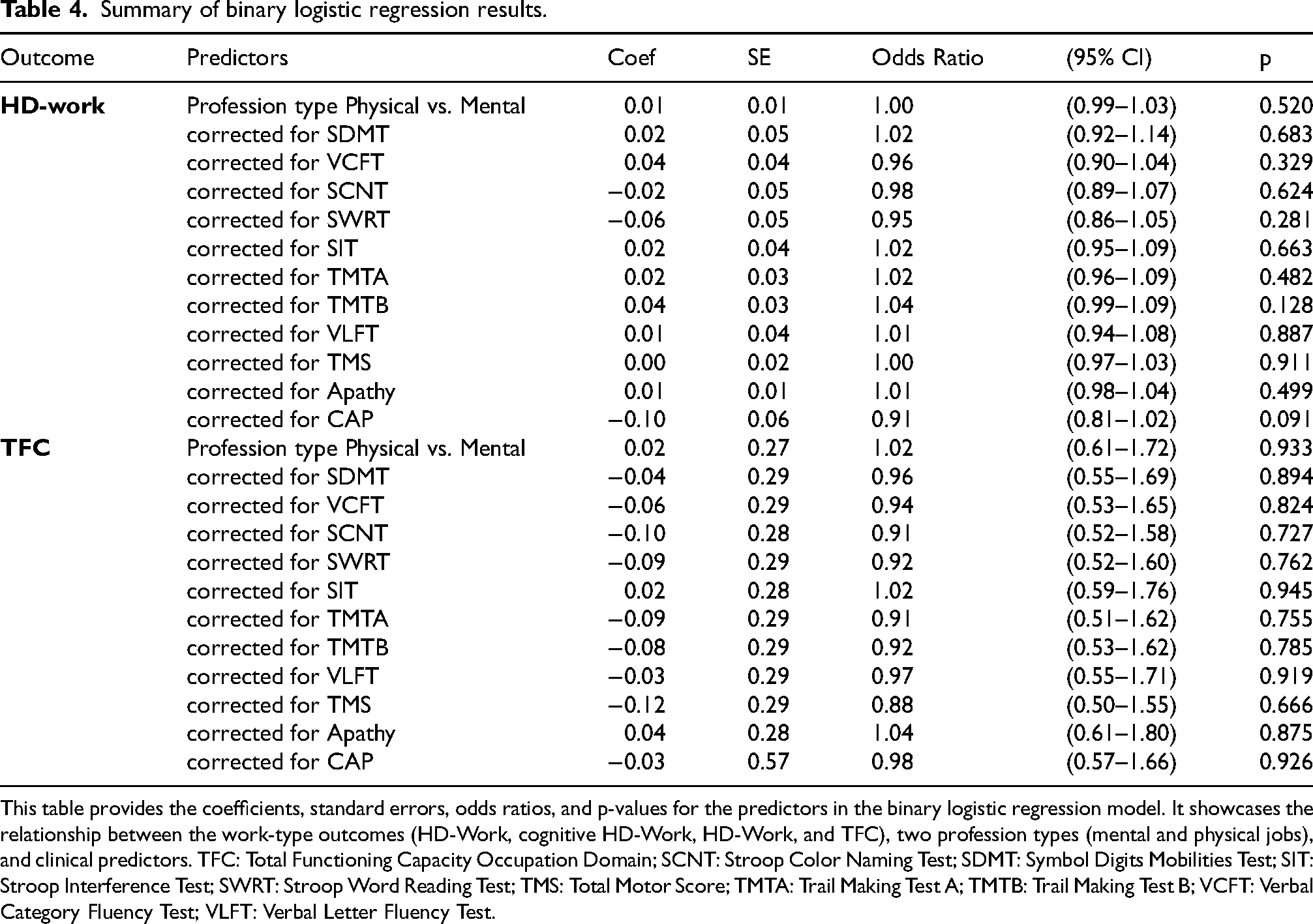
This table provides the coefficients, standard errors, odds ratios, and p-values for the predictors in the binary logistic regression model. It showcases the relationship between the work-type outcomes (HD-Work, cognitive HD-Work, HD-Work, and TFC), two profession types (mental and physical jobs), and clinical predictors. TFC: Total Functioning Capacity Occupation Domain; SCNT: Stroop Color Naming Test; SDMT: Symbol Digits Mobilities Test; SIT: Stroop Interference Test; SWRT: Stroop Word Reading Test; TMS: Total Motor Score; TMTA: Trail Making Test A; TMTB: Trail Making Test B; VCFT: Verbal Category Fluency Test; VLFT: Verbal Letter Fluency Test.
HD-work scores do not differ between premanifest and manifest participants (F(1,94) = 0.088, p = 0.800). Therefore, the TFC occupation outcomes are included in the last analysis. The TFC did not correlate significantly with any of the HD-work measures.
HD patients did not score differently on burnout-like symptoms (M = 2.02, SD = 1.57) compared to the general Dutch population 18 t(84) = −1.07, p = 0.29. 18 Only 5 participants reported burnout; one scored above average on every burnout domain, and the other four on one or two domains. Moreover, apathy significantly but not strongly correlated with exhaustion (r = 0.34, p < 0.001).
We further divided the sample into two groups: participants with a physical profession and participants with more mental abilities demands in their work. See the appendix for an overview of the reported professions and their distribution by mental or physical profession type. Profession type did not significantly affect the HD-work outcome and TFC outcome measures (Table 4). Nor did the addition of clinical characteristics or disease progression reveal any significant effects. When we perform a multivariate binary logistic regression with any or all covariates, no model remains significant due to multicollinearity (VIF > 10).
Discussion
In this study, the ability to work is unaffected by profession-specific requirements, even when combined with HD symptoms and signs. Individuals who have a profession with primarily physical requirements are not explicitly affected by the onset of HD motor symptoms. Neither are people with a profession with mental requirements overly influenced by the onset of cognitive symptoms. Notably, individuals with limited working capacity had significantly higher motor scores and performed worse on some cognitive tests compared to those with full working capacity. Despite these findings, disease progression and other clinical characteristics did not independently predict better work outcomes. Therefore, workplace adjustments should be tailored to individual preferences rather than being based solely on the general clinical expression of HD. Therefore, adjustments to the workplace based on profession-specific requirements and the clinical expression of HD should be tailored to the individual's preferences rather than the disease in general.
We have found -not unexpected- differences between premanifest and manifest participants, and those who are working at a normal working capacity and those at limited working capacity. Notably, the manifestation of the disease itself did not influence the work outcomes.
Burnout or burnout-like symptoms in HD did not significantly affect the ability to work in our cohort. Although exhaustion and depersonalization are reported more frequently in people with reduced working capacity, these symptoms do not score above the threshold for clinical burnout, according to the UBOS manual. The current sample has approximately the same ratio of burnout-like symptoms as we see in the Dutch population, roughly one in six. 18 Participants did not experience feelings of incompetence. Therefore, burnout-like symptoms may reflect other symptoms associated with HD. For instance, exhaustion may be more akin to fatigue caused by HD. Moreover, depersonalization (the feeling of detachment from one's emotions, thoughts, or body, often resulting in the feeling that the world is strange or unreal) is closely related to anxiety, 22 which is very prevalent in HD. Therefore, the association between anxiety and mild reports of depersonalization in HD may be worth studying.
In contrast to previous studies highlighting apathy as a significant contributor to work decline in early stages of HD,5,6 our findings did not demonstrate a significant association between apathy and work outcomes. This discrepancy suggests that while apathy is recognized as a key clinical feature in HD, its impact on work capacity may vary across different study populations and settings. Moreover, apathy is also not associated with exhaustion in this study, therefore not confirming our initial hypothesis.
US-American researchers developed the HD Work Functioning Scale (HDWF) and reported that the scale discriminates between premanifest and manifest HD mutation carriers. 19 Since we are utilizing a scale derived from the HDWF (i.e., HD-Work Questionnaire), we hypothesized that it would effectively distinguish between premanifest and manifest participants. However, our sample did not yield significant differences between the two groups. Similarly, the HD-work scores did not differ between participants with full working capacity and those with limited working capacity, nor were they associated with the occupation item of the Total Functional Capacity (TFC), a basic work outcome measure in HD.
A limitation of our study is that it contained predominantly premanifest and prodromal participants, probably resulting in a too-skewed divided sample to provide any information on the validity of the HD-work questionnaire in discriminating between premanifest and manifest mutation carriers. This limits the generalizability of our findings to the overall HD population. The majority of our sample at baseline is premanifest or prodromal, as our study aimed for a long-term follow-up to look at the progression to manifest HD. Our longitudinal study's data was heavily influenced by the COVID-19 pandemic and the consequently changing working conditions that affected everyone. Moreover, in contrast to US citizens, in the Netherlands, more premanifest and prodromal individuals carrying the HD-expanded gene mutation seek hospital assistance regardless of their disease stage, possibly due to a better health insurance system. In addition, cultural differences in occupation and social security systems between the Netherlands and the US may also play a role. Prior research has shown distinctions in work and work-related attitudes between the US and other countries. 2 However, these cross-cultural effects were not considered in this analysis and warrant further investigation in future studies.
Furthermore, because our main analysis did not provide clinically significant findings, we explored a qualitative analysis comparing participants with the same professions. Here, we closely tried to study the differences and shared experiences. However, due to the limited sample size, as few individuals shared the same profession within our cohort an analysis was impossible. Those with the same profession missing values on other variables limited the analyses. While the diversity in occupations enriched our sample, it restricted the possibility of qualitative interpretation. A separate study, carefully matching individuals in the profession, disease stage, sex, and other factors, might shed light on the shared experiences of HD-expanded gene carriers and their job roles.
Another limitation was the arbitrary division between physically and mentally demanding professions. Many professions involve a blend of physical and mental demands, making it challenging to categorize individuals accurately. For example, consider a nurse's role, which involves physical and mental tasks. We explored whether this issue could be solved by adding a third ‘mixed’ group. However, this analysis yielded no clinically relevant or statistically significant findings, thereby confirming that profession-specific requirements related to HD clinical manifestations do not play a major role in work outcomes.
Conclusion
In conclusion, our study suggests that profession-specific requirements may not significantly impact the ability to work among individuals with HD in our sample of participants in relatively early phases of HD. Therefore, workplace adjustments should be tailored to individual preferences rather than assumptions based solely on profession-specific demands. Regarding burnout-like symptoms, our findings indicate that these symptoms did not appear to markedly affect work capacity in our participants. Further research is needed to investigate the relationship between burnout-like symptoms such as depersonalization and exhaustion and HD symptoms.
Supplemental Material
sj-docx-1-hun-10.1177_18796397241288161 - Supplemental material for Huntington's disease at work: The effect of profession-specific requirements as related to clinical characteristics on work outcome
Supplemental material, sj-docx-1-hun-10.1177_18796397241288161 for Huntington's disease at work: The effect of profession-specific requirements as related to clinical characteristics on work outcome by Kasper F. van der Zwaan, Milou Jacobs, Raymund A. C. Roos and Susanne T. de Bot in Journal of Huntington's Disease
Footnotes
Acknowledgments
Data used in this work was generously provided by the participants in the HD-Work study. HD-work would not be possible without the vital contribution of the research participants. We would also like to thank Fleur Mijssen (FM), Merijn Mulder, Esther Arendts, Amy Putman, Hannah Bakels, Stephanie Feleus, Nadine van de Zande for their contributions to HD-work.
Funding
This study was conducted without any external funding.
Declaration of conflicting interests
Authors K.F. van der Zwaan and S.T. de Bot are members of the European Reference Network for Rare Neurological Diseases - Project ID No 739510. Leiden University Medical Center receives grants from the European Huntington's Disease Network (EHDN) and Cure HD Initiative (CHDI), participates in an EU Horizon 2020 project: Innovative Medicines Initiative (IMI) 2 (IDEA_FAST), and participates in clinical trials sponsored by PRILENIA, PTC Therapeutics, WAVE and VICO Therapeutics. The aforementioned sponsors had no role in the design, execution, interpretation, or writing of this manuscript.
R.A.C. Roos is part of the DSMB uniQure CT-AMT 130, DSMB Enroll-HD. R.A.C. Roos is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review.
M. Jacobs has no conflicts of interest to report.
Data availability
The data supporting the findings of this study are available on request from the corresponding author. The data is not publicly available due to privacy, ethical restrictions, or other concerns.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.