
Abstract
Complementary and alternative therapies (CAT) is an umbrella term applied to a diverse set of approaches, with high interest among persons with Parkinson's disease. However, scientific community regards evidence-based medicine as the only acceptable, creating a black and white dichotomy, which is neither epistemologically correct nor workable in daily practice. CAT are heterogeneous, and the label is dynamic as new scientific insights might accrue. Medicine encompasses a wide range of interventions that can be positioned alongside a spectrum of credibility, with many shades of grey between the extremes. We define credibility along three dimensions: the underlying rationale, the scientific rigor, and patient perceptions. By no means this implies we encourage adoption of weakly grounded therapies, or favor exotic treatments over evidence-based approaches. Credibility serves as basis for a nuanced debate in clinical practice, with attention to adverse effects, interactions, and costs. The degree of credibility also informs the need for further research. This offers a practical road forward for open-minded, yet rational decisions by persons with Parkinson's disease, clinicians, funding bodies and relevant stakeholders.
Introduction and background
Complementary and alternative therapies (CAT) is an umbrella term applied to a wide and heterogenous set of approaches, from homeopathy to traditional Eastern medicines. 1 The interest in CAT has increased in the last decades, particularly among persons affected by chronic and progressive diseases. In Western countries, interest seems particularly high among women and those with a higher income or more education, but also among ethnic minorities.2,3 The use of CAT is also high among persons with Parkinson's disease (PwP). 4 This is true not only in Eastern countries (CAT use over 76% in Korea, 61% in Singapore) but also in Western countries (at least 30–60% in Sweden, USA and Ireland).2–5 The actual numbers might be even higher because of underreport. For example, less than half of PwP discusses the use of herbal supplements in clinic, possibly by fear of being misjudged or criticized by their attending doctors, who rarely are curious or knowledgeable about such therapeutic strategies2,5,6
Several reasons may account for the growing interest in CAT, such as disillusionment with usual care, personal interests and beliefs, and shared experience of other PwP (Table 1).2–4,7 Many healthcare users search for more holistic and integrative approaches than what is offered by Western medicine.2,7,8 Physicians who prescribe CAT commonly deliver these in a rather personalized way, with a great deal of attention to each individual's narrative and peculiarities, frequently emphasizing the need for an active role of the subject and whole mind and body involvement. They generally avoid the rush and alienation that unfortunately characterizes many Western medicine healthcare systems, and they rely on time, self-explanation, listening and coaching the person in their disease journey. Undoubtedly, all this enhances a powerful placebo effect, and augments the perceived quality of the therapy, resulting in high satisfaction rates by the users.9,10
Some potential benefits and drawbacks of CAT.
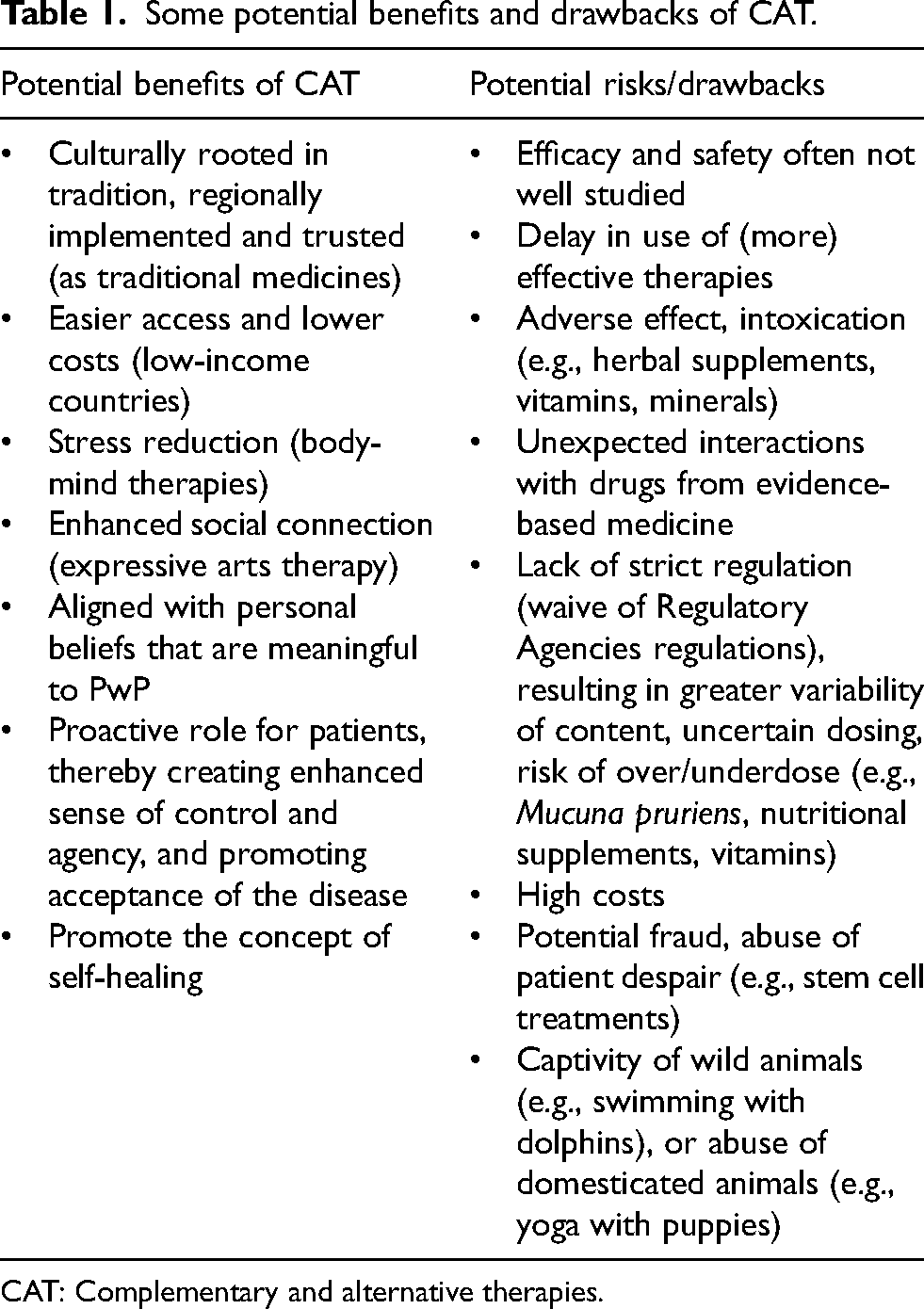
CAT: Complementary and alternative therapies.
However, the clinical and scientific community does not share this interest that much. In a 1998 New England Journal of Medicine editorial, CAT – and specifically herbal supplements – were criticized fiercely because of the lack of evidence, insufficient safety regulations and risks of adverse events for users, such as intoxication or poisoning.11,12 The unambiguous conclusion was: “There cannot be two kinds of medicine — conventional and alternative. There is only medicine that has been adequately tested and medicine that has not, medicine that works and medicine that may or may not work”. As such, this editorial reflected the widely felt perspective of a black and white distinction between classic evidence-based medicine (EBM) and CAT approaches.
This position may be understandable if one takes EBM as the only way to judge the merits of a particular treatment. However, this black and white distinction ignores the increasing interest in CAT among PwP, and the widespread use of such therapies. Given the great heterogeneity of CAT (Table 1), it also seems inappropriate to lump them altogether under one umbrella, especially since boundaries are difficult to draw. Moreover, panels may shift: many therapeutic approaches once considered as being largely alternative, such as physical exercise, have become settled, evidence-based interventions.13–15 Also, some CAT may be challenging to test under EBM conditions (e.g., difficulty to find properly matched placebo interventions, or to isolate the most effective elements of complex interventions). Finally, it is interesting that we have accepted many interventions without ever fulfilling a formal EBM requirement, parachutes being a prime example. 16 In the PD field, levodopa and apomorphine had been prescribed for decades before adequate randomized controlled trials (RCTs) were performed.17,18 In these cases, the introduction was facilitated by clear effectiveness, feasibility, safety and, importantly, credibility of the intervention.14–18 And even within the realm of EBM, there is not always a clear-cut distinction between what works and what does not.
In this viewpoint, we argue that a categorical separation into two opposing extremes is neither epistemologically correct nor optimally workable in daily clinical practice. Of note: we do not encourage adoption of weakly grounded therapies, or favor exotic treatments over evidence-based approaches. We do provide an alternative for a black-and-white distinction, by reasoning that the world of medicine encompasses a wide range of therapeutic interventions that can all be positioned alongside a spectrum of credibility, with many different shades of grey in between the extremes at both ends. We first define this concept of credibility (which is more comprehensive than merely EBM), and then illustrate how various interventions for PD might be positioned along a continuum of credibility. We also address issues such as adverse effects, unexpected interactions and costs. We conclude by offering a practical road forward, which we hope will offer a basis for open-minded yet rational decisions, not just for those affected, but also for clinicians, funding bodies and other relevant stakeholders.
The concept of credibility
We define credibility according to three complementary dimensions. The first relates to the
The second dimension relates to the
The third dimension of credibility relates to the way in which a specific treatment is perceived by an affected individual. We refer to this as
Shades of grey along a spectrum of credibility
We illustrate the spectrum of credibility in Figure 1, where the x-axis represents a non-quantitative scale of credibility, in this case determined by a sum of the rationale and available scientific evidence. In this graph, we did not incorporate the third dimension (the patient's perspective on the credibility of the treatment), as it is impossible to weight this properly against both other dimensions. This credibility scale gradually progresses from interventions with an extremely low degree of credibility, which are positioned at the left end (deep black), along multiple shades of grey until it becomes clear white at the right end, for interventions that have a high degree of credibility. The treatment costs are explicitly not part of the credibility spectrum, because these can be high for both rational, adequately tested interventions (such as immunotherapy for cancer) and irrational therapies (such as intravenous stem cell therapies for PD). This is not to say that costs are unimportant: unnecessary expenditures by PwP should be avoided by strongly cautioning against the use of therapies that have a low degree of credibility.
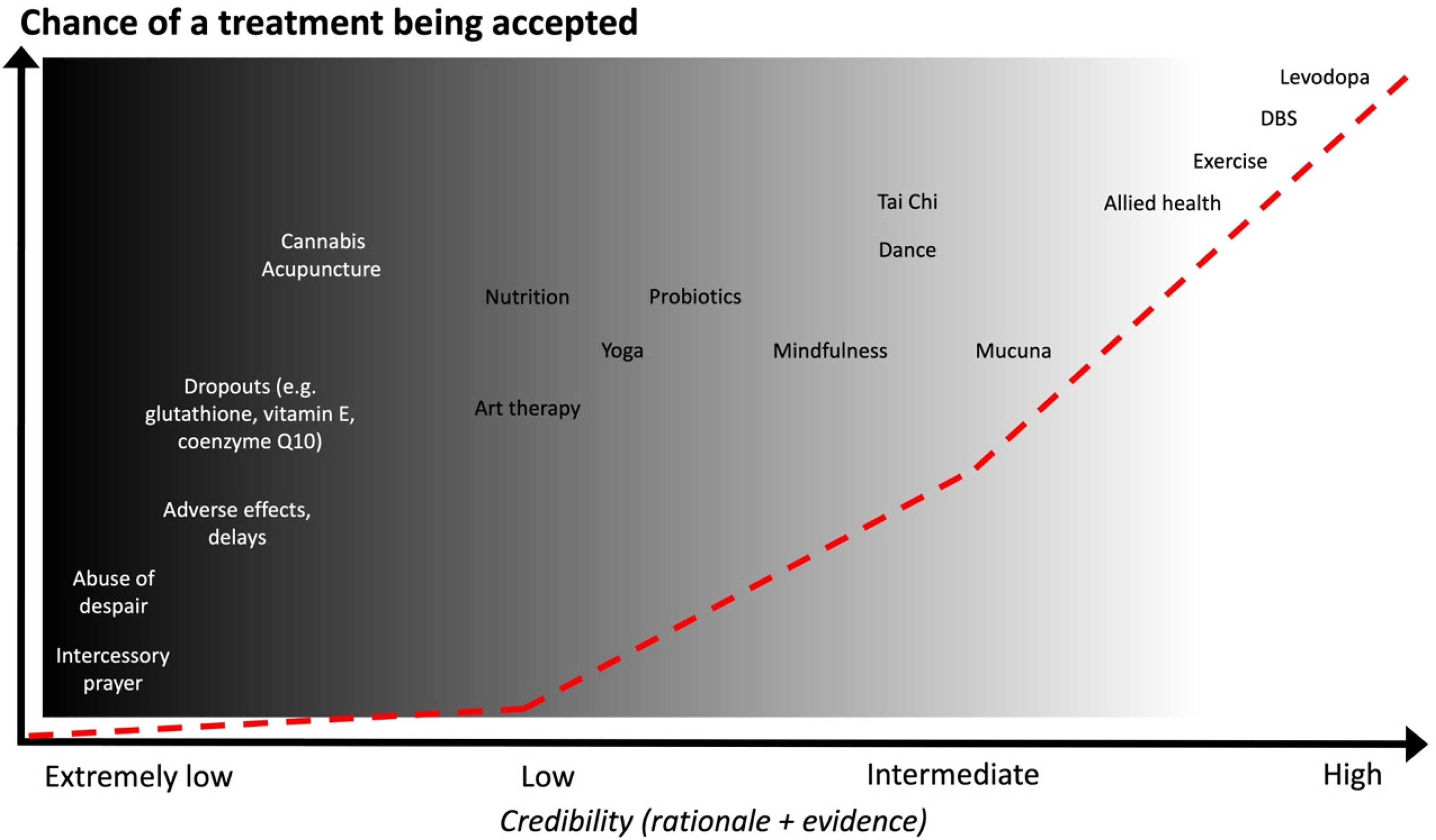
The shades of grey alongside the spectrum of credibility. Examples of different therapies are placed alongside the axis of credibility, considering a weighted sum of the rationale behind the intervention and the available evidence. The list of illustrated interventions is merely illustrative and far from comprehensive. We did not aim for preciseness and acknowledge that the exact position of each intervention in the graph is arbitrary and open for further debate. Instead, our aim is to present graphically how blurred the shades of grey may be in between the black and white ends.
Examples of different interventions
At the left end of the graph in Figure 1 (black part of the spectrum), we have positioned a mix of more exotic therapies and therapies that are proven to be ineffective. The exotic therapies, unfamiliar to mainstream medicine, lack scientific evidence and often also plausibility. These treatments are delivered mainly by non-medical professionals. Some may carry potential risks, can come with excessive costs and have a low probability of being helpful. Examples of proven ineffective treatments are glutathione, coenzyme Q or vitamin E, all shown to be inefficacious in properly designed studies.7,28,29 Also, unlike conventional drugs, dietary supplements have been exempted from Food and Drug Administration (FDA) regulation in the United States since 1984, and homeopathic products since 1938. There are also safety concerns when considering these products.11,12 This is relevant as vitamin and mineral supplements carry a risk of intoxication and poisoning (e.g., hypercalcemia with excess of vitamin D, polyneuropathy with B6, manganese intoxication due to mineral supplements). 30 Despite the hype in the PD community, controlled trials on cannabinoids have so far yielded negative results, and there are concerns about their safety (cognitive adverse events, for example).31,32
As clinicians, we are also responsible for preventing fraud or abuse of patients’ despair. An exemplary, highly disconcerting development relates to private companies that offer stem cell therapies to patients via Internet, without any supporting research, often at high prices; there is an important role for clinical professionals to safeguard patients from such malpractices. 33 Recognizing which therapies are justly placed into this black end of the credibility spectrum thus has implications for clinical practice, but also on the research agenda because we would discourage further research into such interventions.
At the right end of the graph (the whiter part of the spectrum), we place treatments that are supported by a solid evidence-based scientific background, with clear efficacy and acceptable risks. Examples include levodopa and deep brain stimulation, noting that the latter therapy has a lower credibility degree than levodopa because it is more challenging to perform fully placebo-controlled trials. 23
Science is a dynamic process, and so is the concept of credibility, where colors may shift. Panels will undoubtedly move as more knowledge is accrued, new evidence emerges and personal experiences grows. As we pointed out earlier, some interventions that were once regarded as alternative therapies (because they lacked evidence) are now positioned more into the light grey part of the spectrum. This explains the position in Figure 1 for physical exercise. The evidence is weaker (but growing) for dietary approaches, such as the Mediterranean diet or high-fiber nutrition.15,34 These interventions do score additional points on the credibility scale because the underlying scientific rationale is often reasonable. Certainly, many PwP have a firm belief in the merits of nutrition.
What to do with the greys within the credibility spectrum?
Where the discussion becomes difficult, but also interesting, is around the many “grey” interventions that are positioned in the intermediate part of the credibility spectrum. Examples are abundant, and many therapies in this part of the spectrum are used widely by PwP. For example, Mucuna pruriens has established its non-inferiority compared to levodopa (with possibly better tolerability and more rapid onset of effect) in a properly designed trial. 35 However, in Western countries the cost is high, and it is marketed as a dietary supplement, lacking the regulatory framework of conventional drugs. With less strict regulation, the accepted variability of the active principle included in the preparations is higher, as low as 6% and as high as 143% of the claimed levodopa content. 36 This poses challenges to dosage and prescription regimes and increases the likelihood of underdosing or adverse events; this limits its progression towards the white end. Importantly, many patients do not report the use of Mucuna pruriens with their physician, because they perceive this as a natural plant-based product that is relatively innocuous, or perhaps for fear of negative repercussions by their physician. 6 Yet, Mucuna pruriens is actually an effective treatment, and its concurrent use with chemically manufactured levodopa may complicate the finetuning of dopaminergic medication.
Other interesting therapies in this medium grey category include mindfulness and yoga. There is increasing evidence to support their merits for stress management and improving motor and non-motor symptoms of PD. Safety is rarely a concern, and this earns these interventions a position towards the whiter end of the spectrum.3,24,37–39 It is not surprising that anxiety-relieving strategies have such a positive impact on PwP, as the effects of stress may be overwhelming: stress may unmask PD40,41 and worsen tremor as well as other motor and non-motor symptoms.24,25,40 Expressive arts therapies are highly valued by PwP (high degree of perceived credibility), but currently score low when it comes to evaluation in terms of EBM. Yet, these interventions do have some credibility because the rationale is attractive: art interventions can promote disease acceptance, increase self-esteem, reduce stigma and alleviate loneliness, with additional benefits of social connection in group activities.42–45 The reflections of PwP on art therapies are remarkable; certainly, few drugs ever elicit such responses. 46 Moreover, dance (specifically tango) and tai-chi are supported by well-designed trials, showing benefits in balance and motor and non-motor variables, with sustained benefits in the long term.47–50 Again, these are arguments to place these interventions into the whiter end of the greys scale.
For traditional medicine, the evidence (as defined according to Western medicine) is lacking, giving these interventions a generally poor reputation in the EBM world. Yet, several components of the mainly plant-based treatments of Traditional Chinese medicine and Ayurvedic medicine (which includes Mucuna pruriens) have at least somewhat of a rationale, with e.g., antioxidant properties as demonstrated in animal studies, or with evidence of MAO-B inhibition. 7 Available studies, especially for Chinese Medicine components, are limited by methodologic flaws, but generally – and cautiously – point towards their potential usefulness as add-on therapy to levodopa, with generally good tolerability.51–54 These data are presently insufficient to justify a prescription in clinical practice, but may justify further research to clarify the efficacy and safety. Also, studies assessing biological pathways can add to their credibility.
Another issue to consider is that in many parts of the world, especially in low-income countries, therapies classified as CAT are the most feasible, economic and accessible treatment strategies for PwP. Ayurvedic medicine is mostly based on dietary and plant-derived products that patients may find in their local markets and gardens, while mainstream drugs come with high costs and poor availability. 55 Pranayama, or breathing exercises, have potential in relieving anxiety, perceived stress and insomnia, at virtually no cost, beyond the time invested to learn and practice them. 56 There is a growing scientific rationale and initial evidence to support the merits of such breathing exercises. 57 The same applies to chanting and folklore dances, again bearing in mind that there is some EBM support for the merits of dancing for PwP.41–44 Also, in most Eastern countries (China, India, Korea, Japan), these approaches are tightly linked to history and culture, taught in medical school, covered by insurance companies, and widely consumed by PwP, as the main therapies or in association with Western Medicine approaches.2,4,6 In these large, highly populated areas of the world, perhaps the term “alternative” applies best to Western medicine, and the perceived credibility and acceptability of CAT interventions is actually higher. The local accessibility, the widespread confidence in these treatments and the initial supporting evidence to our mind justifies further research.
Many interventions come with a strong placebo effect. This can have a particularly great impact on the treatment response in PD, which is unusually sensitive to such placebo effects. These placebo effects are usually short-lived, although experience in trials suggests it can last for up to several months.58,59 However, if a particular treatment is personally relevant according to an individual's beliefs and perceived as effective, if the costs are reasonable, and if the safety and feasibility are warranted, then it is worth considering to prolong the “self-healing” effect of placebo responses. Of course, one would ideally want to prescribe only interventions with a high level of supporting evidence, but for some interventions traditionally allocated as being CAT, that evidence may never arrive.60–62 PwP may not be willing to wait for further research to be funded, performed and published before they try something that is meaningful and appealing to them. However, clinicians must always be transparent in disclosing where a particular intervention resides alongside the spectrum of credibility, so that the PwP can make a well-informed decision.
Conclusions and future directions
We have motivated how the wide range of available therapeutic interventions can be ranked according to a credibility scale. This includes interventions that would be rated as traditional Western, evidence-based medicine and interventions formally labeled as CAT strategies. Their degree of credibility is determined mainly by the underlying scientific rationale and available evidence from the traditional EBM framework. However, the perceived belief and expectation among PwP should also be considered. The multi-dimensional concept of credibility is a helpful basis for a rational debate around a particular intervention, in both clinical practice and research.
With regard to clinical practice, we explicitly do not aim to stimulate a thoughtless adoption of unregulated and even potentially dangerous or costly interventions. Neither do we favor alternative therapies over evidence-based medicine, or do we equate personal interests or beliefs with scientific data. We do stimulate a debate around all three dimensions of credibility in a shared decision process, together with affected individuals. A common example is when PwP express an interest in interventions that score poorly on the first two dimensions, but that nevertheless are met with a high degree of perceived credibility. Initiating an open dialogue about the position of that particular intervention alongside the spectrum of credibility, and explaining the difference between e.g., scientific rationale vs perceived credibility, can help to reach a well-informed decision. Such a debate offers PwP a chance to explain why a particular intervention is appealing to them, and why they would like to resort to this, possibly after self-prescription (many products are available over-the-counter, or can be purchased via Internet). The credibility debate will lead to a nuanced discussion around the pros and cons of interventions, including safety and costs, rationale or plausibility, possible working mechanisms, likelihood of effectiveness, quality of preclinical and empirical evidence, feasibility, and the particular meaning for the PwP.
We feel that an open credibility discussion can build trust in the clinical relationship, supporting both PwP and clinicians. For PwP, it increases self-management and offers a sense of agency and control, especially if the discussed interventions are meaningful to them. Clinicians may find it helpful to explain why a high degree of credibility enhances the likelihood of a treatment being prescribed by medical professionals and, conversely, why they are reluctant to prescribe or counsel interventions with a low credibility. Importantly, instead of being left in the dark, this discussion enables clinicians to be fully updated about any treatments that patients are receiving, which is important to safeguard possible interactions with other treatments, to monitor for adverse effects, and to avoid a possible delay of more efficacious treatments. Ideally, information about where specific interventions are positioned along the credibility spectrum should be present on e.g., websites or in printed brochures that are readily accessible to PwP, so that clinicians save time during their busy consultations. 63 Finally, clinicians may learn from the way alternative strategies are typically being communicated: taking sufficient time to explain the underlying rationale, with a coaching style, with personalized and holistic attention, and by promoting hope (“hopamine” as a PD advocate accurately defined). 64
Credibility can also impact on how funding bodies decide which type of research to fund. In times of financial scarcity, our limited resources should not be wasted on irrational interventions that are positioned in the dark grey areas of the credibility spectrum. But it is fair to have a debate around interventions for which a reasonable rationale exists, but which have thus far not been tested properly. Properly designed research can help to reduce the uncertainty around interventions that are presently in the medium part of the spectrum. Some interventions may prove to be highly efficacious and cost-effective, thus shifting them further to the right end of the spectrum of greys. Positive findings from adequate research can thus offer a well underpinned motivation to promote the wider use of specific interventions. Conversely, other interventions may prove to be ineffective, unsafe or excessively costly, consequently shifting them towards the left alongside the credibility spectrum. This provides credible ammunition to definitively discard ineffective treatments that offer false hope to patients, sometimes at the expense of their health (in case of adverse effects), and help to avoid unnecessary financial loss. Indeed, an important perk of the credibility discussion is that it helps to ensure that PwP are protected from fraud and from making unnecessary financial commitments, and that exclusive engagement in therapies with a low credibility does not delay the installment of proven efficacious treatments.
Taken together, we regard credibility as a useful instrument that can support everyone's efforts in attaining optimal person-centered care for the many persons affected by PD worldwide.
Footnotes
Acknowledgements
The Radboudumc Centre of Expertise for Parkinson & Movement Disorders was supported by a center of excellence grant of the Parkinson's Foundation. Professor Bas Bloem is the editor-in-chief of the Journal of Parkinson's Disease but was in no way involved in the external peer-review process.
Author contributions
Araceli Alonso-Canovas: conception, manuscript elaboration and review.
Olaf M Dekkers: original idea, manuscript elaboration and review.
Bastiaan R Bloem: original idea, conception, manuscript elaboration and review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.