
Abstract
Plain language summary
Stigma affects people living with Parkinson's disease (PD) and their families. Studies from different countries have examined how people experience stigma in their everyday life, the impact it has on their lives and what they do about it. This new research looked at existing studies reporting stigma experiences and grouped them together to understand the bigger picture of PD stigma. The researchers did extensive literature searches on different databases to identify and select all the relevant studies that reported stigma experiences. Twenty-two studies were found and analysed with a method called ‘thematic synthesis’, a common method to synthesise qualitative studies. The three main themes were: (1) living with self-stigma: some people feel inferior and vulnerable because of their condition, decide to keep it a secret and avoid meeting family and friends, (2) living with public stigma: many people who do not understand PD, have stereotypes about the condition and the symptoms which are not true and exclude or ignore people with PD and (3) living with structural stigma: people with PD feel vulnerable at work because they are judged for their condition. Our findings are important because they provide evidence that people living with PD experience different types of stigma and they need support to manage it. We need to design interventions to raise awareness of PD and fight stereotypes about PD, its symptoms and treatments.
Introduction
Parkinson's disease (PD) stands as the fastest-growing neurological disorder globally, ranking as the second most prevalent neurodegenerative disease following Alzheimer's disease.1,2 It is a chronic and progressive neurological disorder characterized by neurodegeneration in the main sources of dopamine involved in the control of movements, i.e., substantia nigra and ventral tegmental area. These pathophysiological processes give rise to marked slowness of movements (bradykinesia), accompanied by rigidity, postural instability or tremor at rest that are the classic parkinsonian symptoms, essential for a first diagnosis. Nevertheless, other alterations such as mood (depression, anxiety, apathy), cognitive and sleep disturbances or speech difficulties, make up PD too. 3 These, despite being common and contributing to the decrease in quality of life, often go unnoticed. 4 Therefore, many patients suffer in silence while their doctors focus on more visible symptoms such as tremor or sluggishness. In fact, many non-specialist doctors may not be aware of the complexity of PD and the significant non-motor load it represents in their day-to-day lives.
Lack of knowledge around the complexities of PD and the addition of different sources of stigma (ageism, mental health, etc.) make PD one of the most stigmatizing diseases. Factors such as visible motor symptoms, cultural misconceptions, and age-related biases amplify the experience of stigma. The World Health Organization (2022) 2 highlights how the lack of awareness and understanding about PD leads to stigmatization and how it may delay presentation to health care services and initiation of treatment, negatively affecting patients’ overall well-being. For example, imbalance may be perceived as alcohol intoxication and masked facial expression as an unfriendly demeanour. 5 Public and self-misjudgments can lead to social withdrawal, anxiety and isolation, reluctance to seek health care, loneliness, depression or stress, especially in younger patients and in women. 6
Stigma is a complex phenomenon that can arise from cultural and community misconceptions and beliefs about the disease. The general meaning of the word stigma is linked to a complex human experience including devaluating, discriminant, and discomfort feeling. It comprises negative attitudes, beliefs, stereotypes and discrimination that people may face due to their condition. 7 The evidence (see 6 for an overview) highlights that stigma significantly exacerbates the burden of PD, affecting patients’ physical, psychological, and social well-being. To break this significant barrier, a key starting point is to specifically identify the misconceptions and beliefs that drive stigmatization. However, due to the multifaceted and variable presentation, the social impact of PD is difficult to capture in quantitative research.
Qualitative methodologies can be very useful in uncovering people's perceptions and experiences of the different dimensions of stigma. A previous narrative review 8 of qualitative studies concluded that stigma is not only a feeling of shame and embarrassment arising from a self-perception of inadequacy (self-stigma), but also an experience related to the attitudes and beliefs of the social context towards the person who is stigmatized and forced to withdrawal (social stigma). Another scoping review 9 explored public knowledge of symptoms, causes and treatment of PD and highlighted a lack of understanding about the disease, the social consequences of the disease but also the lack of educational resources to increase public understanding of PD. To date, there has been no systematic review exploring all of these aspects from the perspective of the people living with PD and their families, which justifies the need for the current review.
The aim of this review was to rigorously analyze how people living with PD and their caregivers experience stigma by adopting a holistic approach, to provide an overview of specific dimensions of stigma, including public and self-stigma and to explore the impact of stigma on people living with PD. In this context, we expected to shed some light on how stigma shapes the illness’ perceptions and experiences of people with PD and their loved ones, but also explore behaviors and strategies used to tackle such stigma. A protocol 10 was published online setting out all aspects of our review plan.
Methods
We conducted a systematic review of qualitative studies using the thematic synthesis approach 11 and reported the synthesis following the Enhancing Transparency in REporting the synthesis of Qualitative research (ENTREQ) guidelines. 12
Inclusion and exclusion criteria
Qualitative studies that examined any of the aspects of stigma experienced by people living with PD and their caregivers were relevant for inclusion. Studies that explored experiences of living with PD but did not explicitly mention ‘stigma’ as the main focus or part of the findings, were excluded. Publications were screened as to whether they met the following criteria: (1) primary qualitative studies, or qualitative studies that were part of a mixed methods project, from any geographical location published from 2004 onwards. (2) The study population had to include either people living with PD (of any type, stage and age) or informal caregivers (e.g., family, friends, neighbors). (3) Studies had to examine either experiences, attitudes and/or beliefs around the diagnosis, experiences of treatment, social/work/personal life around PD, barriers and facilitators to living with PD and/or perceptions of how stigma has affected their lives. (4) Studies had to have used any qualitative approach (including grounded theory, ethnography, narrative analysis and phenomenology).
Studies were excluded if the sample was mixed (e.g., a mixture of people with PD and people with other long-term conditions) and the findings were not reported separately. The views of other adults (e.g., clinicians and other therapists), although important, were excluded from the scope of this review.
Search strategy
We used two main search terms (Parkinson* AND stigma) to capture our review question. Our search strategy was intentionally broad and inclusive to ensure retrieval of all relevant papers. 13 An experienced, professionally-qualified Information Specialist developed the search strategies for each database using keywords and subject terms.
Our initial search was performed in SCOPUS (February 2024) and following testing of the results, we expanded the search to three more databases: Web of Science, PubMed and EBSCO, covering Cumulative Index to Nursing and Allied Health Literature (CINAHL) and PsycInfo. We set a year limit in all databases (from 2004 to 2024) and languages (English and Spanish).
Knowing that qualitative studies can be particularly challenging to identify and retrieve, 14 we decided to complement our searches with hand searching. Searches of reference lists from relevant published papers, reviews and grey literature (such as conference proceedings, theses) were also conducted. 13 Duplicates were deleted and the final results were saved on a reference management package (Figure 1).
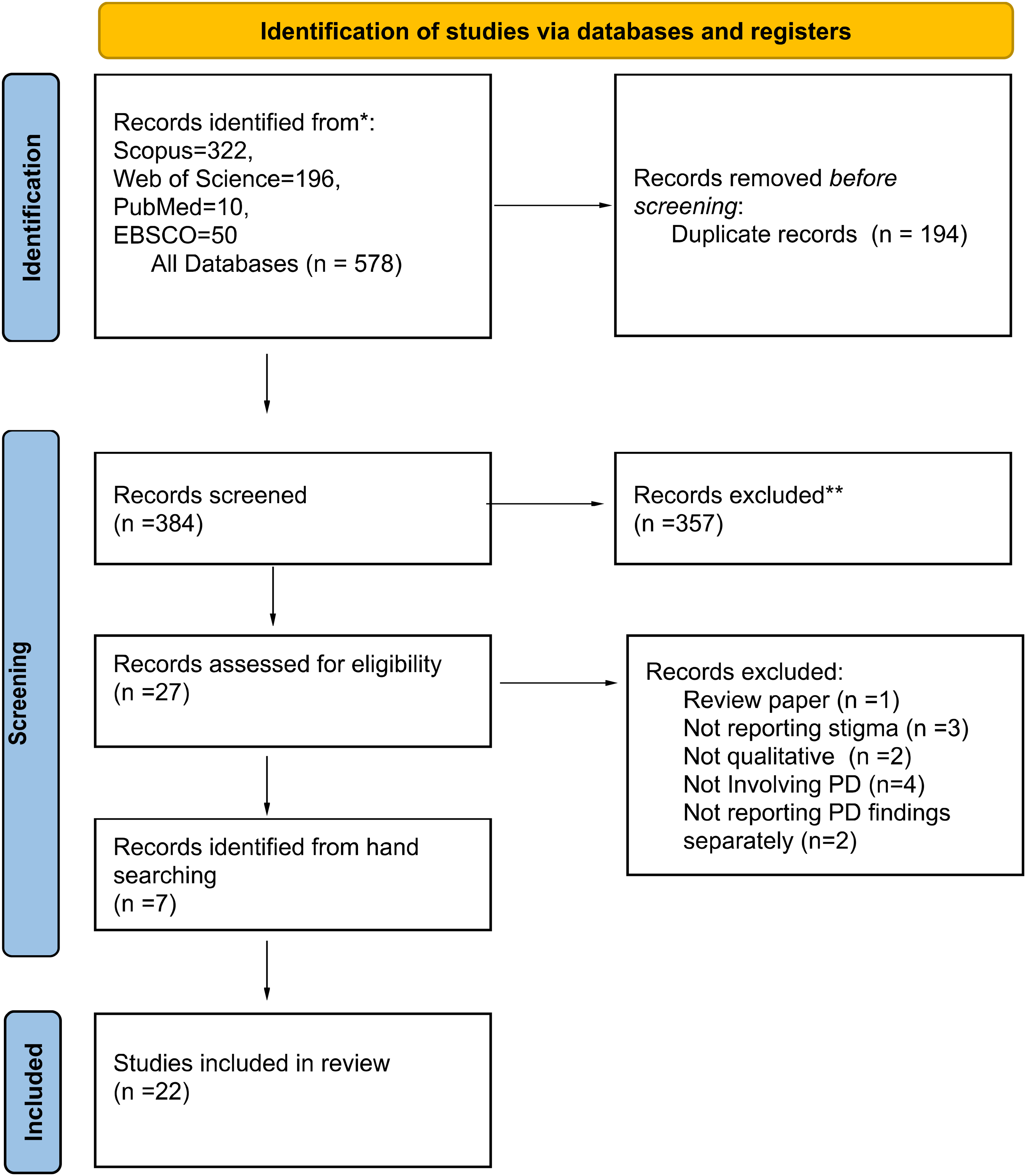
PRISMA flow diagram of the qualitative synthesis.
Data screening
Papers were double screened independently by two reviewers (DS, PA). Screening was done in two stages: first on titles and abstracts, and then on full papers. The two reviewers met to discuss their selection and disagreements were resolved by consensus or by discussion with a third reviewer (AS).
Data extraction
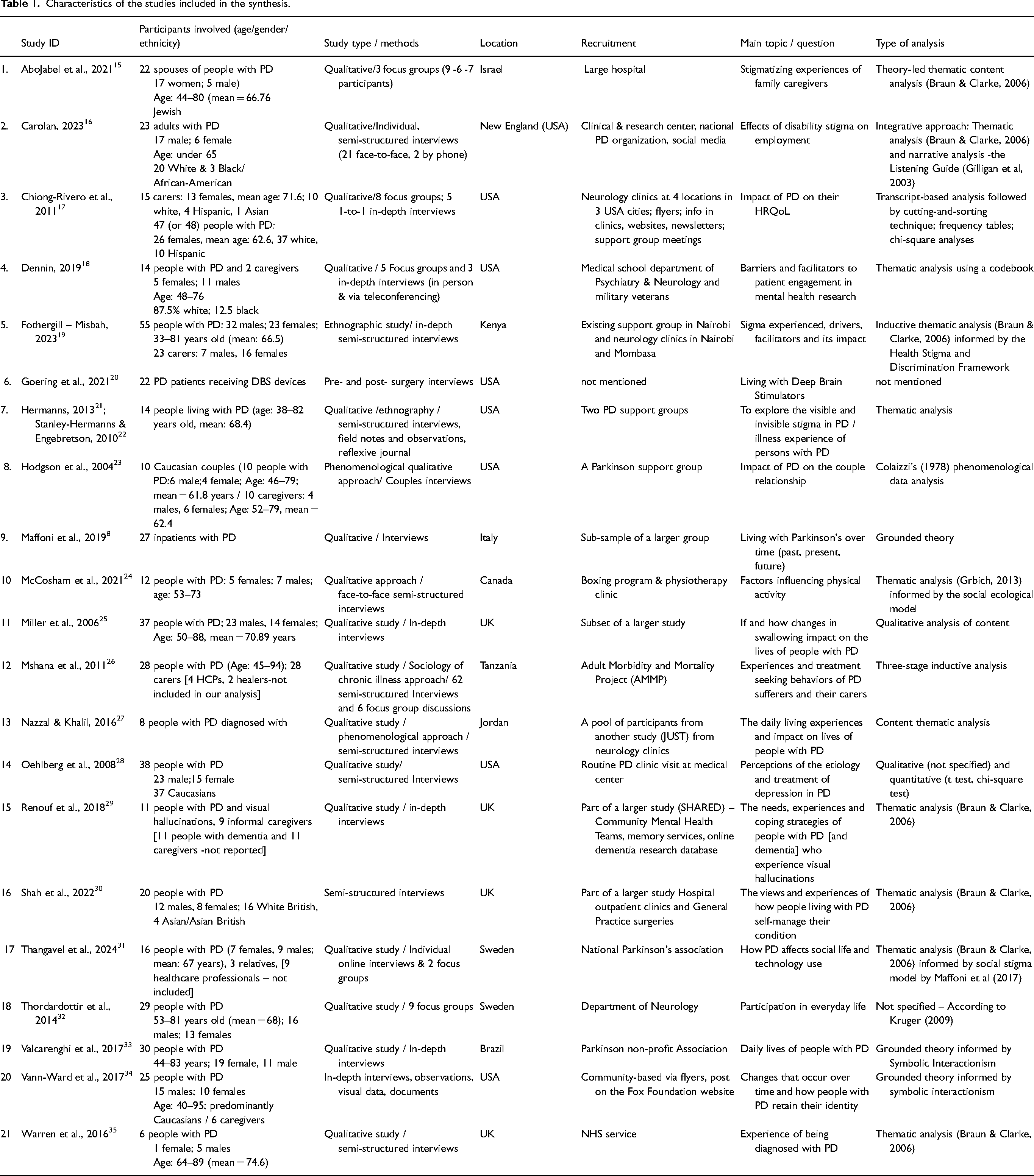
One reviewer (DS) extracted data from all included publications on an Excel file and a second reviewer (PA) checked them for accuracy. Data extracted included: author, year, population, sample size and demographics, type of study design, methods, setting, theoretical framework, method of analysis of the primary data (Table 1). If the same study (with the same sample and methods) was published in different papers, we collated them and extracted the data as one unit.
Characteristics of the studies included in the synthesis.
Another Excel form was used to extract data from the included papers and synthesize our findings. DS coded the text into domains reported by the authors of the included studies, or, were appropriately, created new domains. Relevant data (including text from the findings section, discussion and illustrative quotes) were extracted on the Excel file.
Quality assessment
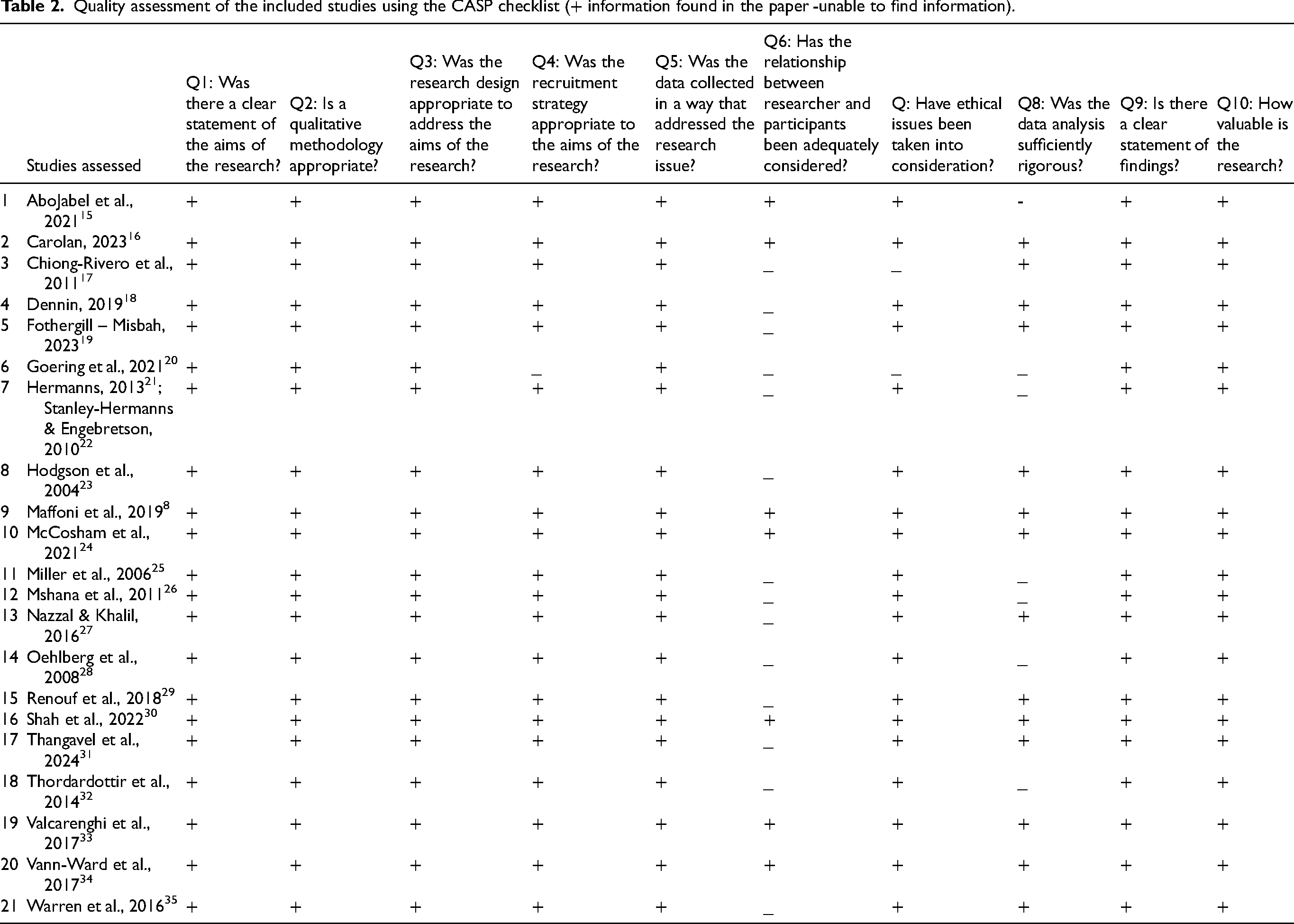
We used the Critical Appraisal Skills Programme (CASP) checklist, consisting of ten questions, to evaluate the included papers (see Table 2). We included all studies regardless of quality but acknowledging their strengths and/or weaknesses. 13 DS evaluated all studies independently and AS checked for accuracy, discussed and resolved any disagreements.
Quality assessment of the included studies using the CASP checklist (+ information found in the paper -unable to find information).
Data synthesis
This synthesis aimed to answer a predefined question using thematic synthesis. 11 Each included paper was systematically reviewed, coded and analyzed by DS. The co-reviewers (PA, AS) discussed the initial themes, helped to refine and validated the findings.
The analysis involved three stages: (a) reading each study repeatedly, highlighting the relevant text and then coding it in excel, (b) reading again the codes to identify similarities and differences across studies and grouping them together (if relevant) to produce descriptive themes/topics, (c) creating descriptive themes to ‘go beyond’ the original studies and answer the review questions. 11 Following discussion with all reviewers the final themes were agreed.
Results
Search results
As seen in the PRISMA Figure 1, our searches identified 578 papers (including 194 duplicates). From these, we doubled-screened 384 titles and abstracts and selected 34 for full screening. Twenty-two papers (21 studies) were finally included covering all the inclusion criteria for this review.
Included studies
All included studies are presented in Table 1. We found two papers21,22 that represented the same study. The studies represent data from seven countries: most of the papers (n = 9) were from USA,16–18,20–23,28,34 followed by studies (n = 4) conducted in the UK,25,29,30,35 Sweden (n = 2),31,32 Israel, 15 Kenya, 19 Tanzania, 26 Canada, 24 Jordan, 27 Brazil 33 and Italy. 36
The majority of studies (n = 17) reported that the data collection was conducted via semi-structured or in-depth interviews. Two studies used focus groups as their data collection method and four studies used both interviews and focus groups.
The participants’ characteristics were: 472 people living with PD and 98 informal caregivers. Not all the studies included information about the gender of participants. From those that reported the gender of the people with PD, 188 were females and 227 were males, predominately White and with ages ranging between 33 and 95. From the studies that reported the demographics of the caregivers, 46 of them were females and 14 males, predominately White.
The quality assessment of the included papers using the CASP checklist can be seen on Table 2 and the contribution of studies into our three themes are presented on Table 3. In terms of quality, six studies provided information to answer all questions on the CASP checklist and were considered of good quality. The majority of studies (n = 15) lacked or missed some methodological information (Table 2). The relationship between the researcher and participants was not reported in most studies (n = 14), followed by insufficient description of the analysis conducted (n = 7) and insufficient information of the ethical issues (n = 2). The sensitivity analysis examined if the final themes were affected significantly after removing the study from the synthesis and involved re-analyzing the data without the studies considered to be of low quality (CASP score <8 out of 10). There was only one study 20 that did not address more than two of the above-mentioned elements and could be considered of low quality. We found that our themes did not change, which means that the contribution of this study was minor to formation of the three main themes, as the main themes did not change after removing it.
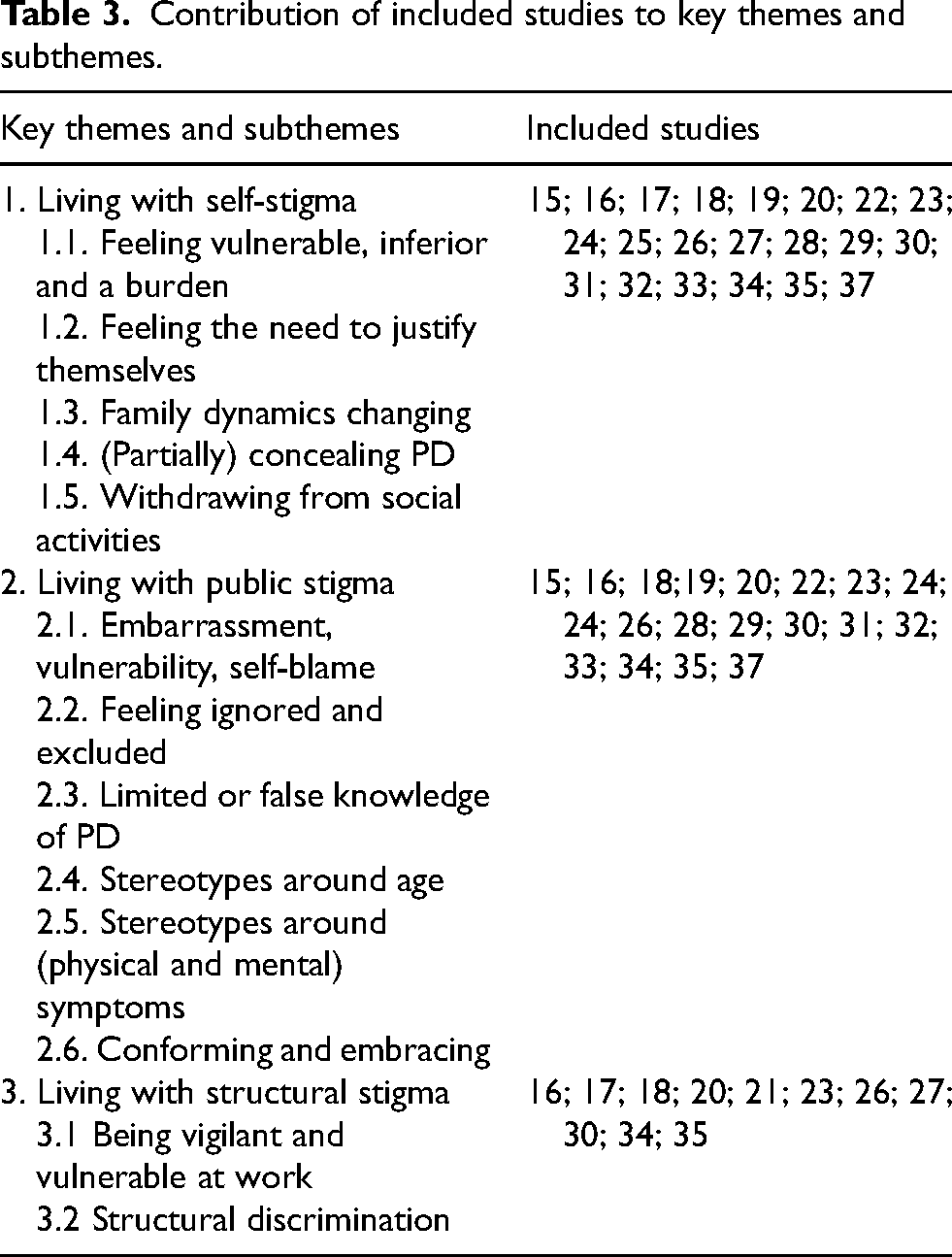
Contribution of included studies to key themes and subthemes.
Our review included papers that used different terms to refer to the type of stigma studied: family,15,26 social/public,15,17,24,26–28,30–33,35,36 self-stigma,15,19,23,27,33–35 structural stigma,15,19 internalized,16,19 anticipated,16,19 disability-related,15,16 work,16,17 perceived stigma,18,21,24,25,29,31 embodied/bodily,19,20 enacted, 19 secondary (associative) stigma, 19 (in)visible stigma21,22 and caregiver stigma. 31
Thematic synthesis
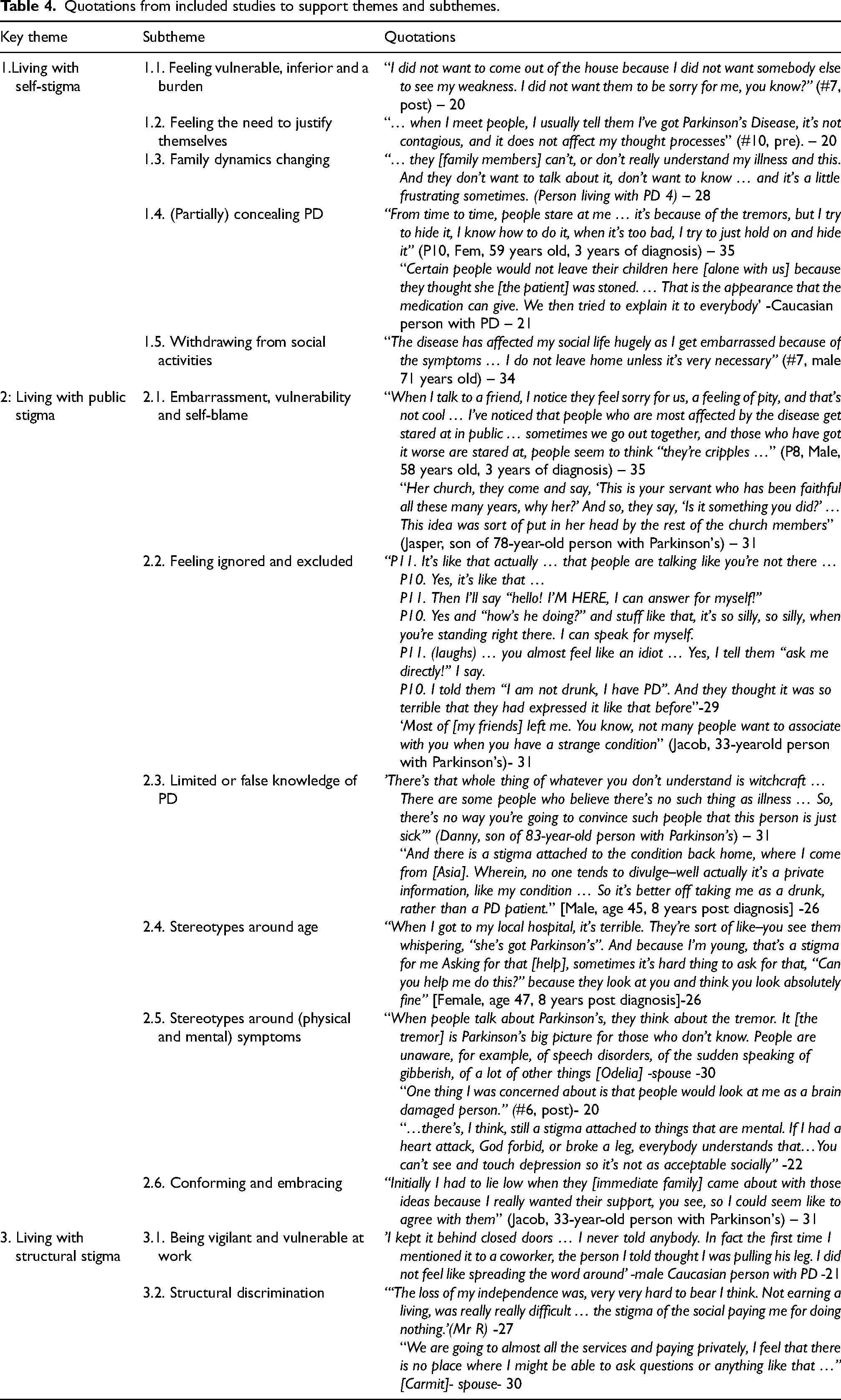
Three themes and several subthemes (Table 3) derived from the analysis of the included studies. Direct quotations from these studies were used to represent the key themes that are presented in Table 4 and explained below.
Quotations from included studies to support themes and subthemes.
THEME 1: Living with self-stigma
This theme presents the findings of how people living with PD experience stigma because of their own perceptions and beliefs. It also covers their behaviors and strategies (e.g., concealing, withdrawing) of managing their own stigma and family stigma.
Feeling vulnerable, inferior and a burden
A few studies16–18,20,36 reported that people with PD expressed feelings of embarrassment, being “weak”, 16 “inadequate”,28,34 “inferior”. 33 These feelings emerged by their inability to perform physical tasks, or their perception that others may feel pity or shame toward them due to their disease and dependence. Many studies19,31,34,35 reported loss of identity as participants with PD felt being a burden to their families, that they no longer ‘belonged’, being perceived as ‘cyborgs’, 20 ‘zombies’, 21 a ‘robot’, 36 ‘stoned’, 23 a ‘clod’ 34 or feeling odd and out of place. 32 As a result, people with PD felt ashamed and exposed to talk about personal experiences or mental health and had a great difficulty to ask for help.18,34
Feeling the need to justify themselves
Studies reported that people with PD with internalized stigma had to constantly negotiate other people's perceptions about their condition and ability, e.g., had to explain that they do not use their condition as an excuse for laziness, or undeserved special treatment.16,19 Some people with PD felt the need to justify their decisions to avoid being labelled as that “type of person” who uses disability as an excuse for obtaining undeserved rewards. 16 Furthermore, participants reported how fluctuations in symptoms (‘on’ and ‘off’ times) caused conflicting reports of the person's condition, which could further contribute to the belief that the person was pretending to be sick, lazy or avoid work potentially causing conflicts and misunderstandings19,36 leading to people making disparaging comments towards the person with PD. 34
Family dynamics changing
Studies15,17,19,23,31,32,34 reported that family members had not enough understanding of it, felt unease and/or maintained a certain distance from the person with PD. Facial masking was identified as one of the visible features that were reported as one potential reason. 21 This was a physical distance (for example, family members did not want to accompany them in various social situations) or emotional distance.
Family caregivers also talked of psychological burden and dependency on their relatives as a result of stopping work activities. 26 Other studies reported that some people with PD expressed worries of being abandoned by spouses or children when the disease progressed.19,34
(Partially) concealing PD
Studies reported that participants tried to hide the diagnosis from other people, from their work and/or even from their closest relatives.15,19,27 They were investing heavily in keeping the diagnosis a secret, especially in the early stages, when the symptoms were not visible15,19 or if the person was experiencing visual hallucinations. 28 This was explained as a self-protective behavior 20 and a need to fit in with social norms. 35 Apart from the diagnosis, some studies16,19,21,33 reported that people with PD tried to hide or make excuses for their physical (e.g., delayed reactions, slowed gait) or mental health symptoms.18,29 Participants used strategies to hide the tremor such as holding on to objects or hiding the hands.21,33 One study reported that caregivers noted situations where the person with PD would try to hide their symptoms, e.g., holding their hands in their lap to stop their tremor. 19 Concealing was easier for people with more discrete symptoms 19 and more evident for veterans who noted that military culture contributes to stigma regarding mental health and discomfort about being portrayed as “weak” when sharing about personal struggles. 18
Only later and when the physical symptoms and/or the effects of the medication were visible, they shared the diagnosis with wider circles.15,17,23 In some cases, it was necessary to avoid false perceptions (e.g., that the person was stoned). The concealment was not always mutually agreed by the person with PD and their main carers and was thought to be due to the fear of stigmatizing reactions in response to their disease.15,17
Withdrawing from social activities
Studies reported that people with PD chose to limit their social life.17,19,21,22,27,31 This was depending on their (ON/OFF) status 15 and due to their concerns or embarrassment about their symptoms, e.g., face masking.19,21,25,30,32,33 This decision was made to protect their self-image or avoid questions about their condition. Caregivers also mentioned social isolation as one strategy used by their relatives. 19 One study 27 noted that women especially restricted their social activities. Another study 32 reported that people with moderate PD were experiencing more stigma than those with mild or severe PD presumably because those with mild PD attracted less attention than those with moderate, whereas those having severe PD had learnt to cope with the increased attention.
Apart from social gatherings, stigma related to their medical and mental health symptoms may prevent some people with PD to avoid other aspects of social participation, 32 such as involvement in research 18 or engaging in physical activity24,30 if they believed that they may be judged by the public, which impacted their self-esteem and willingness to embrace their condition. 30 Family caregivers also reported social isolation as they could not go away from home to attend community activities (e.g., church) or visit friends and relatives. 26
THEME 2: Living with public stigma
Overall, this theme describes the public stigma that people living with PD experience because of public attitudes and behaviors. It described how it is experienced (e.g., feeling ignored), potential reasons (e.g., public's limited knowledge and stereotypes), and also ways people with PD respond to such stigma.
Embarrassment, vulnerability and self-blame
Some studies described how people with PD believed that their visible symptoms (e.g., tremors, drooling) attracted the attention of others in public, made them feel exposed and vulnerable.17,20,24,25,31,32,36 The progressive nature of PD made people feeling vulnerable due to emotional and physical changes and fear that future circumstances might worsen. Participants in three studies27,32,34 expressed that people perceived individuals living with PD differently and sometimes behave inappropriately towards them (e.g., staring, laughing at their odd gait and involuntary movement, making hurtful comments). The community misconceptions were also affecting behaviors and blame towards the people with PD creating a form of internalized, or self-blame.
Feeling ignored and excluded
Some studies discussed how people with PD were disregarded by others or felt discredited because of their condition, symptoms or treatments15,31,32 which was experienced as stigmatizing. Experiences of doctors' lack of training in clinical encounters were mentioned, where the physician delivered the diagnosis in an insensitive way, 33 avoided direct communication, ignored or spoke over them, and only communicated with the child or spouse of the person with PD. 15 Another study 28 reported that people with PD who were experiencing visual hallucinations were thought “crazy” and “not normal,” and that family or health professionals were unlikely to believe them. Harsh criticism, mocking and negative or mislabeled views (e.g., an alcoholic) were also reported by some studies.20–22 Other studies discussed how other people perceived them as lacking capacity and, in some instances, they had to explain that their judgement had not been affected by PD.
In addition, some studies15,19,31,34 reported that people (family, friends, strangers) kept social distance (e.g., being avoided on the street, excluded from social circles and communities). This resulted often in people with PD having a passive role with social encounters and clinical meetings15,33 probably due to feelings of shock and being overwhelmed. 34 People with PD tended to understand and forgive the family stigma (e.g., grandchildren's distancing), but less so the behaviors of their friends. 15
Limited or false knowledge of PD
Studies discussed how the complexities of PD were not well understood by the general public, especially when there was no visible tremor.30,31 Lacking valid information and having preconceptions about the disease was reported by many studies15,21,27,33,34 with some acknowledging that very few people had ever heard of PD and its potential causes, 26 with some people believing that PD was ‘contagious’ and feared contamination.15,19,20 Limited or false knowledge was reported not only from the public but also from the health professionals and family caregivers. 26
Socio-cultural factors also affect people's beliefs and attitudes towards PD. For example, in studies conducted in African countries (e.g., Kenya, Tanzania), increased stigma, misconceptions (jealousy) and supernatural beliefs (e.g., witchcraft) to explain the condition19,26 were reported due to poor awareness, lack of health policy and limited clinical capacity of neurological services. Younger patients questioned the cause of their illness more than others believing that they might have been bewitched or cursed or associated with taking things forcefully from other people. 26 In one study it was thought that PD was a bone related illness caused by cold weather. 26
Similar perceptions were reported by one study from the USA 23 where participants attributed their illness to spiritual reasons. One study 30 reported that people with PD from Asian ethnicity were experiencing stigma due to their cultural norms. Another study from Jordan 27 viewed the disease as a test from God. As a result of these beliefs, some people opted to use alternative therapies and traditional healers,19,26 instead of taking their prescribed medication.
Stereotypes around age
A major stigmatizing perception also reported by the studies was that PD cannot affect younger people as PD is a disease of “white”, “rich” or “old” people.15,19,21,26 Two main consequences were reported by studies15,19,27,30: (a) the perception that PD is a ‘normal’ old age illness could delay getting timely and proper care 26 and (b) younger people with PD could face more stigma, as a result of their being perceived by others as “abnormal”, while older people were expected to have some form of disability and that was perceived ‘normal’. Younger patients and those more recently diagnosed were more likely to experience stigmatizing behaviors, than older patients who had been living with the illness for some time 27 and some doctors dismissed them attributing their symptoms to old age. 35 Some younger participants said they were suffering from a disease of ‘older people’ when they should have been in their “youthful years”, being productive and “useful”, 19 often receiving hurtful comments 21 and not receiving suitable therapeutic programs to fit their needs. 33
Stereotypes around (physical and mental) symptoms
All studies reported that the stigma experienced by people with PD occurred due to the characteristics of the disease, mainly tremors, stiffness and difficulty walking. The limited public knowledge can often result in reducing PD in one symptom, mainly the tremors, embodying the whole nature of the disease. 15 People thought tremors as the main and even only symptom. This exaggerated emphasis on tremors by others could be explained due to their visibility or attributed to what people perceived as significant suffering,15,19 despite participants reporting that the tremors were thought less significant. 15 Similar experiences were documented in a study 20 exploring the stigma experienced by people with Deep Brain Stimulators, especially as the surgery can leave signs (e.g., scars) resulting in stigmatized perceptions (e.g., people seeing the scars, not the person).
This ‘narrow’ and false perception of PD excluding psychological symptoms was reported by studies18,20,21,27,28,33 that discussed stigma related to discussing mental health and non-motor symptoms of PD, e.g., depression and anxiety over diagnosis and over these physical symptoms20,21,27,28 and/or hallucinations. 29 One study 29 concluded that feeling “abnormal” prevented people with PD from discussing and seeking support for hallucinations, although some felt they were not important or that discussing them would not achieve anything. Gender and culture influenced how people with PD experienced their mental health and perceptions of others. Discussing treatments for mood symptoms was also of significant stigma,18,28 but it was acknowledged that discussing mental health, and the benefits of engaging in mental health care, was important toward addressing stigma.18,29
Conforming and embracing
Studies discussed the pressure individuals and families were under to conform to expectations and certain behaviors, or risk further stigmatizing perceptions and potential exclusion from the society.19,21 Some had to hide their symptoms, as discussed above, or put up with people's (false) imposed perceptions about them. The positive side of conforming was that it may have helped some people with PD to come to terms with their illness and be (passively) compliant to prescribed medications and recommended therapies.20,22,27,34,36 Experiences varied, with some people describing the acceptance process as a given process that they had to submit to (unavoidable acceptance), and others acknowledging that they had only partly accepted (acceptance in progress) the disease. 36 Only once they accepted the diagnosis, they started their medications, asked for help, managed people's stereotypes and improved their quality of life.27,30,31
THEME 3: Living with structural stigma
This theme reports the findings from studies that mentioned stigma manifested when the patient or caregiver had to interact in the wider society (e.g., workplace).
Being vigilant and vulnerable at work
Being in employment was seen as an important part of life and thus many people with PD wished to continue working, showing a sense of stigma associated with not working. 35 When discussing the stigma experienced in their employment, one study 16 reported that people with PD had to navigate both ableism and ageism, severely affecting their employment experiences and potentially their mental health.
Studies reported that disability-related stigma can be an employment barrier that affects employment experiences and expectations regarding current and future employment options.16,23 Some people with PD anticipated discrimination in the job market and shared examples when they were fired or pushed to resign or retire early.16,33,34 Others decided to hide their diagnosis fearing they would lose their jobs or having the stigma attached to PD.23,30,34 Disclosing personal information with work colleagues was not thought helpful, especially for people who continued working. Moreover, people with PD feared a loss of respect and being seen as less competent and more vulnerable to carry on with their employment. This fear of disability stigma acted as a barrier to disclosure for many participants, who tried to hide their symptoms to present ‘healthy’. Even those who disclosed their diagnosis, they continued to worry about being discriminated against. Studies16,17,21,33 also reported that people with PD anticipated discrimination (e.g., feeling watched “under a microscope” and judged) due to societal perceptions focused on physical appearance and as a result, they demonstrated a sense of vigilance. Participants who had experienced disability related and/or age-related discrimination and stigma expected to encounter continued discrimination.
Structural discrimination
One study reported how social systems may ignore the needs of individuals living with PD and the needs of their caregivers. 15 Some studies reported the unfair and unequal treatment that people with PD received from the governmental bodies (such as National Insurance Institutes) regarding (inappropriate) eligibility criteria for the care allowance, due to the way the requirements do not align with the progressive or unpredictable (ON/OFF condition) characteristics of the disease. 15 This may in turn result in unequal access to resources. Another study noted that people who received governmental support (statutory help) was also perceived to be stigmatizing.
As a result, people with PD and their caregivers had nowhere to get support.15,20,21,27,30 Many needed information and sought it on the internet, from the doctors or in clinic leaflets, but that was sometimes regarded as too generic, inconsistent or overwhelming.30,34 The lack of information during the diagnosis, the lack of support from clinicians and communication about the nature and management of PD and the lack of resources of valid information caused additional stress and made it harder to deal with the psychological shock of being diagnosed and living with PD.30,34 Lack of social and governmental support had emotional and financial impact.
Discussion
This review aimed to gather evidence on how people with PD and their carers experience stigma. We set out to understand what types of stigma they experience to deepen our understanding of the perceptions, experiences and meaning of stigma in people living with PD and their caregivers. As highlighted in the findings, the main types of stigma reported by the literature are: self, public and structural stigma. Lack of awareness, existing preconceptions and stereotypes about PD and limited education are factors that maintain public stigma, something that is confirmed by previous literature. 9 This review also highlighted the impact of these forms of stigma on people with PD and their families: withdrawing from social arena, hiding their diagnosis and symptoms, conforming to others’ beliefs, staying vigilant, expecting continuous discrimination and blaming themselves for their condition.
Overall, one third of the included studies (eight out of total 21 studies) included caregivers in their sample.15,17–19,23,26,29,31 Interestingly, our review did not find any study that reported experiences of stigma for family caregivers (“caregivers’ stigma”), and all reported very limited information around their experiences of stigma. The only study that included data only from caregivers, the authors concluded that the caregivers ‘shared experiences of the stigma attached to the illness and/or to their loved ones, but not to themselves’ and reported that some caregivers were acting as protectors and advocates for the person living with PD. 15 Even in the studies that included mixed sample (persons with PD and caregivers), they included themes around impact of PD on them (e.g., social isolation, balancing work and caring responsibilities, emotional impact) or drivers of stigma (e.g., lack of awareness), the stigmatic experience of the person with PD but not the caregivers.17,19,23,26,29 This could be partly explained given that in some studies caregivers were the minority of the sample, 31 the stigma experienced by caregivers was less compared to the person living with PD or perhaps the caregivers were more reluctant to share their experiences.
In this review we found that some stigmatizing behaviors were also driven by cultural beliefs. A previous review 38 examining a large spectrum of factors universally associated with stigma in PD also found that some factors affecting stigma in PD may differ depending on the specific culture.
The public's limited understanding of the complexity of neurological diseases is also prevalent in the dementia literature. Research on stigma and dementia also shows consistently limited knowledge, as well as stereotype, prejudice, and discrimination towards people with dementia and their family caregivers.39,40 According to the recent Editorial Lancet Neurology, [see 41 ] a third of respondents believed that people with dementia are dangerous, and two-thirds thought they are impulsive and unpredictable. About 40% thought the disease is caused by a lack of family support. Gathering evidence, running international campaigning, local and global advocacy 2 are some examples to fight dementia stigma, something that is still behind in PD communities.
Strengths and limitations
This is the first systematic review to present up-to-date evidence on stigma experienced by people living with PD. Included studies were published from 2004 to 2024, covering a period of 20 years of stigma research. Although all the included studies were published in English, some studies reported findings from seven different countries and our findings may be relevant to other countries and cultures. By incorporating international studies, we have provided compelling evidence to assist people with PD, their families, health and social care professionals in identifying several types of stigma and creating cultural appropriate interventions to tackle it.
One limitation of our review is that we included papers that explicitly mention ‘stigma’ in their aims and findings, which means we may have missed some literature. This decision was guided by our review question (which was focused on stigma) and also guided by our librarian's suggestions with expertise on the search terms (and explosion of such terms to include similar constructs where appropriate). The review team screened over 500 papers and expanded the search of relevant studies to look at reference lists from relevant published papers, other reviews, conference proceedings and theses to ensure that the search was focused but comprehensive.
Also, the subjective nature of qualitative research means that some issues may not have been reported or missed in the publications and/or in our synthesis. In addition, we decided to use the CASP tool albeit not designed for systematic reviews. Nevertheless, it helped us to become aware of the limitations of the included studies. Low score in quality assessment, and lack of information on methodological aspects might have affected the depth and relevance of the findings of these studies. However, our intention was not to exclude studies as we acknowledge that the information missing from these studies may have been due to other reasons (e.g., type of journal, journals’ word restrictions) and not necessarily due to lack of robust methodology. 37 Our sensitivity analysis confirmed that the final themes were not affected significantly after removing the ‘low-quality’ study from our analysis.
Implications for practitioners
This study provides a comprehensive synthesis of qualitative research on stigma in PD, a topic that has been explored in individual studies but not systematically reviewed with a thematic approach. By identifying three primary dimensions of stigma (self-stigma, public stigma, and structural stigma), this review extends the findings from a previous scoping review 8 and deepens our understanding of how stigma manifests and affects individuals with PD and their caregivers.
Unlike previous studies that may have focused on single aspects of stigma or specific cultural populations, this review integrates findings from diverse international contexts and highlights the urgent need for empirically tested educational interventions to address misconceptions and discrimination. Furthermore, it emphasizes the importance of tailored support strategies for individuals at different stages of PD and underscores the need for future research to expand globally and include caregivers’ experiences. By synthesizing these qualitative insights, our study provides valuable implications for healthcare professionals, policymakers, and researchers, guiding the development of more inclusive, stigma-reducing interventions that could improve the social and psychological well-being of individuals living with PD.
Although our findings are unlikely to be applicable to all people with PD and their families, they could provide the basis for educational materials to tackle stigma and promote interventions to raise public awareness. This is urgently needed as there is a significant lack of empirically tested educational resources to change stereotypes about PD. Public knowledge and attitudes remain variable across the globe, potentially contributing to social marginalization of this group within their communities. 9 When designing PD interventions health and social care professionals should be mindful of the age, stage, meanings, preferences and readiness of the patient. Individually tailored assessment and support could enable people with PD to stay socially active, remain at work, avoid social exclusion and mental health problems. Future research should expand on more countries and focus on the co-development of interventions to promote public knowledge of PD internationally. It should also examine how stigma is experienced by caregivers as there is limited qualitative research.
Conclusions
Our review offers most up-to-date knowledge on PD and stigma. It particularly notes the stigma of being diagnosed with a condition typically associated with older age, and cultural beliefs and challenges encountered with employment amongst other significant issues. It also underscores the importance of recognizing the nuanced ways in which stigma can impact PD experiences to facilitate the development of targeted interventions, policies, and evidenced-educational initiatives that address the multifaceted challenges associated with stigma in PD.
Footnotes
Acknowledgement
We are grateful to Mrs María Jesús Manzano Mulet for her support with the database searches.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Dia Soilemezi was a Visiting Professor at the University of the Balearic Islands during the research carried for this review.
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during this review. The data supporting the findings of this review are openly available in the public domain and all articles cited in this manuscript are included in the reference list.